Introduction
Nephrogenic systemic fibrosis (NSF) is a progressive multiorgan fibrosing condition mainly caused by patients' exposure to gadolinium-based contrast agents (GBCAs) used for magnetic resonance imaging (MRI).[1] This condition is primarily characterized by thickening of the skin and subcutaneous tissue in addition to systemic manifestations. The clinical features may involve any fibrous tissue in the body, including the internal organs such as the liver, heart, muscles, and lungs.[2][3][4] NSF is a clinically highly variable condition. Some patients may have only mild effects on the skin, other patients may have limited movement, and rarely, the disease may be lethal.[2]
The condition was first described in 2000; however, several years later, a group of nephrologists explained the pathophysiology and the important role of GBCAs to induce this condition.[1][5][6] It occurs in patients with acute or severe chronic renal failure with an estimated glomerular filtration rate (eGFR) of less than 30 mL/min/1.73 m^2.[7][8] The condition was initially called nephrogenic fibrosing dermopathy due to the cutaneous manifestations.[9] The term gadolinium-induced fibrosis or gadolinium-induced NSF has also been used.[1][10][11]
Patients with severe renal insufficiency are at high risk of developing this condition if GBCAs are used in MRI. The incidence rate was dramatically reduced in the last years due to strict adherence of the health care providers with the regulatory guidelines that advise the radiologists to avoid using high-risk GBCAs in severe renal failure.
The association between gadolinium and nephrogenic systemic fibrosis was first put forward in a case series comprising of 13 patients, where all the patients had developed NSF after exposure to gadolinium.[12] One case report published the appearance of NSF after ten years of gadolinium exposure.[13] Newer contrast agents, such as gadobenate dimeglumine carry a smaller risk; however, there is more room for evidence.[14][15]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Nephrogenic systemic fibrosis is a rare disease associated with the use of GBCAs connected to impaired kidney function. Since 1988 when gadopentetate dimeglumine was approved for clinical practice, GBCAs had been intravenously applied to improve MRI examinations' visibility. Gadolinium (Gd) is a known heavy metal, and it is considered highly toxic in biological systems. To be used as a contrast agent, gadolinium must be bound to ligands. GBCAs consist of gadolinium ions and chelating molecules, which could be cyclic or linear. The linear molecules are less stable and provide a weaker link to the gadolinium ion; thus, they are considered high-risk agents.[1][16] The macrocyclic molecules offer better binding to gadolinium ions and provide better protection. The American College of Radiology (ACR) classified the GBCAs into three groups as the following:
- Group 1 (gadopentetate dimeglumine, gadodiamide, gadoversetamide)
- Group 2 (gadobenate dimeglumine, gadoterate meglumine, gadoteridol, gadobutrol)
- Group 3 (gadoxetic acid disodium)
Data suggest that NSF may be because of the use of any GBCA, and the US Food and Drug Administration (FDA) continues to analyze the safety profile of each GBCA to better establish its NSF risks.
The extent of renal insufficiency that leads to the development of NSF is not known. However, some risk factors include stage 4 and 5 chronic kidney disease and inflammatory conditions. The FDA updated the public health advisory in order to include cases with moderate renal failure, such as chronic kidney disease stage 3.[17] The use of metformin may influence NSF, but this needs more evidence.[18]
Epidemiology
Nephrogenic systemic fibrosis is an iatrogenic disease, first identified in 2000. Annually, about 4.5 million Americans are exposed to GBCAs, according to a report by the United States Food and Drug Administration (FDA).[19] Until 2019, the FDA reported 3,094 cases of NSF, including 742 deaths and 2,962 serious cases. The United States has the second-highest MRI utilization rate as opposed to any other country after Germany.[19][20]
NSF has no preference for race, sex, or age.[1][7][4] It is reported in both adults and children.[10] The risk for developing NSF depends on the amount of residual renal function and the type of GBCA used. The amount of initial dose and the cumulative dose of GBCA can also increase the risk.[7] According to a systematic review, very young patients and those older than 80 have a lower risk.[21] However, the validity of this finding has been questioned.[16] A chronic kidney disease patient with a stage 5 is defined as chronic dialysis-dependent or as having an estimated GFR of less than 15 mL/min/1.73 m^2; stage 4 is defined as having an eGFR of less than 30 mL/min/1.73 m^2, and stage 3 as having an eGFR of less than 60 mL/min/1.73 m^2).[1]
When the high-risk group 1 GBCAs were used, the estimated incidence was 36.5 cases per 100,000 gadolinium-enhanced MRI examinations; however, the incidence was reduced to four cases per 100,000 tests after the screening for risk was instituted in 2007.[22] A systematic review showed that only seven biopsy-confirmed cases had been reported with GBCAs exposure after 2008.[21] After the group 2 GBCAs usage commenced, a systematic review found that no patients developed NSF among 4931 patients receiving group 2 GBCAs, for an estimated risk of less than 0.07%.[8] Another systematic review found no patients who developed NSF among 80,932 patient exposures receiving group 2 or 3 (macrocyclic or newer linear) GBCAs.[23]
Deo et al conducted a study on a cohort of end-stage renal failure patients in Connecticut over a period of eighteen months. The incidence of NSF was found to be 4.3 patients per 1000 patient-years. A 2.4% risk of NSF was observed in each radiologic study that used gadolinium.[24]
Todd et al observed an exaggerated risk of developing skin manifestations of NSF with exposure to gadolinium as opposed to patients with no exposure to gadolinium.[25]
Interestingly, delayed-onset NSF was reported in a patient with renal failure in Korea who had a "reverse superscan" observed on bone scintigraphy at the age of 19 years. The patient had exposure to gadolinium at the age of 14 years.[26] A study conducted in Denmark reported an incidence of 12 cases of NSF per one million. This could be the highest noted prevalence worldwide.[27] In France, it was observed that the incidence of NSF markedly reduced after having established new guidelines with regards to the use of gadolinium.[28]
