Introduction
Mumps, once a common childhood disease, is a contagious viral illness. With the widespread vaccination, the incidence of mumps has decreased substantially. Mumps typically presents with a prodrome of headache, fever, fatigue, anorexia, and malaise, followed by the classic hallmark of the disease, parotitis.[1] The disease is typically self-limited, with most patients experiencing a full recovery.
Mumps is caused by the rubulavirus, which belongs to the Paramyxoviridae family.[2] Mumps affects individuals globally and is the only known cause of epidemic parotitis. The majority of mumps cases in temperate zones are observed during late winter and early spring.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Mumps is caused by a single-stranded RNA paramyxovirus. Nucleoprotein, phosphoprotein, and polymerase together with the genomic RNA facilitate the replication of the virus, leading to the formation of the nucleocapsid. A host-derived lipid bilayer surrounds the nucleocapsid (see Image. Paramyxovirus Virion Under Transmission Electron Microscope). Within this lipid bilayer are viral neuraminidase and fusion proteins, which allow cell binding and virus entry. These fusion complexes are the main targets of virus-neutralizing antibodies.[1] To date, 12 mumps genotypes have been identified.[4] Genotype G has been the primary mumps virus genotype circulating in the United States since 2006.[5]
Risk factors for mumps include immunodeficiency, international travel, living in a crowded or close-knit setting, and lack of vaccination.[3]
Epidemiology
Mumps is endemic worldwide with epidemic outbreaks occurring approximately every 5 years in unvaccinated regions. The mumps virus is highly infectious and transmissible through direct contact with respiratory droplets, saliva, and household fomites. Up to one-third of infected individuals exhibit no symptoms but are contagious.
The incidence of mumps in the United States dropped by 99% after the mumps vaccine was introduced in 1967.[6] Nonetheless, several significant mumps outbreaks have occurred in the United States, Canada, and Europe since the mid-2000s.[2] Before the widespread use of mumps-containing vaccines, mumps predominantly occurred in young school-aged children. However, with routine vaccination of preschool and school-aged children, mumps outbreaks in the 21st century now primarily affect adolescents and young adults.
Several factors have likely contributed to the recent increase in mumps outbreaks, including declining vaccine coverage rates, failure to complete the two-dose series, historical use of less-effective vaccine strains in some European countries, and removal of mumps vaccine from the routine schedule in Japan and other countries.[1] Recent outbreaks among fully vaccinated college students have suggested that immunity to mumps may wane over time.[7] A 2006 study of a significant mumps outbreak in a university with high vaccine coverage rates found that students vaccinated 13 or more years before the outbreak were 9 times more susceptible to mumps compared to students who had been vaccinated less than 2 years before the outbreak.[5] In addition, many behaviors that can contribute to mumps transmission are common among college and university students, such as living in shared housing, prolonged face-to-face contact with other students, and exchange of saliva with other people.[8]
Pathophysiology
Humans are the only natural hosts for the mumps virus.[2] Mumps has a variable incubation period of 12 to 25 days. Individuals are contagious from 2 days before the onset of symptoms through 5 days after onset.[1] Primary replication occurs in the upper airway mucosal epithelium. Infection of mononuclear cells in regional lymph nodes promotes viremia, resulting in systemic inflammation in the salivary glands, testes, ovaries, pancreas, mammary glands, and the central nervous system.[4]
History and Physical
The prodrome of the mumps virus includes nonspecific symptoms such as fever, malaise, headache, myalgia, and anorexia, shortly followed by parotitis in the subsequent days. Mumps parotitis is the most common manifestation of the virus, occurring in over 70% of infections. Parotid swelling is typically bilateral, but unilateral swelling can occur. Parotid swelling presents as painful inflammation of the area between the earlobe and the angle of the mandible (see Image. Mumps Parotitis in a Pediatric Patient). The mucosa of the Stensen duct is often red and swollen along with the involvement of the submaxillary and submandibular glands. Glandular inflammation most often presents but then subsides within 1 week. Recurrent sialadenitis may occur as a complication of parotitis.
Orchitis is the next most common manifestation of mumps, characterized by unilateral or bilateral painful swelling, enlargement, and tenderness of the testes. Testicular atrophy develops in one-half of those affected. Infertility or subfertility may occur in up to 30% of cases of mumps orchitis among post-pubertal males but rarely occurs in pre-pubertal boys.[4] Oophoritis is a rare complication among infected post-pubertal females.
