 Anatomy, Head and Neck: Eye Medial Rectus Muscles
Anatomy, Head and Neck: Eye Medial Rectus Muscles
Introduction
Extraocular muscles are responsible for controlling eye movements, maintaining proper eye alignment, and moving the upper eyelids. These muscles work in pairs to move the eyes in various directions. The following are the 7 extraocular muscles:[1][2][3][4]
- Superior rectus muscle
- Inferior rectus muscle
- Medial rectus muscle
- Lateral rectus muscle
- Superior oblique muscle
- Inferior oblique muscle
- Levator palpebrae superioris muscle
Each of these muscles plays a specific role in moving the eye, and their coordinated actions allow for smooth and precise eye movements. Nerve palsies or muscle lesions can impair eye movements and make it difficult for a person to fixate on objects in their field of vision. The medial rectus muscle is primarily responsible for eye adduction, which means it moves the eye medially.
This article discusses the medial rectus.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The medial rectus is an adductor muscle. It moves the eye from side to side with the lateral rectus, an abductor. The globe can rotate 50° horizontally from the anterior midline. However, normal extraocular muscle movement can be limited to only 15° when the head moves.
Each extraocular muscle has a functional insertion point at the closest point where the muscle first contacts the globe. This point forms a tangential line from the globe to the muscle origin, known as the arc of contact. The medial rectus has an arc of contact of 7 mm, whereas the lateral rectus has an arc of contact of 12 mm.
Embryology
Head mesenchyme, which gives rise to the orbit and its structures, forms primarily from the mesoderm and the neural crest. The extraocular muscle fibers originate from the mesoderm, but the muscles' satellite and connective tissues arise from neural crest cells.
Blood Supply and Lymphatics
The arterial supply to the extraocular muscles comes from the muscular branches of the ophthalmic artery, which has a small superior branch and a large inferior branch. The superior branch supplies the lateral rectus, superior rectus, superior oblique, and levator palpebrae superioris. The inferior branch of the ophthalmic artery supplies the medial rectus, inferior rectus, and inferior oblique. The lateral rectus muscle is also partly supplied by the lacrimal artery.
Venous drainage is similar to the arterial system and empties into the superior and inferior orbital veins. Usually, there are a total of 4 vortex veins located at the lateral and medial sides of the superior and inferior rectus muscles.
Nerves
The lower division of the oculomotor nerve (cranial nerve III) innervates the medial rectus. The oculomotor nerve is divided into the superior and inferior divisions. The superior division innervates the superior rectus and levator palpebrae superioris. The inferior division supplies the medial rectus, inferior rectus, and inferior oblique. The abducens nerve (cranial nerve VI) innervates the lateral rectus. The trochlear nerve (cranial nerve IV) innervates the superior oblique.
Muscles
The rectus muscles originate posteriorly from the Annulus of Zinn, coursing anteriorly before inserting on the globe. The medial and lateral recti make up the horizontal rectus muscles. The superior and inferior recti form the vertical rectus muscles.
The recti insert on the globe at varying distances from the limbus.
- Medial rectus: Inserts at 5.5 mm from the limbus
- Inferior rectus: Inserts at 6.5 mm from the limbus
- Lateral rectus: Inserts at 6.9 mm from the limbus
- Superior rectus: Inserts at 7.7 mm from the limbus
The Spiral of Tillaux is the imaginary line connecting the recti's insertion points.
The medial rectus travels along the medial orbital wall. On average, it is 10.3 mm wide at its insertion point and 40.8 mm long. The mean length of the medial rectus tendon is 3.7 mm.
Extraocular muscles have a large ratio of nerve fibers to skeletal muscle fibers—1:3 to 1:5—whereas other skeletal muscles have 1:50 to 1:125. Extraocular muscles are specialized skeletal muscles, having many fiber types like slow, fatigue-resistant tonic types and rapid, saccadic types.
Physiologic Variants
The size, insertion distance, and other features of the medial rectus muscle vary widely. Ocular misalignment can arise from congenital extraocular muscle anomalies.[5][6][7][8]
Surgical Considerations
The potential complications of extraocular muscle surgery include the following:
- Unsatisfactory alignment is the most common, though it can be surgically repaired.
- Refractive changes can occur after surgery involving two rectus muscles in the same orbit but may resolve within months.
- The nerves to the rectus and superior oblique muscles insert around a third of the distance from the origin to the insertion point. Damage to these nerves during anterior segment surgery is difficult but not impossible. However, advancing instruments 26 mm posterior to the rectus muscle insertions can injure the nerves.
- The arteries supplying the extraocular muscles anastomose with those of the globe's anterior segment. Extraocular muscle surgery may compromise orbital circulation.
- The Tenon capsule is an elastic connective tissue that attaches to the optic nerve posteriorly and is pierced by all the extraocular muscles except the levator palpebrae superioris. Surgical instruments inserted 10 mm posterior to the limbus can injure the Tenon capsule, causing prolapse of the surrounding adipose tissue and adhesions around the extraocular muscles (see Image. The Extraocular Muscles).