Pathophysiology
The exact pathogenesis is unknown, but most studies hypothesized that gadolinium might dissociate from its chelate and become free Gd.[7] This cation can interact with tissue receptors macrophages or monocytes and stimulate the production of chemokines, profibrotic cytokines, and collagen formation, resulting in fibrosis of the tissues. These cells may stimulate circulating fibrocytes to differentiate into fibroblasts, which preserve a profibrotic phenotype producing elevated amounts of the extracellular matrix.[1][7] This mechanism perpetuates and creates the clinical manifestation of dermal and visceral fibrosis. It is essential to note that patients with severe renal dysfunction (eGFR less than 30 mL/min/1.73 m^2) exposed to GBCAs are more likely to be affected than patients with normal kidney function.[1]
In patients with advanced kidney disease, the injected GBCA remains for more hours than those with normal renal function. Gadolinium is more likely to dissociate from its chelate when the less stable GBCAs are used.[1] Another hypothesis suggests that Gd ion may activate a vicious fibrotic cycle of transforming growth factor-beta 1 (TGF-β1) production and dendritic cell maturation, resulting in excessive collagen deposition in soft tissues.[29] In a mice model, the C-C chemokine receptor 2 has been implicated in the production of NSF.[19][30] Proinflammatory events, hyperphosphatemia, and beta-blockers had been reported as contributing factors.[21]
Various Hypotheses with Regards to Underlying Pathogenic Mechanisms
For historical reasons, it is important to include the following discussion as the understanding of NSF has changed a great deal.
- McNeill and Barr[31] - In 2002, McNeill and Barr proposed that hemodialysis patients with hepatitis C would be more at risk of developing NSF due to high levels of fibroblast growth factor and/or transforming growth factor-beta1.
- Mackay-Wiggan et al[32] - Mackay-Wiggan et al, in 2003, put forward two theories to explain the pathogenesis of NSF. Firstly, they observed that there was a significant role of anticardiolipin or antiphospholipid antibodies in the development of NSF. Secondly, they believed that edema coupled with the suppressed immune system in patients having antiphospholipid antibodies trigger a physiologic response, leading to the proliferation of fibroblast-like cells and deposition of mucin in the dermis.
- Jiménez et al and Ortonne et al - In 2004, the histopathology of NSF was studied and it was found that the fibrotic process of NSF was not limited to the dermis. Instead, it extended to the subcutaneous tissues, fascia, skeletal muscles, lungs, and myocardium. The skin was observed to contain huge numbers of CD68/factor 13a dendritic cells and an abundance of transforming growth factor-beta1.
-
Kucher et al - Nine biopsy specimens of NSF and seven biopsy specimens of scleromyxedema were studied. Immunohistochemical staining was similar for both conditions in terms of CD34, factor 13a, CD31, CD68, smooth muscle actin, and colloidal iron. Procollagen-1 was increasingly expressed in scleromyxedema.[33]
Histopathology
Skin biopsies usually demonstrate dermal fibrosis without signs of inflammation. A significant increase in cellularity is also noted, as shown in the image. These cells are described as being spindle-shaped fibroblasts, fibrohistiocytic, fibroblast-like, or polygonal epithelioid fibroblasts.[34][35] Under light microscopy, the dermal collagen is increased with bundles arranged haphazardly associated with mucin deposition. The abundant spindle-shaped cells often express type 1 procollagen and CD34.[34]
History and Physical
Clinical manifestations of nephrogenic systemic fibrosis (NSF) may occur days or even years after GBCAs exposure but usually present within 2-10 weeks.[7] All patients have a history of renal impairment of varying severity and duration and gadolinium exposure. Many patients have had treatments that include hemodialysis, peritoneal dialysis, or renal transplantation. However, neither dialysis nor transplantation is a prerequisite for nephrogenic systemic fibrosis. Early clinical features include burning pain, pruritus, weakness, and cutaneous papules or plaques, usually accompanied by edema.[1]
Many patients with NSF have calcium-related pathology. Traumatic calcinosis cutis has been observed in dialysis patients with NSF. Osseous metaplasia in the background of NSF has also been noted.[36] A variant of NSF has been referred to as a pathology of dysregulated matrix remodeling and it appears to have osteoclast-like giant cells. Calciphylaxis and metastatic calcification have also been reported in association with NSF.[37]
Patients may have tightening or thickening of the skin. Stiffening of hands and contractures can occur. Patients may also report that their skin looks shinier. This condition may develop slowly. In many patients, some prominent features can be pain or pruritus causing a great deal of distress to them. In some reports, dialysis-related NSF has been observed to involve skeletal muscle.[38]
Further progression of the disease leads to thickened and hyperpigmented skin (as shown in the image). The disease may involve both the lower and upper extremities, progresses from the distal extremity to the proximal one, and always spares the face. The skin is shiny and hard to the touch. A woody consistency is typical. Papules and subcutaneous nodules can also be seen. The skin can have a peau d'orange appearance, and plaques may have an amoeboid advancing edge. Joint involvement usually results in disability and contractures. Yellow scleral plaques have been reported. The fibrosis may also involve the renal tubules, lungs, dura mater, ocular sclera, and skeletal and cardiac muscles.[1] If the lungs are affected, the mortality rate increases, particularly if the diaphragm is involved.[10] The face is almost always spared. Yellow-colored palmar papules that appear as cutaneous calcinosis have been noted. Additionally, some reports suggest the appearance of yellow scleral plaques in patients with NSF.