Neurological manifestations include meningitis, encephalitis, transverse myelitis, Guillain–Barré syndrome, cerebellar ataxia, facial palsy, and hydrocephalus. Neurological complications are typically self-resolving, and a low incidence of morbidity and mortality is expected.[9] Additional rare complications include pancreatitis, mastitis, myocarditis, thyroiditis, nephritis, hepatic disease, arthritis, keratitis, and thrombocytopenia.[7][10]
Research findings regarding the impact of maternal mumps infection on neonatal outcomes are inconsistent.[1][6] Although some early studies reported increased rates of spontaneous abortion following first-trimester mumps infection, more recent research found no higher rates of spontaneous abortion nor premature birth following mumps infection during pregnancy.[11][12]
Evaluation
Clinical observation and laboratory testing confirm a mumps infection. Not all mumps cases classically display orchitis and parotitis, and individuals may present heterogeneously. During an outbreak, the diagnosis is clinical in cases of parotid swelling with a history of exposure. When the local incidence is low, other infectious and noninfectious causes of parotitis warrant investigation.
Mumps laboratory confirmation techniques include reverse transcriptase-polymerase chain reaction (RT-PCR) and serum immunoglobulin M (IgM) antibodies. At the initial presentation of an individual suspected of mumps infection, the treating clinician should collect 2 specimens: a buccal or oral swab for RT-PCR and an acute-phase serum specimen for IgM and IgG antibodies. Ideally, buccal specimens should be obtained within 3 days of parotid gland swelling and no later than 8 days after symptom onset. Massaging the parotid gland 30 seconds before buccal swab collection can improve specimen quality. The IgM response may not be detectable for up to 5 days after the onset of symptoms in unvaccinated individuals and may not be detectable in vaccinated people.[1] Incorrect collection of acute-phase samples can lead to false-negative results. When this occurs, repeat serum samples should be collected 7 to 10 days after the onset of symptoms to yield positive results.[6]
Clinicians treating patients with suspected or confirmed mumps should notify their local or state health authority according to their state's public health laws and regulations.[13]
Treatment / Management
Mumps is typically a benign illness that is self-resolving. Treatment primarily involves providing supportive care for the symptoms presented. Analgesic medications and cold or warm compresses for parotid swelling are beneficial. Testicular swelling and tenderness should be treated with elevation and cold compression. No proven benefit for glucocorticoid use is demonstrated for mumps orchitis.[4] A therapeutic lumbar puncture may relieve a headache associated with aseptic meningitis due to mumps viral infection.[6]
Patients with mumps should undergo droplet precautions and remain isolated for 5 days after the onset of parotid swelling to minimize the risk of mumps transmission.[14]
Differential Diagnosis
Mumps is the most common cause of childhood parotitis. A classic presentation of parotitis during a mumps outbreak may be presumptively diagnosed based on clinical presentation. However, clinicians should consider other potential etiologies when symptoms are atypical or when the patient has not recently been exposed to mumps. The differential diagnosis may vary depending on the patient's symptoms and signs.
