Introduction
The role of the nasal cavity is to humidify and warm the inspired air. Also, as the air passes through, the nasal cavity removes minute airborne particles and other debris before the air reaches the lower airways. Columnar epithelium lines the nasal cavity. This type of epithelial lining also secretes mucus that coats the lining and helps with the mucociliary clearance of minute aerosolized particles that become trapped in the nasal mucosa. The nasal cavity also functions to facilitate drainage for the secretions from the adjacent paranasal sinuses. It also captures the odor bearing particles and transmits them to the olfactory recesses, that are in the superior portion of the nasal cavity, just medial to the superior turbinates. Air containing mucosal lined sinuses surround the nasal cavity, which includes the frontal, paired maxillary, sphenoid, and ethmoid sinuses. These cavities directly communicate with the nasal cavity. The secretions from these sinuses drain into the nasal cavity via the thin-walled ostia. Like the nasal cavity, the wall lining of the sinuses also secretes mucus. The cilia on the surface sweep the mucus in a carpet like fashion and move them towards the nasal ostia. The hard palate lines the floor of the nasal cavity. The lateral walls are spiral shaped mucosal folds that overlie the turbinates and sinus ducts draining into the ostia. The spiral shape of the turbinates is designed to increase the surface area for the inspired air.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The nasal cavity is the most cephalic part of the respiratory tract. It communicates with the external environment via the anterior apertures, nares, and the nasopharynx via the posterior apertures, choanae. This cavity is divided into two separate cavities by the septum and kept patent by a bone and cartilaginous framework. Each cavity consists of a roof, floor, medial wall, and lateral wall. Within each cavity are three regions; nasal vestibule, respiratory region, and olfactory region.
Surrounding the nasal cavities are air-containing mucosal lined sinuses, which include the frontal sinuses (superior anterior), ethmoid sinuses (superior), paired maxillary sinuses (lateral), and sphenoid sinuses (posterior). All of these paranasal sinuses, except the sphenoid, communicate with the nasal cavity via ducts that drain through ostia, which empty into spaces located on the lateral wall. The sphenoid sinus empties into the posterior roof. Having a fundamental knowledge of the anatomy of the nasal cavity is vital in understanding its functions.
Respiratory Region
The respiratory region functions to humidify, warm, filter, protect, and eliminate debris. Covered in respiratory epithelium and mucous cells, this is the most substantial part of the nasal cavity. As air traverses through the nasal cavity, it warms to body temperature and reaches near one hundred percent humidity. The neurovascular supply of this region aids this. It regulates the nasal airflow by controlling the blood volume in the erectile tissue on the inferior turbinate and anterior septum. Under normal conditions, this tissue is continuously stimulated by sympathetic signals via the superior cervical ganglia to keep the nasal cavity uncongested.
Particles that get past the nasal vestibule then become trapped in the mucosa of the nasal cavity. When this occurs, the mucociliary system helps get rid of these particles. The ciliated pseudostratified columnar epithelium sweeps particles at a rate of one centimeter per minute into the nasopharynx for further expulsion.
The mucus of the nasal cavity forms a protective barrier to inhaled pathogens. The components of the mucus that actively protect the host are immunoglobulin A, lysozymes, and lactoferrin.[1][2][3]
Olfactory Region
Olfaction requires orthonasal or retronasal airflow to transport odor-bearing particles up to the olfactory epithelium located at the apex of the nasal cavity. As odorants become trapped in the mucus, it binds to odorant binding proteins that concentrate and help solubilize the particles. The particles are then attached to olfactory receptors on cilia that transmit specific signals up through the cribriform plate to synapse with neurons of the olfactory bulb, which then sends signals through the olfactory nerve (CNI) into the secondary neurons for higher processing before entering the brain. A unique feature of the olfactory receptors is that a single receptor cell can detect only one odorant type and cannot regenerate.[1][2][3]