Evaluation
There is no specific test that accurately diagnoses nephrogenic systemic fibrosis (NSF). The diagnosis is usually made with a good history, appropriate physical examination, and exclusion of other differential diagnoses. The health professional should consider the clinical scenario of this condition while making the diagnosis. The typical clinical scenario is a patient with severe renal insufficiency (eGFR less than 30 mL/min/1.73 m^2) exposed to GBCAs during an MRI examination. It is essential to know that patients with mild or moderate renal insufficiency may also be affected by this condition, but this occurred when older high-risk GBCAs were utilized. The biopsy of the affected organ, including the skin with the typical findings, may furtherly support the diagnosis.[1]
A deep punch biopsy of the skin should be performed. A sample of the dermis, subcutaneous fat, and fascia should ideally be obtained. On histopathology, lesions within 20 weeks of disease onset show reticular, dermal, large, and epithelioid or stellate spindle cells. These cells extend into the subcutaneous fat lobule septa and widen it. The spindle cells are arranged diffusely among thickened collagen bundles. Clefts encompass spindle cells that are CD34/procollagen positive and form a dense interconnecting network. Lesions that are older than 20 weeks from clinical onset have less prominent clefting, less mucin, and fewer CD34/procollagen–positive cells. Calcification, which is dystrophic in nature, can be present. Histopathologically, nephrogenic systemic fibrosis resembles scleromyxedema.
Rarely, some patients with NSF are found to have the following in their blood:
- Peripheral eosinophilia
- Antinuclear antibodies
- Anticardiolipin or antiphospholipid antibodies
- Hypercoagulability
Nerve conduction abnormalities have been reported in some patients.
Treatment / Management
To date, there are no proven treatments that cure nephrogenic systemic fibrosis (NSF). Restoration of renal function, if feasible, is essential to prevent further progression as it appears to slow or hold the progression.[7] Some studies showed limited skin lesions improvement by using intravenous immunoglobulin, photopheresis, and local administration of interferon.[1][7][39] Extracorporeal photopheresis (ECP) appears to provide the best but extremely expensive treatment for nephrogenic systemic fibrosis.(B2)
New research documented that using steroids and methotrexate combined with ultraviolet A (UV-A) phototherapy may relieve cutaneous symptoms. UV-A phototherapy can decrease skin induration by suppressing the production of procollagen and TGF-β1.[29] Methotrexate is thought to reduce systemic immune and inflammatory reactions while suppressing profibrotic factors' activities.[40] In one study low-dose oral imatinib mesylate improved skin texture but not joint mobility.[41] Cyclophosphamide has not shown the efficacious in the treatment of NSF. Topical calcipotriene led to subjective improvement in two patients. Calcipotriene and betamethasone dipropionate together seem to have some role in the topical treatment of NSF.(B2)
Narcotic analgesics may be required to control pain secondary to contractures.[1] Physical therapy is an important part of the treatment to maintain and improve joint motion and reduce contractures.[1] Renal transplantation may improve or produce symptom reduction.[42][43][44] Restoration of renal function had shown symptomatic improvements.[21](A1)
In 2005, photodynamic therapy was reported by Schmook et al as a successful treatment option for NSF.[45] In 2004, UV-A1 was reported as a viable treatment option for NSF by Kafi et al.[46] In 2004, Chung and Chung reported that NSF responded to intravenous immunoglobulin.[47] Wahba et al suggested that UV light treatment is also a management option for NSF, based on two cases they observed.[48] Yerram et al published a case where a patient with NSF who had multiple previous exposures to gadolinium responded substantially to intravenous sodium thiosulfate.[49](B3)
Differential Diagnosis
Nephrogenic systemic fibrosis (NSF) diagnosis relies on excluding the other differential diagnosis; thus, the healthcare providers should be aware of these differentials while making the final diagnosis. The following diseases encompass the most likely differential diagnosis:[1]
- β-microglobulin amyloidosis
- Calciphylaxis
- Chronic graft vs. host disease
- Carcinoid syndrome
- Borreliosis
- Dermatofibrosarcoma protuberans
- Lipodermatosclerosis
- Early cellulitis
- Early panniculitis
- Eosinophilic fasciitis
- Fibroblastic rheumatism
- Drug-induced fibrosis
- Radiation-induced fibrosis
- Scleroderma
- Scleromyxedema
- Phenylketonuria
- Porphyria cutanea tarda
- Superficial fibromatosis
It is essential to note that the history of GBCAs exposure during the MRI examination will favor NSF among the differential diagnosis.[50] Among the differential diagnoses, only β2-microglobulin amyloidosis occurs exclusively in individuals with advanced renal disease; however, it usually affects the shoulders, volar wrists, and tongue.[1]
Prognosis
Nephrogenic systemic fibrosis is considered a debilitating, rapidly progressive disease. This condition causes visceral and cutaneous fibrosis in patients with severe renal insufficiency exposed to GBCAs. Although skin changes associated with NSF may be improved after the restoration of kidney function, especially after recovery from acute kidney injury, this condition does not usually regress spontaneously and almost always progresses relentlessly. Thus, the prognosis depends on the extent of the visceral fibrosis. It is documented that the mortality rate associated with this condition increases as the disease progresses. The high mortality rate does not come from the cutaneous lesions but rather from visceral fibrosis, particularly in the cardiac and respiratory systems.[25]
Todd et al observed that 24-month mortality following examination was 48% in patients with skin changes and 20% in the cases where skin changes were absent.[25] Within a few weeks of disease onset, the majority of patients become wheelchair-bound due to contractures. Many patients have been reported to have died because of falls and other complications due to their mobility problems. In addition, many patients have reported causalgia and maddening pruritus. Finally, patients can also experience flexion contractures if the condition involves a joint.