Acute parotitis
- Other viral causes such as Epstein-Barr virus, influenza A virus, parainfluenza virus types 1 and 3, and enteroviruses
- Suppurative parotitis such as Staphylococcus aureus, Streptococcus species, and atypical mycobacteria
- Noninfectious causes such as sialolithiasis, drug reaction, and malignancy
- Other causes of facial swelling that may mimic parotitis such as lymphoma, mastoiditis, and dental abscess [1][6][15]
Aseptic meningitis
- Other viral causes such as enteroviruses, herpes simplex virus, and lymphocytic choriomeningitis virus
- Noninfectious causes such as Kawasaki disease, malignancy, and drug reaction
Orchitis in isolation is typically caused by mumps, but orchitis can co-occur with epididymitis or cause symptoms similar to those of testicular torsion.[16][17]
Prognosis
The prognosis for a patient with mumps is typically excellent. After aseptic meningitis, recovery is generally complete.[3] Deafness can occur after mumps but is also rare.[1]
Complications
In the pre-vaccine era, complications of mumps were estimated to occur in up to half of males and 25% of females infected with mumps. Orchitis was the most common complication among males, occurring in about 1 in 5 cases of mumps among males, whereas aseptic meningitis was the most prevalent mumps complication across genders.[18][19]
Studies of mumps outbreaks in the modern area have consistently reported lower rates of complications compared to those reported in the prevaccine era, suggesting that high levels of community-wide vaccination may protect against more severe mumps infections.[20] Comparative studies of complication rates among vaccinated and unvaccinated populations have been limited by low numbers of unvaccinated children in the United States. However, a study conducted during a large multi-year mumps outbreak in Israel found statistically significantly lower rates of complications and hospitalization among vaccinated people infected with mumps compared to unvaccinated cases.[21]
Nonetheless, complications of mumps can still occur among vaccinated people, including orchitis, oophoritis, meningitis, encephalitis, sensorineural hearing loss, mastitis, and pancreatitis.[7][8][10]
Deterrence and Patient Education
As clinicians in this era of the anti-vaccination movement, advocating the benefits of the measles-mumps-rubella (MMR) vaccine is vital. The resurgence of mumps outbreaks is preventable with proper patient education by clinicians from all spectrums of practice. Nurses, pharmacists, and other healthcare professionals should repeatedly encourage caregivers to get their children vaccinated against mumps.
The mumps vaccine is available in the United States as part of a trivalent MMR vaccine. This vaccine is administered in 2 doses, with the first dose given to children at the age of 1 and the second dose typically administered between the ages of 4 and 6. Children and adults without documented immunity to measles, mumps, and rubella should receive catch-up MMR vaccination as soon as possible unless they have a contraindication to the vaccine. The second dose can be given as soon as 28 days after the first dose.
A 2019 Cochrane Review evaluating vaccines for measles, mumps, rubella, and varicella revealed that a single dose of the MMR vaccine is around 72% effective in preventing mumps, and its efficacy rises to 86% after the second dose. The most common adverse effects of the MMR vaccine are fever, rash, transient lymphadenopathy, and transient parotitis. Febrile seizures may occur after the MMR vaccine in about 1 in 1000 to 1 in 2000 children younger than 5. No evidence of a causal association between the MMR vaccine and autism spectrum disorder is recognized.[22]
The mumps vaccine is a live-attenuated virus. The vaccine should not be administered to pregnant women, and women are advised to wait 4 weeks after MMR vaccination before attempting to conceive. Vaccination is recommended in women who are breastfeeding along with children and other household contacts of pregnant women. Individuals with life-threatening allergic reactions to components of the vaccine or those with significant immunosuppression are not candidates for vaccination. This includes patients with AIDS, leukemia, lymphoma, generalized malignancy, and those receiving treatment with chemotherapy, radiation, or corticosteroid therapy. Household contacts to individuals with severe immunosuppression should be vaccinated. AIDS or HIV patients who have signs of immunosuppression should not be vaccinated, but patients with HIV who do not have laboratory evidence of immunosuppression should be vaccinated.[23]
In 2018, the Centers for Disease Control (CDC) recommended that individuals previously vaccinated with 2 doses of MMR vaccine who are identified by a public health authority as being at increased risk during a population outbreak should receive a third dose of MMR vaccine to provide them with additional protection during the outbreak.[5] This recommendation is based on data from 3 studies that evaluated the use of a third dose of MMR vaccine to control mumps outbreaks. Collectively, these 3 studies estimated that individuals who received a third dose of MMR during a mumps outbreak had a 61% to 88% lower attack rate compared to those with 2 doses.[24][25][26] Adverse events following a third dose of MMR vaccine were similar to or less than those observed following a second dose.[27]
Healthcare professionals should alert parents about the risks associated with not vaccinating their children against mumps. In November 2023, the CDC reported that MMR vaccine coverage rates among children in U.S. kindergartens had dropped below the Healthy People 2030 target for the third consecutive year. Declining rates of childhood vaccination raise the risk of vaccine-preventable disease outbreaks.[28] Prevention with vaccination is the most practical and effective control measure against mumps.