- Other possible surgical complications of extraocular muscle surgery include diplopia, scleral perforation, and postoperative infections. Although uncommon, serious infections, such as pre-septal or orbital cellulitis and endophthalmitis, may occur after strabismus surgery.
Clinical Significance
Extraocular muscle function testing can be assessed by having the patient look in nine directions.
- Primary gaze: both the head and eyes are oriented toward the anterior midline
- Secondary positions: superior, inferior, left, and right
- Tertiary positions: superior right quadrant, superior left quadrant, inferior right quadrant, and inferior left quadrant
The patient follows the clinician's finger as it starts from the primary gaze and then traces a wide letter "H" in the air.
Other tests for ocular alignment include:
- Cover test
- Corneal light reflex test
- Dissimilar image test
- Dissimilar target test
Many patients with extraocular muscle abnormalities are young children. Toys and other visually attractive objects can help elicit young children's cooperation.
Strabismus or ocular misalignment can be caused by binocular vision or neuromuscular abnormalities.
Esotropia is a condition where the cornea deviates nasally. Comitant esotropia is present when the extent of eye deviation does not change with gaze direction. In contrast, incomitant esotropia is characterized by eye deviation severity changing with gaze orientation. One cause of incomitant esotropia is a medial rectus palsy or lesion, which may arise from thyroid myopathy, medial orbital wall fracture, Duane syndrome, or excessive medial rectus muscle resection.
Other Issues
A-pattern and V-pattern strabismus are horizontally oriented, and they can be corrected by vertically transposing the rectus muscles. For A-pattern deviations, the medial rectus is moved superiorly along the globe toward the location of the deviation. In V-pattern deviations, the medial rectus is moved inferiorly toward the deviation. These procedures weaken the muscle pulling toward the direction of the deviation. Full treatment plans for these conditions depend on the function of the other extraocular muscles, especially the superior and inferior obliques. Postoperative assessment of overaction or underaction is crucial.
Media
(Click Image to Enlarge)
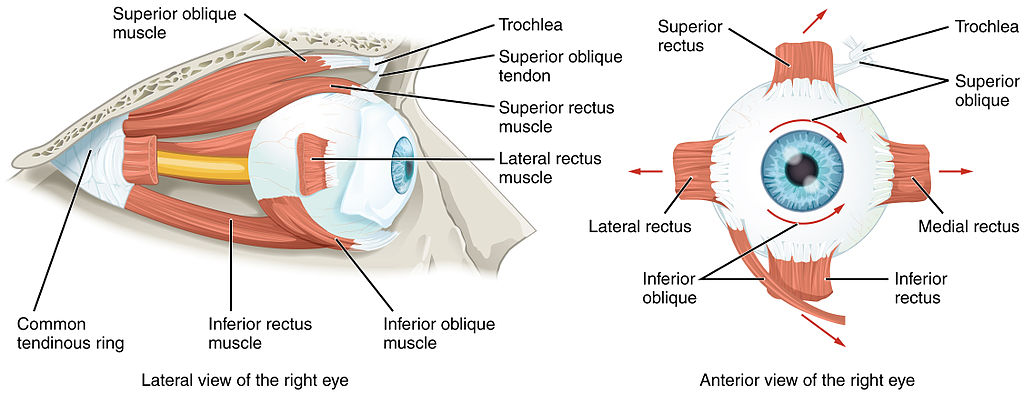
The Extraocular Muscles. Left: Lateral view of the right eyeball. Right: Anterior view of the right eyeball. Muscle insertion points are shown.
By OpenStax College [CC BY 3.0 (https://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons
References
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Orbit Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 30285385]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck: Eye Superior Rectus Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30252323]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Eye Extraocular Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30137849]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck: Eye Inferior Rectus Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30085520]
Bird B, Stawicki SP. Anatomy, Head and Neck, Ophthalmic Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 29493942]
Kono R, Ohtsuki H, Kishimoto F, Hamasaki I, Morizane Y, Shiraga F. Magnetic resonance imaging findings of age-related distance esotropia in Japanese patients with high myopia. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2019 Mar:257(3):657-662. doi: 10.1007/s00417-019-04250-0. Epub 2019 Jan 22 [PubMed PMID: 30671656]
Shin HJ, Lee SH, Ha TJ, Song WC, Koh KS. Intramuscular Nerve Distribution in the Medial Rectus Muscle and Its Clinical Implications. Current eye research. 2019 May:44(5):522-526. doi: 10.1080/02713683.2018.1562556. Epub 2019 Feb 27 [PubMed PMID: 30624996]
Demer JL, Clark RA. Functional anatomy of human extraocular muscles during fusional divergence. Journal of neurophysiology. 2018 Nov 1:120(5):2571-2582. doi: 10.1152/jn.00485.2018. Epub 2018 Sep 19 [PubMed PMID: 30230991]