Complications
Nephrogenic systemic fibrosis (NSF) complicates the already existing kidney disease. The complications of NSF include:
- The most debilitating NSF sequelae are the fibrosis of the visceral organs such as the heart, lungs, renal tubules, and skeletal muscles. Even though visceral fibrosis is often asymptomatic, it may contribute to the development of pulmonary hypertension, cardiomyopathy, and skeletal muscle weakness.
- Patients with NSF may experience blood vessel thrombosis; as the disease progresses, these patients may develop significant hypotension, affecting their ability to tolerate the hemodialysis.[51]
- Flexion contractures may lead to wheelchair dependence within weeks in many patients.
- Falls are common in these patients and fractures can also occur.
Consultations
The diagnosis and management of nephrogenic systemic fibrosis (NSF) need a multidisciplinary team. Following specialties work as a team for NSF management:
- Dermatology
- Nephrology
- Radiology
- Pulmonology
- Histopathology
- Physical therapy and rehabilitation
Deterrence and Patient Education
Since this disease is caused by GBCAs exposure in patients with severe renal impairment, optimization of the medical therapy could slow down the progression to end-stage kidney disease, especially after an acute kidney injury. Patients with this condition should be informed that there are no proven treatments that could cure the nephrogenic systemic fibrosis (NSF), and the current therapies could only relieve some symptoms. However, if the disease progresses and visceral fibrosis develops, medication adherence may improve the patients' quality of life.[29]
For patients with severe kidney disease, health care providers should discuss and guide patients on the potential risks of GBCAs. Providers should discuss the MRI study's risks and benefits over the alternative use of contrast-enhanced computed tomographic (CT) scan, producing a loss of residual renal function and precipitating dialysis initiation.[52][23] The use of group 2 GBCAs in patients with stage 4 or 5 chronic kidney disease and those in dialysis may be safer than the use of contrast-enhanced CT scan as the residual kidney function is better protected, associated with a survival benefit.[53] Those patients who have received group 1 GBCAs in the past should be more careful as effects can be cumulative.[52]
Pearls and Other Issues
- The incidence rate of nephrogenic systemic fibrosis (NSF) is drastically reduced when the regulatory authorities like the FDA, ACR, and the European Society of Urogenital Radiology (ESUR) implemented precautionary guidelines that advise the radiologist to avoid high-risk GBCAs if the patient has severe renal insufficiency.[2]
- The chelate of GBCAs is categorized into two groups; the first is linear and less stable; the other is macrocyclic, which is more stable and provides better protection.
- The lowest possible dose of GBCA to obtain the essential clinical information should be used.[7][52][54]
- A second dose of GBCA should be delayed for several days to a week or avoided if possible.[7][52]
- The diagnostic benefit of GBCAs in the imaging study must be weighed cautiously against the significant risk of developing this debilitating disease.[52][55]
- There is no prophylactic agent that prevents the development of NSF.
- Patients at risk must be recognized before administering a GBCA to prevent the development of NSF.[7]
- In patients who are in chronic hemodialysis, early hemodialysis is recommended following the GBCA MRI examination.[52][21][23]
- High-risk GBCAs (group 1) are contraindicated for patients with acute kidney injury or severe chronic kidney disease.