Enhancing Healthcare Team Outcomes
A single case of mumps can lead to an outbreak in a community with low MMR vaccine coverage rates or with close and prolonged contact.[5] Although the infection is rarely life-threatening, it can cause considerable morbidity if the testes or ovaries are affected.[23]
When a mumps case is diagnosed, the local authorities should be notified.[13] Clinicians should educate patients with mumps and their close contacts on hand washing, respiratory hygiene, signs and symptoms of potential adverse effects, and the need for isolation or quarantine, as appropriate.[29] Public health nurses should monitor these patients for complications and refer all patients with symptoms to the primary care clinician. A coordinated educational approach between clinicians helps prevent the spread of this disease. Patients and caregivers must be educated that the vaccine is safe and that adverse reactions are rare. An interprofessional approach to prevention, evaluation, and treatment is essential for successfully resolving a mumps outbreak.[8]
Media
(Click Image to Enlarge)
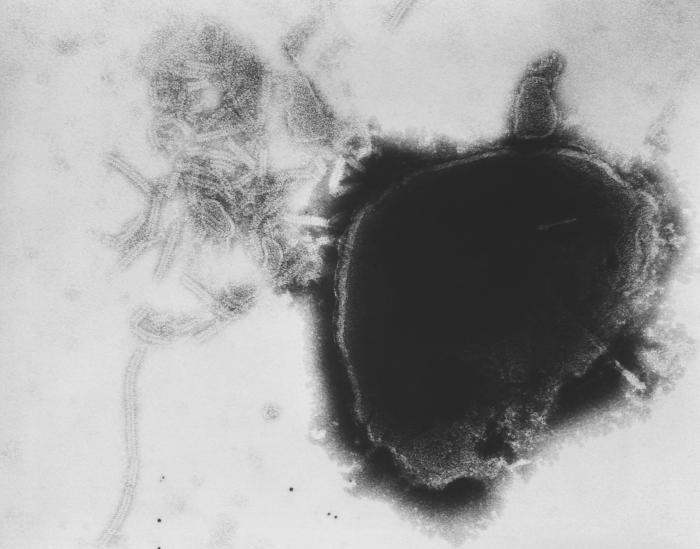
Paramyxovirus Virion Under Transmission, Electron Microscope. The image displays the viral nucleocapsid of a paramyxovirus virion as visualized under a transmission electron microscope.
Fred Murphy, MD, Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)

Mumps Parotitis in a Pediatric Patient. Parotid swelling presents as painful inflammation of the area between the earlobe and the angle of the mandible.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
References
Lam E, Rosen JB, Zucker JR. Mumps: an Update on Outbreaks, Vaccine Efficacy, and Genomic Diversity. Clinical microbiology reviews. 2020 Mar 18:33(2):. doi: 10.1128/CMR.00151-19. Epub 2020 Feb 26 [PubMed PMID: 32102901]
Almansour I. Mumps Vaccines: Current Challenges and Future Prospects. Frontiers in microbiology. 2020:11():1999. doi: 10.3389/fmicb.2020.01999. Epub 2020 Aug 20 [PubMed PMID: 32973721]
Su SB, Chang HL, Chen AK. Current Status of Mumps Virus Infection: Epidemiology, Pathogenesis, and Vaccine. International journal of environmental research and public health. 2020 Mar 5:17(5):. doi: 10.3390/ijerph17051686. Epub 2020 Mar 5 [PubMed PMID: 32150969]
Wu H, Wang F, Tang D, Han D. Mumps Orchitis: Clinical Aspects and Mechanisms. Frontiers in immunology. 2021:12():582946. doi: 10.3389/fimmu.2021.582946. Epub 2021 Mar 18 [PubMed PMID: 33815357]
Marin M, Marlow M, Moore KL, Patel M. Recommendation of the Advisory Committee on Immunization Practices for Use of a Third Dose of Mumps Virus-Containing Vaccine in Persons at Increased Risk for Mumps During an Outbreak. MMWR. Morbidity and mortality weekly report. 2018 Jan 12:67(1):33-38. doi: 10.15585/mmwr.mm6701a7. Epub 2018 Jan 12 [PubMed PMID: 29324728]
Hviid A, Rubin S, Mühlemann K. Mumps. Lancet (London, England). 2008 Mar 15:371(9616):932-44. doi: 10.1016/S0140-6736(08)60419-5. Epub [PubMed PMID: 18342688]
Shepersky L, Marin M, Zhang J, Pham H, Marlow MA. Mumps in Vaccinated Children and Adolescents: 2007-2019. Pediatrics. 2021 Dec 1:148(6):. pii: e2021051873. doi: 10.1542/peds.2021-051873. Epub [PubMed PMID: 34814181]