Nasal Vestibule
The nasal vestibule is the first area encountered as you move posteriorly through the anterior nares, also known as the nostrils or external nasal valve. The first half of the vestibule has a covering of keratinized stratified squamous epithelium that contains coarse hairs called vibrissae. These hairs filter inhaled particles. The covering of the second half of the vestibule is in respiratory epithelium, pseudostratified ciliated columnar epithelium.[1][2][3]
- Lateral: lateral crus of the lower lateral cartilage (LLC) and fibrofatty alar tissue
- Medial: medial crus of the LLC and septal cartilage
- Posterior: limen naris
The roof of the Nasal Cavity
The mucosa of the roof of the nasal cavity contains perforations that communicate with the cribriform plate. Within these perforations are the olfactory axons.[1]
- Anterior: nasal spine of the frontal bone and nasal bone
- Posterior: cribriform plate of the ethmoid and the body of the sphenoid
The floor of the Nasal Cavity
The floor of the nasal cavity is broader than that of the roof.[1]
- Anterior: the palatine process of the maxilla
- Posterior: horizontal plate of the palatine bone
Incisive Canal
This canal is located in the floor of the nasal cavity, posterior to the central incisor, and lateral to the nasal septum. This structure transmits the nasopalatine nerve into the oral cavity and the greater palatine artery into the nasal cavity.[1]
Nasal Septum
The nasal septum partitions the nasal cavity into two equal but separate compartments. Cartilage and bone comprise the nasal septum. It is covered by squamous epithelium, which differs from the lateral walls of the nasal cavity. A portion of the anterior septum is covered in erectile tissue. It also contributes to lateral projections called the upper lateral cartilages, which makes up the middle third of the nose. The bony segment of the septum is pneumatized, and when it over expands, it has the potential to obstruct airflow. Below are the components of the septum.[1]
Quadrangular (septal) cartilage: This is the most anterior portion of the septum. It contains the Kiesselbach plexus (see blood supply).[4]
Attachments:
- Superior: nasal bone
- Inferior: anterior nasal spine of the maxilla
- Posterior-Superior: perpendicular plate of the ethmoid
- Posterior-Inferior: vomer and maxillary crest
Perpendicular Plate of the Ethmoid: This is a vertical projection from the cribriform plate of the ethmoid inferiorly to the septal cartilage.[5]
Vomer: Located inferior and slightly posterior to the perpendicular plate of the ethmoid. It is attached inferiorly to the nasal crest of the maxilla and palatine bone.[5]
Nasal Crest of the Maxilla and Palatine Bone: Together these bones form the inferior support for the septal cartilage.[5]
Anterior Nasal Spine of the Maxilla: This is a bony projection formed by the paired maxillary bones. It located anterior to the piriform aperture and are palpable at the superior portion of the philtrum of the upper lip.[5]
Lateral Wall of the Nasal Cavity
The nasal cavity's lateral wall has three medially projecting inferiorly curved bones called conchae. The middle and superior conchae are part of the ethmoid bone, whereas the inferior concha is a separate bone altogether. There is a normal variant called the supreme conchae. These conchae, when covered by mucosa, are termed turbinates. The turbinates augment the surface area of the nasal cavity to aid in its functions of humidifying, warming, and humidifying the air. The turbinates create four channels. Three of these channels are termed meatuses, and the fourth is the sphenoethmoidal recess.[1][6][5][7]
Bones of the lateral wall:
- Ethmoid bone
- Perpendicular plate of the palatine bone
- The medial plate of the pterygoid process of the sphenoid bone
- Medial surface of the lacrimal and maxillary bones
- Inferior concha
Sphenoethmoidal Recess: Located superior to the superior turbinate and inferior to the nasal cavity roof, which is the drainage site of the sphenoid sinus.[1][6][5][7]
Meatuses
- Superior Meatus: located inferior to the superior turbinate and superior to the middle turbinate; this is the drainage site of the posterior ethmoid sinus.
- Middle Meatus: located inferior to the middle turbinate and superior to the inferior turbinate - there are several structures within this meatus. This is the drainage site of the frontal, anterior ethmoid, and maxillary sinuses.