- The use of GBCAs (group 2 or 3) is not contraindicated for any patient, including those with acute kidney injury or severe chronic kidney disease (eGFR less than 30 mL/min/1.73 m2).[7][21][23][56]
- A systematic review found that no patient with stage 4 or 5 chronic kidney disease developed NSF after receiving a group 2 GBCAs and estimated the risk for developing NSF at less than 0.07%.[8] This result was independent of the patient's chronic kidney disease stage or if the patient was receiving dialysis.[57]
- Performing a clinically indicated MRI using a group 2 GBCA in a patient with acute kidney injury or severe chronic kidney disease despite the potentially harmful effect may outweigh the risk of developing NSF.[54]
Enhancing Healthcare Team Outcomes
The prevalence of nephrogenic systemic fibrosis (NSF) is higher among individuals with acute or chronic severe kidney disease. It is rational to avoid high-risk GBCAs if the eGFR is less than 30 mL/min/1.73 m^2. The management of this disease requires the collaboration of the entire healthcare team. The radiologist should avoid high-risk GBCAs in patients with severely injured kidneys. The primary provider should be aware of this disease if the patients presented with symptoms after exposure to GBCAs. Good history taking, thorough physical examination, and excluding the other differential diagnosis is the cornerstone for making the correct diagnosis. After confirming the diagnosis, nurses, pharmacists, and physical therapists are essential for better health outcomes. Referral to the appropriate specialist should be a consideration if the disease progresses further.[55]
The ACR recommends screening patients by identifying risk factors for compromised renal function (age more than 60 years, hypertension, diabetes mellitus, dialysis, kidney surgery, kidney transplant, kidney cancer, or single kidney). If the patient presents one of the risk factors, obtaining serum creatinine before GBCA administration is warranted. According to the ESUR, patient assessment is based on the type of GBCA used. If a high-risk GBCA is to be used, serum creatinine and clinical assessment before contrast medium administration must be performed. For intermediate and low-risk GBCAs, a questionnaire assessment of the renal function is sufficient.[7]
Media
(Click Image to Enlarge)

Example of skin changes seen in nephrogenic systemic sclerosis. Contributed by Rian Kabir, MD
(Click Image to Enlarge)
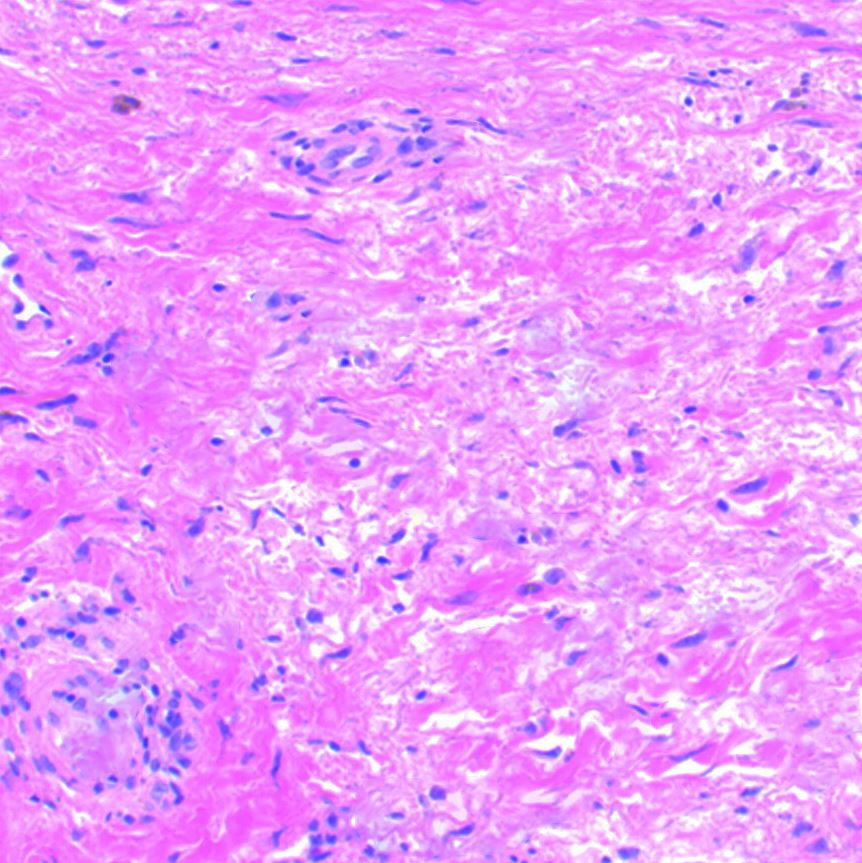
Nephrogenic systemic sclerosis histopathology slide showing dermal fibrosis and an increase in cellularity. Contributed by Rian Kabir, MD
References
Todd DJ, Kay J. Gadolinium-Induced Fibrosis. Annual review of medicine. 2016:67():273-91. doi: 10.1146/annurev-med-063014-124936. Epub [PubMed PMID: 26768242]
Malikova H. Nephrogenic systemic fibrosis: the end of the story? Quantitative imaging in medicine and surgery. 2019 Aug:9(8):1470-1474. doi: 10.21037/qims.2019.07.11. Epub [PubMed PMID: 31559176]
Kitajima K, Maeda T, Watanabe S, Ueno Y, Sugimura K. Recent topics related to nephrogenic systemic fibrosis associated with gadolinium-based contrast agents. International journal of urology : official journal of the Japanese Urological Association. 2012 Sep:19(9):806-11. doi: 10.1111/j.1442-2042.2012.03042.x. Epub 2012 May 9 [PubMed PMID: 22571387]
Mathur M,Jones JR,Weinreb JC, Gadolinium Deposition and Nephrogenic Systemic Fibrosis: A Radiologist's Primer. Radiographics : a review publication of the Radiological Society of North America, Inc. 2020 Jan-Feb; [PubMed PMID: 31809230]
Cowper SE, Su LD, Bhawan J, Robin HS, LeBoit PE. Nephrogenic fibrosing dermopathy. The American Journal of dermatopathology. 2001 Oct:23(5):383-93 [PubMed PMID: 11801769]
Cowper SE, Robin HS, Steinberg SM, Su LD, Gupta S, LeBoit PE. Scleromyxoedema-like cutaneous diseases in renal-dialysis patients. Lancet (London, England). 2000 Sep 16:356(9234):1000-1 [PubMed PMID: 11041404]
Level 3 (low-level) evidenceDaftari Besheli L, Aran S, Shaqdan K, Kay J, Abujudeh H. Current status of nephrogenic systemic fibrosis. Clinical radiology. 2014 Jul:69(7):661-8. doi: 10.1016/j.crad.2014.01.003. Epub 2014 Feb 28 [PubMed PMID: 24582176]