Shah M, Quinlisk P, Weigel A, Riley J, James L, Patterson J, Hickman C, Rota PA, Stewart R, Clemmons N, Kalas N, Cardemil C, Iowa Mumps Outbreak Response Team. Mumps Outbreak in a Highly Vaccinated University-Affiliated Setting Before and After a Measles-Mumps-Rubella Vaccination Campaign-Iowa, July 2015-May 2016. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2018 Jan 6:66(1):81-88. doi: 10.1093/cid/cix718. Epub [PubMed PMID: 29020324]
RUSSELL RR, DONALD JC. The neurological complications of mumps. British medical journal. 1958 Jul 5:2(5087):27-30 [PubMed PMID: 13546635]
Dayan GH, Quinlisk MP, Parker AA, Barskey AE, Harris ML, Schwartz JM, Hunt K, Finley CG, Leschinsky DP, O'Keefe AL, Clayton J, Kightlinger LK, Dietle EG, Berg J, Kenyon CL, Goldstein ST, Stokley SK, Redd SB, Rota PA, Rota J, Bi D, Roush SW, Bridges CB, Santibanez TA, Parashar U, Bellini WJ, Seward JF. Recent resurgence of mumps in the United States. The New England journal of medicine. 2008 Apr 10:358(15):1580-9. doi: 10.1056/NEJMoa0706589. Epub [PubMed PMID: 18403766]
Siegel M, Fuerst HT, Peress NS. Comparative fetal mortality in maternal virus diseases. A prospective study on rubella, measles, mumps, chicken pox and hepatitis. The New England journal of medicine. 1966 Apr 7:274(14):768-71 [PubMed PMID: 17926883]
Level 2 (mid-level) evidenceEnders M, Rist B, Enders G. [Frequency of spontaneous abortion and premature birth after acute mumps infection in pregnancy]. Gynakologisch-geburtshilfliche Rundschau. 2005 Jan:45(1):39-43 [PubMed PMID: 15644639]
Level 2 (mid-level) evidenceMcNabb SJ, Jajosky RA, Hall-Baker PA, Adams DA, Sharp P, Anderson WJ, Javier AJ, Jones GJ, Nitschke DA, Worshams CA, Richard RA Jr, Centers for Disease Control and Prevention (CDC). Summary of notifiable diseases --- United States, 2005. MMWR. Morbidity and mortality weekly report. 2007 Mar 30:54(53):1-92 [PubMed PMID: 17392681]
Centers for Disease Control and Prevention (CDC). Updated recommendations for isolation of persons with mumps. MMWR. Morbidity and mortality weekly report. 2008 Oct 10:57(40):1103-5 [PubMed PMID: 18846033]
Brook I. Diagnosis and management of parotitis. Archives of otolaryngology--head & neck surgery. 1992 May:118(5):469-71 [PubMed PMID: 1571113]
Wright WF, Pinto CN, Palisoc K, Baghli S. Viral (aseptic) meningitis: A review. Journal of the neurological sciences. 2019 Mar 15:398():176-183. doi: 10.1016/j.jns.2019.01.050. Epub 2019 Jan 31 [PubMed PMID: 30731305]
Trojian TH, Lishnak TS, Heiman D. Epididymitis and orchitis: an overview. American family physician. 2009 Apr 1:79(7):583-7 [PubMed PMID: 19378875]
Level 3 (low-level) evidencethe Association for the Study of Infectious Disease. A retrospective survey of the complications of mumps. The Journal of the Royal College of General Practitioners. 1974 Aug:24(145):552-6 [PubMed PMID: 4465449]
Level 2 (mid-level) evidenceGray JA. Mumps. British medical journal. 1973 Feb 10:1(5849):338-40 [PubMed PMID: 4685627]