- Inferior Meatus: Located inferior to the inferior turbinate and superior to the floor of the nasal cavity. The nasolacrimal duct drains tears from the lacrimal sac at the medial aspect of the eye into the anterior portion of this meatus via Hasner's valve.[1][6][5][7]
Limen Naris: The limen naris is a mucosal ridge that signifies the posterior boundary of the nasal vestibule and the anterior boundary of the nasal cavity proper.[1][6][5][7]
Agger Nasi Cells: These cells are the most anterior portion of the anterior ethmoid air cells. They are located anterior and superior to the basal lamella, most anterior attachment to the lateral wall, of the middle turbinate to create the anterior aspect of the frontal recess.[1][6][5][7]
Frontal Recess: Located between the posterior wall of the agger nasi cells and the middle turbinate.[1][6][5][7]
Uncinate Process of the Ethmoid: This is a thin crescent-shaped bone that is part of the ethmoid bone. It is attached to the lacrimal bone anteriorly, the inferior turbinate inferiorly and superiorly to the lamina papyracea. This structure protects the sinuses of the infundibulum from inhaled foreign particles.[1][6][5][7]
Lamina Papyracea: This thin bone is the separation between the orbit and the ethmoid air cells.[1][6][5][7]
Ethmoid Infundibulum: This is a pyramidal shaped channel located at the anterior portion of the semilunar hiatus that drains the maxillary, anterior ethmoid, and frontal sinuses.[1][6][5][7]
Semilunar Hiatus: Located between the uncinate process anteriorly and the ethmoid bulla posteriorly, this is a space that empties the ethmoid infundibulum.[1][6][5][7]
Ethmoid Bulla: Located just anterior to the semilunar hiatus and superior to the ethmoid infundibulum, which is where the middle ethmoidal air cells open into the nasal cavity.[1][6][5][7]
Ostiomeatal Complex (OMC): This is an area located lateral to the middle turbinate that houses the ostia of the lateral wall sinuses; frontal, maxillary, and anterior/middle ethmoid sinuses.[1][6][5][7]
Sphenopalatine Foramen: This foramen connects the nasal cavity to the pterygopalatine fossa and is posterior to the middle turbinate in the posterior portion of the superior meatus. The significant content of this foramen is[1][6][5][7]:
- Sphenopalatine artery of the maxillary artery
- Nasopalatine branch of the maxillary nerve of the trigeminal nerve (CNV2)
- Posterior superior lateral nasal nerves of CNV2
Choanae
The choanae are also known as posterior nasal apertures. It is the posterior boundary of the nasal cavity proper. It opens into the nasopharynx.[1][6][5][7]
- Superior: the body of the sphenoid bone
- Inferior: horizontal plate of the palatine bone
- Lateral: the medial pterygoid process of the sphenoid bone
- Medial: vomer
Internal Nasal Valve (INV)
The INV is the narrowest portion of the nasal cavity and constitutes the area of highest resistance to airflow, which causes an increase in the acceleration of airflow. Without proper support, this increased airflow causes a decrease in intraluminal pressure, which ultimately causes the INV to collapse; this is Bernoulli's principle of flow. The average cross-sectional area of the INV in adults is around 0.73 square centimeters. At the apex of the valve the ULC and, the nasal septum come together at an angle of 10 to 15 degrees.[8]
- Superior: upper lateral cartilage (ULC/caudal edge)
- Inferior: nasal floor or hard palate
- Lateral: the anterior portion of the inferior turbinate
- Medial: nasal septum
Embryology
The nasal placodes, oval thickenings of surface ectoderm, develop inferior and lateral to the frontonasal prominence at the end of the fourth week of the embryonic period. They contain mesenchyme near the outer edges that begin to proliferate to form the medial and lateral nasal prominences (MNP, LNP). As a result, the nasal placodes reside in deep nasal pits, which are the primitive anterior nares and nasal cavities. The LNP form the alae of the nose. The MNP forms the nasal septum, ethmoid bone, and cribriform plate.[9][10]
As the maxillary prominences proliferate the cause the nasal structures to move medially and by the end of the sixth week, the maxillary prominences begin to merge with the LNP at the nasolacrimal groove. During the sixth to eighth weeks, the nasal cavity and the oral cavity begin to communicate through the choanae. As this is occurring, the lateral wall of the nasal cavity begins forming five ethmoturbinals. The ethmoturbinals eventually form the turbinates and other structures found within each meatus of the nasal cavity.[9][10][11]
- One: agger nasi cells and uncinate process
- Two: ethmoid bulla
- Three: basal lamella of the middle turbinate
- Four: superior turbinate
- Five: supreme turbinate (a normal variant that undergoes
The olfactory epithelium is developing from the ectoderm in the roof of the nasal cavity while the conchae are forming.
Blood Supply and Lymphatics
Arterial Supply
The nasal cavity has an abundant supply of vasculature to aid in functions of warming and humidifying inhaled air. It allows the mucosa to enlarge and shrink, under the influence of sympathetic innervation. The arterial supply to the nose and nasal cavity originates from the internal and external carotid arteries.[12]
Internal Carotid Artery (ICA)
The primary branch off of the ICA that supplies the nasal cavity is the ophthalmic artery. Coming off of the ophthalmic artery are the anterior and posterior ethmoid arteries, as well as the dorsal nasal artery. The anterior ethmoid artery supplies the lateral nasal wall and the nasal septum. The posterior ethmoid artery supplies the superior turbinate and the nasal septum. The dorsal nasal artery supplies the dorsal aspect of the external nose.[1][2]
External Carotid Artery (ECA)
The ECA gives rise to the maxillary artery and the facial artery. These two significant arteries then branch into smaller vessels.