Level 2 (mid-level) evidenceWoolen SA,Shankar PR,Gagnier JJ,MacEachern MP,Singer L,Davenport MS, Risk of Nephrogenic Systemic Fibrosis in Patients With Stage 4 or 5 Chronic Kidney Disease Receiving a Group II Gadolinium-Based Contrast Agent: A Systematic Review and Meta-analysis. JAMA internal medicine. 2020 Feb 1; [PubMed PMID: 31816007]
Level 1 (high-level) evidenceBertero M, Bainotti S, Comino A, Formica M, Giordano F, Musso L, Palazzini S, Seia Z. Nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis. European journal of dermatology : EJD. 2009 Jan-Feb:19(1):73-4. doi: 10.1684/ejd.2008.0547. Epub [PubMed PMID: 19171533]
Level 3 (low-level) evidenceShah AH, Olivero JJ. Gadolinium-Induced Nephrogenic Systemic Fibrosis. Methodist DeBakey cardiovascular journal. 2017 Jul-Sep:13(3):172-173. doi: 10.14797/mdcj-13-3-172. Epub [PubMed PMID: 29744004]
Yee J. Prophylactic Hemodialysis for Protection Against Gadolinium-Induced Nephrogenic Systemic Fibrosis: A Doll's House. Advances in chronic kidney disease. 2017 May:24(3):133-135. doi: 10.1053/j.ackd.2017.03.007. Epub [PubMed PMID: 28501073]
Level 3 (low-level) evidenceMarckmann P,Skov L,Rossen K,Dupont A,Damholt MB,Heaf JG,Thomsen HS, Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. Journal of the American Society of Nephrology : JASN. 2006 Sep; [PubMed PMID: 16885403]
Larson KN, Gagnon AL, Darling MD, Patterson JW, Cropley TG. Nephrogenic Systemic Fibrosis Manifesting a Decade After Exposure to Gadolinium. JAMA dermatology. 2015 Oct:151(10):1117-20. doi: 10.1001/jamadermatol.2015.0976. Epub [PubMed PMID: 26017458]
Bruce R, Wentland AL, Haemel AK, Garrett RW, Sadowski DR, Djamali A, Sadowski EA. Incidence of Nephrogenic Systemic Fibrosis Using Gadobenate Dimeglumine in 1423 Patients With Renal Insufficiency Compared With Gadodiamide. Investigative radiology. 2016 Nov:51(11):701-705 [PubMed PMID: 26885631]
Soyer P, Dohan A, Patkar D, Gottschalk A. Observational study on the safety profile of gadoterate meglumine in 35,499 patients: The SECURE study. Journal of magnetic resonance imaging : JMRI. 2017 Apr:45(4):988-997. doi: 10.1002/jmri.25486. Epub 2016 Oct 11 [PubMed PMID: 27726239]
Level 2 (mid-level) evidenceDavenport MS, Virtual Elimination of Nephrogenic Systemic Fibrosis: A Medical Success Story with a Small Asterisk. Radiology. 2019 Aug; [PubMed PMID: 31268818]
Saab G, Cheng S. Nephrogenic systemic fibrosis: a nephrologist's perspective. Hemodialysis international. International Symposium on Home Hemodialysis. 2007 Oct:11 Suppl 3():S2-6 [PubMed PMID: 17897106]
Level 3 (low-level) evidenceReimer P, Vosshenrich R. [Contrast agents in radiology: current agents approved, recommendations, and safety aspects]. Der Radiologe. 2013 Feb:53(2):153-64. doi: 10.1007/s00117-012-2429-6. Epub [PubMed PMID: 23340684]
Do C, Drel V, Tan C, Lee D, Wagner B. Nephrogenic Systemic Fibrosis Is Mediated by Myeloid C-C Chemokine Receptor 2. The Journal of investigative dermatology. 2019 Oct:139(10):2134-2143.e2. doi: 10.1016/j.jid.2019.03.1145. Epub 2019 Apr 9 [PubMed PMID: 30978353]
Papanicolas I,Woskie LR,Jha AK, Health Care Spending in the United States and Other High-Income Countries. JAMA. 2018 Mar 13; [PubMed PMID: 29536101]
Attari H, Cao Y, Elmholdt TR, Zhao Y, Prince MR. A Systematic Review of 639 Patients with Biopsy-confirmed Nephrogenic Systemic Fibrosis. Radiology. 2019 Aug:292(2):376-386. doi: 10.1148/radiol.2019182916. Epub 2019 Jul 2 [PubMed PMID: 31264946]
Level 1 (high-level) evidencePerez-Rodriguez J, Lai S, Ehst BD, Fine DM, Bluemke DA. Nephrogenic systemic fibrosis: incidence, associations, and effect of risk factor assessment--report of 33 cases. Radiology. 2009 Feb:250(2):371-7. doi: 10.1148/radiol.2502080498. Epub [PubMed PMID: 19188312]
Level 3 (low-level) evidenceGoldstein KM, Lunyera J, Mohottige D, Amrhein TJ, Alexopoulos AS, Campbell H, Cameron CB, Sagalla N, Crowley MJ, Dietch JR, Gordon AM, Kosinski AS, Cantrell S, Williams Jr JW, Gierisch JM. Risk of Nephrogenic Systemic Fibrosis after Exposure to Newer Gadolinium Agents. 2019 Oct:(): [PubMed PMID: 32687278]