Barskey AE, Schulte C, Rosen JB, Handschur EF, Rausch-Phung E, Doll MK, Cummings KP, Alleyne EO, High P, Lawler J, Apostolou A, Blog D, Zimmerman CM, Montana B, Harpaz R, Hickman CJ, Rota PA, Rota JS, Bellini WJ, Gallagher KM. Mumps outbreak in Orthodox Jewish communities in the United States. The New England journal of medicine. 2012 Nov 1:367(18):1704-13. doi: 10.1056/NEJMoa1202865. Epub [PubMed PMID: 23113481]
Zamir CS, Schroeder H, Shoob H, Abramson N, Zentner G. Characteristics of a large mumps outbreak: Clinical severity, complications and association with vaccination status of mumps outbreak cases. Human vaccines & immunotherapeutics. 2015:11(6):1413-7. doi: 10.1080/21645515.2015.1021522. Epub [PubMed PMID: 25874726]
Level 3 (low-level) evidenceDi Pietrantonj C, Rivetti A, Marchione P, Debalini MG, Demicheli V. Vaccines for measles, mumps, rubella, and varicella in children. The Cochrane database of systematic reviews. 2021 Nov 22:11(11):CD004407. doi: 10.1002/14651858.CD004407.pub5. Epub 2021 Nov 22 [PubMed PMID: 34806766]
Level 1 (high-level) evidenceMcLean HQ, Fiebelkorn AP, Temte JL, Wallace GS, Centers for Disease Control and Prevention. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2013 Jun 14:62(RR-04):1-34 [PubMed PMID: 23760231]
Ogbuanu IU, Kutty PK, Hudson JM, Blog D, Abedi GR, Goodell S, Lawler J, McLean HQ, Pollock L, Rausch-Phung E, Schulte C, Valure B, Armstrong GL, Gallagher K. Impact of a third dose of measles-mumps-rubella vaccine on a mumps outbreak. Pediatrics. 2012 Dec:130(6):e1567-74. doi: 10.1542/peds.2012-0177. Epub 2012 Nov 5 [PubMed PMID: 23129075]
Nelson GE, Aguon A, Valencia E, Oliva R, Guerrero ML, Reyes R, Lizama A, Diras D, Mathew A, Camacho EJ, Monforte MN, Chen TH, Mahamud A, Kutty PK, Hickman C, Bellini WJ, Seward JF, Gallagher K, Fiebelkorn AP. Epidemiology of a mumps outbreak in a highly vaccinated island population and use of a third dose of measles-mumps-rubella vaccine for outbreak control--Guam 2009 to 2010. The Pediatric infectious disease journal. 2013 Apr:32(4):374-80. doi: 10.1097/INF.0b013e318279f593. Epub [PubMed PMID: 23099425]
Cardemil CV, Dahl RM, James L, Wannemuehler K, Gary HE, Shah M, Marin M, Riley J, Feikin DR, Patel M, Quinlisk P. Effectiveness of a Third Dose of MMR Vaccine for Mumps Outbreak Control. The New England journal of medicine. 2017 Sep 7:377(10):947-956. doi: 10.1056/NEJMoa1703309. Epub [PubMed PMID: 28877026]
Abedi GR, Mutuc JD, Lawler J, Leroy ZC, Hudson JM, Blog DS, Schulte CR, Rausch-Phung E, Ogbuanu IU, Gallagher K, Kutty PK. Adverse events following a third dose of measles, mumps, and rubella vaccine in a mumps outbreak. Vaccine. 2012 Nov 19:30(49):7052-8. doi: 10.1016/j.vaccine.2012.09.053. Epub 2012 Oct 3 [PubMed PMID: 23041123]
Seither R, Yusuf OB, Dramann D, Calhoun K, Mugerwa-Kasujja A, Knighton CL. Coverage with Selected Vaccines and Exemption from School Vaccine Requirements Among Children in Kindergarten - United States, 2022-23 School Year. MMWR. Morbidity and mortality weekly report. 2023 Nov 10:72(45):1217-1224. doi: 10.15585/mmwr.mm7245a2. Epub 2023 Nov 10 [PubMed PMID: 37943705]
Barbel P, Peterson K, Heavey E. Mumps makes a comeback: What nurses need to know. Nursing. 2017 Jan:47(1):15-17. doi: 10.1097/01.NURSE.0000510761.53098.22. Epub [PubMed PMID: 28027128]