Maxillary Artery
The maxillary branches into the descending palatine artery that then travels through the pterygopalatine fossa down the palatine canal and then branches into the greater and lesser palatine arteries. The greater palatine artery then enters the greater palatine foramen on the posterior aspect of the palate before traversing the palate anteriorly to enter the nasal cavity via the incisive canal. It supplies the septum and the floor of the nasal cavity.
Like the descending palatine artery, the sphenopalatine artery is a branch of the maxillary artery. It branches off of the maxillary artery near the pterygopalatine fossa where it then enters the lateral wall of the nasal cavity through the sphenopalatine foramen, located just posterior to the medial turbinate. The sphenopalatine artery then branches into the posterior lateral nasal branches and the posterior septal branch. The posterior lateral branches supply the middle and inferior turbinates, while the posterior septal branch supplies the posterior septum.[1][2][13]
Facial Artery
The facial artery gives rise to the superior labial artery, the lateral nasal artery, and the angular artery. The superior labial artery gives off an alar branch and a septal branch that supply the same structures as their name. The lateral nasal artery supplies the alar cartilage on the external nose and also supplies the nasal vestibule. The angular artery supplies the external nasal tip, dorsum, and lateral wall.[1][2][13]
Kiesselbach's Plexus (Little's Area)
Kiesselbach's plexus is a vascular anastomosis between the anterior ethmoid artery, superior labial artery, greater palatine artery, and the terminal branch of the posterior septal branch of the sphenopalatine artery. This vascular plexus is located in the anterior nasal septum and is the most common site of epistaxis.[14]
Woodruff's Plexus
Woodruff's plexus is a vascular anastomosis between the sphenopalatine artery and the ascending pharyngeal artery. Located on the lateral wall of the nasal cavity in the area posterior to the middle and inferior turbinates.[15]
Venous Drainage
The names of the veins that drain the nose and nasal cavity follow that of the arteries with which they pair. The maxillary branches drain either into the cavernous sinus or the pterygoid plexus located in the infratemporal fossa. The veins of the anterior nasal cavity drain into the facial vein. Of note, infections located between the oral commissure and nasal bridge, have the potential to become intracranial infections. These must be treated promptly to prevent the extension of infection.
Lymphatics
The anterior nasal cavity drains anteriorly to the face that then makes its way to the submandibular lymph nodes in level IB. The lymphatics of the posterior nasal cavity and paranasal sinuses drain into the upper cervical lymph nodes and retropharyngeal lymph nodes.[16][17]
Nerves
Olfactory Nerve (CNI)
The olfactory nerve transmits signals from the nasal cavity to the brain to give the sense of olfaction. The olfactory epithelium is in the superior portion of the nasal cavity. Within this epithelium are sensory cilia that project up through the cribriform plate to the olfactory bulb. From the olfactory bulb, signals are sent through the olfactory nerve proper to a network of secondary neurons for processing before ending up in the brain.[18]
Trigeminal Nerve (CNV)
The trigeminal nerve is the sensory innervation to the external and internal nose. The branches are the ophthalmic (V1), maxillary (V2), and mandibular (V3). Sympathetic and parasympathetic fibers run with these branches to supply their target tissues. The ophthalmic and maxillary branches innervate the nose and nasal cavity.[19][20]
- Ophthalmic Branches (V1): As the ophthalmic nerve begins to branch, it gives off a nasociliary branch, which then provides the anterior and posterior ethmoid nerves. The anterior ethmoid gives off an external branch that supplies the nasal tip, an internal branch that supplies the anterosuperior nasal cavity and a septal branch that supplies the anterior superior nasal septum. The posterior ethmoid supplies the posterosuperior nasal cavity. Two other branches of the ophthalmic branch of the trigeminal nerve are the supratrochlear and infratrochlear nerves that supply the nasal dorsum.[19][20]
- Maxillary Branches (V2): The maxillary branches of the trigeminal nerve that innervate the nose and nasal cavity branch in or near the pterygopalatine fossa then enter the nasal cavity. The only external nasal branch is the infraorbital nerve, which supplies the malar and lateral nose. The nasopalatine nerve traverses the nasal septum from posterior to anterior in a downward projection to enter the incisive canal. It supplies the posterior and inferior nasal septum as well as mucosa just posterior to the incisors. The greater palatine nerve follows the greater palatine artery down the palatine canal, giving off posterior inferior lateral nasal nerves that supply the posterior lateral wall of the nasal cavity. Three other nerves come off the maxillary branch (V2). Two of these are the posterior superior lateral nasal nerve and posterior superior medial nasal nerve, both of which pass through the sphenopalatine foramen to supply the lateral and medial walls of the nasal cavity, respectively. The superior alveolar nerve is the last branch of V2, and it supplies the anterior septum and the area near the nasal vestibule.[19][20]
Muscles
The muscles of the face subdivide into four groups. These groups consist of the orbital group, the nasal group, the oral group, and others. The muscles correlating with the nasal group are the nasalis, procerus, and depressor septi. Another muscle, levator labii superioris alaeque nasi, is associated with the oral group but has functions associated with the nose. The facial nerve, CNVII, is the innervation for these muscles.