Deo A,Fogel M,Cowper SE, Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure. Clinical journal of the American Society of Nephrology : CJASN. 2007 Mar [PubMed PMID: 17699423]
Todd DJ, Kagan A, Chibnik LB, Kay J. Cutaneous changes of nephrogenic systemic fibrosis: predictor of early mortality and association with gadolinium exposure. Arthritis and rheumatism. 2007 Oct:56(10):3433-41 [PubMed PMID: 17907148]
Khor LK, Tan KB, Loi HY, Lu SJ. Nephrogenic systemic fibrosis in a patient with renal failure demonstrating a "reverse superscan" on bone scintigraphy. Clinical nuclear medicine. 2013 Mar:38(3):203-4. doi: 10.1097/RLU.0b013e31827a22ae. Epub [PubMed PMID: 23354034]
Level 3 (low-level) evidenceElmholdt TR, Olesen AB, Jørgensen B, Kvist S, Skov L, Thomsen HS, Marckmann P, Pedersen M. Nephrogenic systemic fibrosis in Denmark--a nationwide investigation. PloS one. 2013:8(12):e82037. doi: 10.1371/journal.pone.0082037. Epub 2013 Dec 9 [PubMed PMID: 24349178]
Amet S,Launay-Vacher V,Clément O,Frances C,Tricotel A,Stengel B,Gauvrit JY,Grenier N,Reinhardt G,Janus N,Choukroun G,Laville M,Deray G, Incidence of nephrogenic systemic fibrosis in patients undergoing dialysis after contrast-enhanced magnetic resonance imaging with gadolinium-based contrast agents: the Prospective Fibrose Nephrogénique Systémique study. Investigative radiology. 2014 Feb [PubMed PMID: 24169070]
Lim YJ, Bang J, Ko Y, Seo HM, Jung WY, Yi JH, Han SW, Yu MY. Late Onset Nephrogenic Systemic Fibrosis in a Patient with Stage 3 Chronic Kidney Disease: a Case Report. Journal of Korean medical science. 2020 Sep 7:35(35):e293. doi: 10.3346/jkms.2020.35.e293. Epub 2020 Sep 7 [PubMed PMID: 32893521]
Level 3 (low-level) evidenceDrel VR, Tan C, Barnes JL, Gorin Y, Lee DY, Wagner B. Centrality of bone marrow in the severity of gadolinium-based contrast-induced systemic fibrosis. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2016 Sep:30(9):3026-38. doi: 10.1096/fj.201500188R. Epub 2016 May 24 [PubMed PMID: 27221979]
McNeill AM, Barr RJ. Scleromyxedema-like fibromucinosis in a patient undergoing hemodialysis. International journal of dermatology. 2002 Jun:41(6):364-7 [PubMed PMID: 12100695]
Level 3 (low-level) evidenceMackay-Wiggan JM,Cohen DJ,Hardy MA,Knobler EH,Grossman ME, Nephrogenic fibrosing dermopathy (scleromyxedema-like illness of renal disease). Journal of the American Academy of Dermatology. 2003 Jan [PubMed PMID: 12522371]
Level 3 (low-level) evidenceKucher C, Xu X, Pasha T, Elenitsas R. Histopathologic comparison of nephrogenic fibrosing dermopathy and scleromyxedema. Journal of cutaneous pathology. 2005 Aug:32(7):484-90 [PubMed PMID: 16008692]
Level 2 (mid-level) evidenceYoldez H, Ahlem B, Abderrahim E, Faten Z, Soumaya R. [Nephrogenic fibrosing dermatosis: From clinic to microscopy]. Nephrologie & therapeutique. 2018 Feb:14(1):47-49. doi: 10.1016/j.nephro.2017.02.017. Epub 2017 Nov 26 [PubMed PMID: 29239786]
Boyd AS, Zic JA, Abraham JL. Gadolinium deposition in nephrogenic fibrosing dermopathy. Journal of the American Academy of Dermatology. 2007 Jan:56(1):27-30 [PubMed PMID: 17109993]
Level 3 (low-level) evidenceRuiz-Genao DP,Pascual-Lopez MP,Fraga S,Aragüés M,Garcia-Diez A, Osseous metaplasia in the setting of nephrogenic fibrosing dermopathy. Journal of cutaneous pathology. 2005 Feb [PubMed PMID: 15606678]
Level 3 (low-level) evidenceHubbard V, Davenport A, Jarmulowicz M, Rustin M. Scleromyxoedema-like changes in four renal dialysis patients. The British journal of dermatology. 2003 Mar:148(3):563-8 [PubMed PMID: 12653751]
Level 3 (low-level) evidenceLevine JM, Taylor RA, Elman LB, Bird SJ, Lavi E, Stolzenberg ED, McGarvey ML, Asbury AK, Jimenez SA. Involvement of skeletal muscle in dialysis-associated systemic fibrosis (nephrogenic fibrosing dermopathy). Muscle & nerve. 2004 Nov:30(5):569-77 [PubMed PMID: 15389718]
Level 3 (low-level) evidenceZhang R, Rose WN. Photopheresis Provides Significant Long-Lasting Benefit in Nephrogenic Systemic Fibrosis. Case reports in dermatological medicine. 2017:2017():3240287. doi: 10.1155/2017/3240287. Epub 2017 Jun 12 [PubMed PMID: 28695022]