Nasalis
- Transverse part: Originates on the maxilla lateral to the nose and inserts on the dorsum of the nose. This part compresses the nasal aperture.[21]
- Alar part: Originates above the lateral incisor and inserts on the alar cartilage. The function of this part is to open the nostril by pulling the alar cartilage down and lateral.[21]
Procerus
The procerus originates on the nasal bone and upper lateral cartilage while inserting on the skin overlying the glabella. The function of the procerus is to wrinkle skin over the bridge of the nose by pulling the medial angle of the eyebrows downward.[21][22]
Depressor Septi
The depressor septi originates on the maxilla above the central incisors and inserts on the anterior septum. This muscle's primary function is to draw the nose inferiorly.[21][22]
Levator Labii Superioris Alaeque Nasi (LLSAN)
The LLSAN originates on the frontal process of the maxilla and inserts on the alar cartilage and upper lip. The function of this muscle is to open the nostril and elevate the upper lip.[21][22]
Physiologic Variants
Despite having the same essential structural components as the rest of the world, the nose is unique among individuals. Genetics and environmental variation have led to evolutionary changes to the anatomy of the nose within our species. The shape of the nostrils, the angle of the nasal tip, and the width of the nasal bridge are examples of visible variations that give each person a distinct nose.[23]
The uncinate process of the ethmoid bone, as previously described, attaches to the lacrimal bone and the inferior turbinate. The third attachment can vary between the lamina papyracea, the roof of the ethmoid, and the middle turbinate.[6]
Middle Turbinate
The middle turbinate, as previously described, has some common variations associated with it. The variants can obstruct the infundibulum, middle meatus, and if severe, the nasal cavity. As with the inferior turbinate, the middle turbinate can also enlarge by a process called aeration. When the middle turbinate is aerated, it is termed concha bullosa. Normally the middle turbinate is curved downward and laterally like the other turbinates. When the middle turbinate is curved upward, and medially it is named a paradoxical middle turbinate.[24][25]
Surgical Considerations
Congenital Disease
Congenital diseases of the nose need to be addressed due to newborns being nasal breathers. Some signs that a nasal disorder is present are cyanosis when feeding that improves with crying, failure to thrive, and tachypnea.
Choanal Atresia
Choanal atresia occurs due to the presence of the bucconasal membrane or neural crest cell migration into the posterior nasal cavity. During development, the bucconasal membrane usually obliterates around the sixth week of gestation. If neural crest cell migration is the origin of the atresia, it can form a bony, bony-membranous, or membranous obstruction, the most common being the mixed bony-membranous.
Choanal atresia can be a unilateral or bilateral obstruction. Unilateral atresia is typically associated with a right-sided defect, and bilateral atresia is associated with CHARGE syndrome. When bilateral atresia is observed, the physician must also inspect for coloboma, heart disease, retarded CNS growth, and genital and ear abnormalities. The 'A' in CHARGE stands for atresia. Inserting a small transnasal catheter and visualizing a non-patent nasal passage via CT, endoscopy, or mirror are used to diagnose choanal atresia. The repair of the defect is typically done electively for unilateral and within the first week of life if bilateral. Transnasal and transantral endoscopic techniques are employed to repair these defects.[26]
Infection
Infections of the nasal cavity are categorized as acute, recurrent-acute, or chronic. The first line treatment for these is medical management. Failure of medical management warrants consideration for surgery. Abscesses of the nasal cavity must undergo incision and drainage to prevent the spread of the infection. Other infections must be controlled immediately with combination therapy of medical and surgical treatments.
Acute Invasive Fungal Sinusitis
Acute invasive fungal sinusitis is an infection predominantly seen in immunocompromised states like HIV, diabetic ketoacidosis, and transplantation. The pathogens responsible for this infection are Aspergillus, Mucor, Rhizopus, and Absidia. These pathogens invade bone and soft tissue.
Mucormycosis is distinct from the others in that it can invade the surrounding vasculature leading to tissue necrosis. The necrotic tissue may present as black areas on the turbinates and palate. If not treated urgently, the patient can progress into an obtunded state and eventually, death.
The treatment for acute invasive fungal sinusitis involves surgical debridement and antifungal medications.[27]
Trauma
In the setting of trauma, spontaneous or iatrogenic, surgery must be considered. CSF leaking into the nasal cavity is an indication that the roof of the nasal cavity is compromised and the cranial vault is now exposed. This can occur with a direct blow to the face or during a sinus surgery where the surgeon removes too much tissue and violates the nasal cavity boundary. Trauma can also cause profuse bleeding from the nasal cavity. When the bleeding cannot be controlled with non-invasive techniques, vascular ligation and embolization can be used. A child presenting with purulent discharge from the nose could have a foreign body in the nasal cavity. When visualization of the object is not obtained at the bedside, endoscopic surgery is utilized for retrieval.[28][29]
Juvenile Nasopharyngeal Angiofibroma (JNA)
JNA is the most common vascular mass found in the nasal cavity. It is typically seen in adolescent males with recurrent epistaxis and even nasal obstruction. The site it is encountered most often is the roof of the nasal cavity near the sphenopalatine foramen. This tumor is locally aggressive but it does not metastasize. To diagnose, imaging is the preferred method; a biopsy is contraindicated due to the risk of hemorrhage. To treat JNA, the surgeon can choose between endoscopic surgery, open surgical approach, chemotherapy, and radiation, or hormonal therapy. The Fisch Classification of invasion aids in determining which treatment modality to use.[30][31]
Fisch's Classification of Invasion:
- Only in the nasal cavity
- Pterygomaxillary fossa or sinuses
- Infratemporal fossa, orbit, or parasellar region
- Cavernous sinus, optic chiasm area, or pituitary fossa
Other indications for nasal surgery include cancers, nasal valve collapse, and cosmetics.
Clinical Significance
The nasal cavity functions to humidify, warm, filter, and act as a conduit for inspired air, as well as protect the respiratory tract through the use of the mucociliary system. The nasal cavity also houses the receptors responsible for olfaction. If any of the functions of the nasal cavity are compromised, the result is likely to manifest in signs and symptoms of clinically significant disease processes. Understanding the anatomy, physiology, and function of a properly functioning nasal cavity is essential in diagnosing and treating the underlying pathology.
Media
(Click Image to Enlarge)
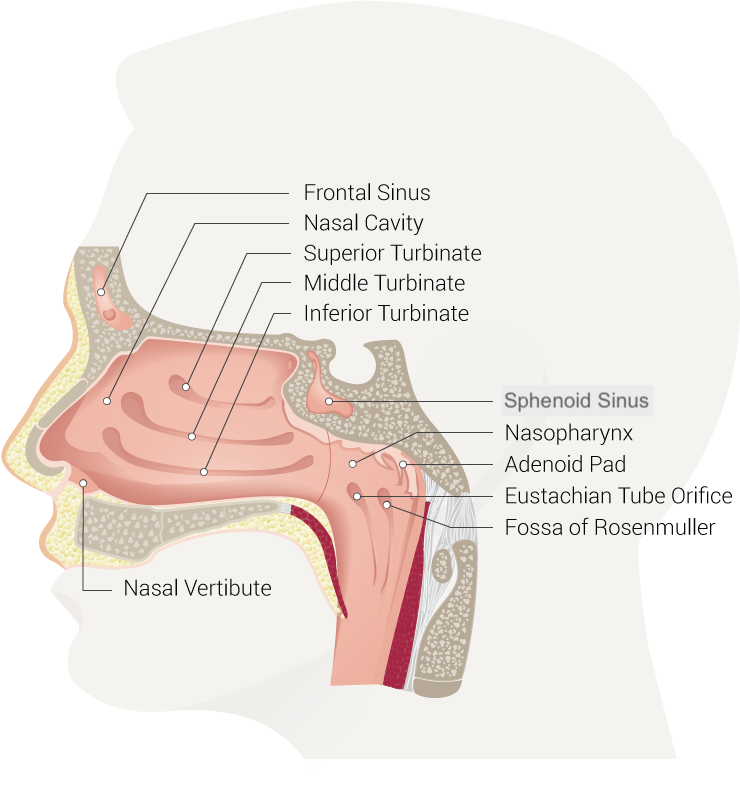
Nasal Cavity. Anatomy of the nasal cavity, including the frontal sinus, superior turbinate, middle turbinate, inferior turbinate, sphenoid sinus, nasopharynx, adenoid pad, eustachian tube orifice, fossa of Rosenmuller, and nasal vestibule.
Contributed by B Palmer
References
Oneal RM, Beil Jr RJ, Schlesinger J. Surgical anatomy of the nose. Otolaryngologic clinics of North America. 1999 Feb:32(1):145-81 [PubMed PMID: 10196443]
Patel RG. Nasal Anatomy and Function. Facial plastic surgery : FPS. 2017 Feb:33(1):3-8. doi: 10.1055/s-0036-1597950. Epub 2017 Feb 22 [PubMed PMID: 28226365]
Lafci Fahrioglu S, VanKampen N, Andaloro C. Anatomy, Head and Neck, Sinus Function and Development. StatPearls. 2023 Jan:(): [PubMed PMID: 30422521]
CONVERSE JM. The cartilaginous structures of the nose. The Annals of otology, rhinology, and laryngology. 1955 Mar:64(1):220-9 [PubMed PMID: 14362333]
AlJulaih GH, Sharma P, Lasrado S. Anatomy, Head and Neck, Nose Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 31082161]
Cappello ZJ, Minutello K, Dublin AB. Anatomy, Head and Neck, Nose Paranasal Sinuses. StatPearls. 2023 Jan:(): [PubMed PMID: 29763001]
Galarza-Paez L, Marston G, Downs BW. Anatomy, Head and Neck, Nose. StatPearls. 2023 Jan:(): [PubMed PMID: 30422465]
Haight JS, Cole P. The site and function of the nasal valve. The Laryngoscope. 1983 Jan:93(1):49-55 [PubMed PMID: 6823174]
Ferrario VF, Sforza C, Poggio CE, Schmitz JH. Three-dimensional study of growth and development of the nose. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 1997 Jul:34(4):309-17 [PubMed PMID: 9257021]
WARBRICK JG. The early development of the nasal cavity and upper lip in the human embryo. Journal of anatomy. 1960 Jul:94(Pt 3):351-62 [PubMed PMID: 13842854]
Asaumi R, Miwa Y, Kawai T, Sato I. Analysis of the development of human foetal nasal turbinates using CBCT imaging. Surgical and radiologic anatomy : SRA. 2019 Feb:41(2):209-219. doi: 10.1007/s00276-018-2145-7. Epub 2018 Dec 6 [PubMed PMID: 30523384]
Widdicombe J. Microvascular anatomy of the nose. Allergy. 1997:52(40 Suppl):7-11 [PubMed PMID: 9353554]
MacArthur FJ, McGarry GW. The arterial supply of the nasal cavity. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2017 Feb:274(2):809-815. doi: 10.1007/s00405-016-4281-1. Epub 2016 Aug 27 [PubMed PMID: 27568352]
Krulewitz NA, Fix ML. Epistaxis. Emergency medicine clinics of North America. 2019 Feb:37(1):29-39. doi: 10.1016/j.emc.2018.09.005. Epub [PubMed PMID: 30454778]
Chiu TW, Shaw-Dunn J, McGarry GW. Woodruff's plexus. The Journal of laryngology and otology. 2008 Oct:122(10):1074-7. doi: 10.1017/S002221510800176X. Epub 2008 Feb 21 [PubMed PMID: 18289456]
Creighton F, Bergmark R, Emerick K. Drainage Patterns to Nontraditional Nodal Regions and Level IIB in Cutaneous Head and Neck Malignancy. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2016 Dec:155(6):1005-1011 [PubMed PMID: 27554510]
Pan WR, Suami H, Corlett RJ, Ashton MW. Lymphatic drainage of the nasal fossae and nasopharynx: preliminary anatomical and radiological study with clinical implications. Head & neck. 2009 Jan:31(1):52-7. doi: 10.1002/hed.20926. Epub [PubMed PMID: 18972423]
Gomez Galarce M, Yanez-Siller JC, Carrau RL, Montaser A, Lima LR, Servian D, Otto BA, Prevedello DM, Naudy CA. Endonasal anatomy of the olfactory neural network: Surgical implications. The Laryngoscope. 2018 Nov:128(11):2473-2477. doi: 10.1002/lary.27194. Epub 2018 Aug 10 [PubMed PMID: 30098048]
Konstantinidis I, Gartz I, Gerber JC, Reden J, Hummel T. Anatomy of the nasal cavity determines intranasal trigeminal sensitivity. Rhinology. 2010 Mar:48(1):18-22. doi: 10.4193/Rhin09.060. Epub [PubMed PMID: 20502730]
Huff T, Weisbrod LJ, Daly DT. Neuroanatomy, Cranial Nerve 5 (Trigeminal). StatPearls. 2023 Jan:(): [PubMed PMID: 29489263]
Hur MS. Anatomical relationships of the procerus with the nasal ala and the nasal muscles: transverse part of the nasalis and levator labii superioris alaeque nasi. Surgical and radiologic anatomy : SRA. 2017 Aug:39(8):865-869. doi: 10.1007/s00276-017-1817-z. Epub 2017 Jan 28 [PubMed PMID: 28132092]
Kuramoto E, Yoshinaga S, Nakao H, Nemoto S, Ishida Y. Characteristics of facial muscle activity during voluntary facial expressions: Imaging analysis of facial expressions based on myogenic potential data. Neuropsychopharmacology reports. 2019 Sep:39(3):183-193. doi: 10.1002/npr2.12059. Epub 2019 May 28 [PubMed PMID: 31136686]
Zaidi AA, Mattern BC, Claes P, McEvoy B, Hughes C, Shriver MD. Investigating the case of human nose shape and climate adaptation. PLoS genetics. 2017 Mar:13(3):e1006616. doi: 10.1371/journal.pgen.1006616. Epub 2017 Mar 16 [PubMed PMID: 28301464]
Level 3 (low-level) evidenceMarks TN, Maddux SD, Butaric LN, Franciscus RG. Climatic adaptation in human inferior nasal turbinate morphology: Evidence from Arctic and equatorial populations. American journal of physical anthropology. 2019 Jul:169(3):498-512. doi: 10.1002/ajpa.23840. Epub 2019 Apr 16 [PubMed PMID: 30993687]
Măru N, Rusu MC, Săndulescu M. Variant anatomy of nasal turbinates: supreme, superior and middle conchae bullosae, paradoxical superior and inferior turbinates, and middle accessory turbinate. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie. 2015:56(3):1223-6 [PubMed PMID: 26662164]
Lesciotto KM, Heuzé Y, Jabs EW, Bernstein JM, Richtsmeier JT. Choanal Atresia and Craniosynostosis: Development and Disease. Plastic and reconstructive surgery. 2018 Jan:141(1):156-168. doi: 10.1097/PRS.0000000000003928. Epub [PubMed PMID: 29280877]
Dwyhalo KM, Donald C, Mendez A, Hoxworth J. Managing acute invasive fungal sinusitis. JAAPA : official journal of the American Academy of Physician Assistants. 2016 Jan:29(1):48-53. doi: 10.1097/01.JAA.0000473374.55372.8f. Epub [PubMed PMID: 26704655]
Daniel M, Raghavan U. Relation between epistaxis, external nasal deformity, and septal deviation following nasal trauma. Emergency medicine journal : EMJ. 2005 Nov:22(11):778-9 [PubMed PMID: 16244333]
Level 2 (mid-level) evidenceGray ST, Wu AW. Pathophysiology of iatrogenic and traumatic skull base injury. Advances in oto-rhino-laryngology. 2013:74():12-23. doi: 10.1159/000342264. Epub 2012 Dec 18 [PubMed PMID: 23257548]
Level 3 (low-level) evidenceAlshaikh NA, Eleftheriadou A. Juvenile nasopharyngeal angiofibroma staging: An overview. Ear, nose, & throat journal. 2015 Jun:94(6):E12-22 [PubMed PMID: 26053985]
Level 3 (low-level) evidenceBakshi SS, Bhattacharjee S. Juvenile Nasopharyngeal Angiofibroma. Journal of pediatric hematology/oncology. 2016 Aug:38(6):491-2. doi: 10.1097/MPH.0000000000000568. Epub [PubMed PMID: 27164528]