Level 3 (low-level) evidenceKowal-Bielecka O,Fransen J,Avouac J,Becker M,Kulak A,Allanore Y,Distler O,Clements P,Cutolo M,Czirjak L,Damjanov N,Del Galdo F,Denton CP,Distler JHW,Foeldvari I,Figelstone K,Frerix M,Furst DE,Guiducci S,Hunzelmann N,Khanna D,Matucci-Cerinic M,Herrick AL,van den Hoogen F,van Laar JM,Riemekasten G,Silver R,Smith V,Sulli A,Tarner I,Tyndall A,Welling J,Wigley F,Valentini G,Walker UA,Zulian F,Müller-Ladner U, Update of EULAR recommendations for the treatment of systemic sclerosis. Annals of the rheumatic diseases. 2017 Aug; [PubMed PMID: 27941129]
Elmholdt TR, Buus NH, Ramsing M, Olesen AB. Antifibrotic effect after low-dose imatinib mesylate treatment in patients with nephrogenic systemic fibrosis: an open-label non-randomized, uncontrolled clinical trial. Journal of the European Academy of Dermatology and Venereology : JEADV. 2013 Jun:27(6):779-84. doi: 10.1111/j.1468-3083.2011.04398.x. Epub 2011 Dec 20 [PubMed PMID: 22188390]
Level 2 (mid-level) evidencePanesar M, Yacoub R. What is the role of renal transplantation in a patient with nephrogenic systemic fibrosis? Seminars in dialysis. 2011 Jul-Aug:24(4):373-4. doi: 10.1111/j.1525-139X.2011.00913.x. Epub [PubMed PMID: 21851392]
Cuffy MC, Singh M, Formica R, Simmons E, Abu Alfa AK, Carlson K, Girardi M, Cowper SE, Kulkarni S. Renal transplantation for nephrogenic systemic fibrosis: a case report and review of the literature. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2011 Mar:26(3):1099-101. doi: 10.1093/ndt/gfq693. Epub 2010 Nov 15 [PubMed PMID: 21079195]
Level 3 (low-level) evidencePanesar M,Banerjee S,Barone GW, Clinical improvement of nephrogenic systemic fibrosis after kidney transplantation. Clinical transplantation. 2008 Nov-Dec; [PubMed PMID: 18713261]
Schmook T, Budde K, Ulrich C, Neumayer HH, Fritsche L, Stockfleth E. Successful treatment of nephrogenic fibrosing dermopathy in a kidney transplant recipient with photodynamic therapy. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2005 Jan:20(1):220-2 [PubMed PMID: 15632355]
Level 3 (low-level) evidenceKafi R, Fisher GJ, Quan T, Shao Y, Wang R, Voorhees JJ, Kang S. UV-A1 phototherapy improves nephrogenic fibrosing dermopathy. Archives of dermatology. 2004 Nov:140(11):1322-4 [PubMed PMID: 15545539]
Level 3 (low-level) evidenceChung HJ, Chung KY. Nephrogenic fibrosing dermopathy: response to high-dose intravenous immunoglobulin. The British journal of dermatology. 2004 Mar:150(3):596-7 [PubMed PMID: 15030351]
Level 3 (low-level) evidenceWahba IM,White K,Meyer M,Simpson EL, The case for ultraviolet light therapy in nephrogenic fibrosing dermopathy--report of two cases and review of the literature. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2007 Feb; [PubMed PMID: 17124282]
Level 3 (low-level) evidenceYerram P, Saab G, Karuparthi PR, Hayden MR, Khanna R. Nephrogenic systemic fibrosis: a mysterious disease in patients with renal failure--role of gadolinium-based contrast media in causation and the beneficial effect of intravenous sodium thiosulfate. Clinical journal of the American Society of Nephrology : CJASN. 2007 Mar:2(2):258-63 [PubMed PMID: 17699422]
Level 3 (low-level) evidenceWagner B, Drel V, Gorin Y. Pathophysiology of gadolinium-associated systemic fibrosis. American journal of physiology. Renal physiology. 2016 Jul 1:311(1):F1-F11. doi: 10.1152/ajprenal.00166.2016. Epub 2016 May 4 [PubMed PMID: 27147669]
He A, Kwatra SG, Zampella JG, Loss MJ. Nephrogenic systemic fibrosis: fibrotic plaques and contracture following exposure to gadolinium-based contrast media. BMJ case reports. 2016 Apr 12:2016():. doi: 10.1136/bcr-2016-214927. Epub 2016 Apr 12 [PubMed PMID: 27073153]
Level 3 (low-level) evidenceMaripuri S,Johansen KL, Risk of Gadolinium-Based Contrast Agents in Chronic Kidney Disease-Is Zero Good Enough? JAMA internal medicine. 2020 Feb 1; [PubMed PMID: 31816006]
Mehdi A, Taliercio JJ, Nakhoul G. Contrast media in patients with kidney disease: An update. Cleveland Clinic journal of medicine. 2020 Nov 2:87(11):683-694. doi: 10.3949/ccjm.87a.20015. Epub 2020 Nov 2 [PubMed PMID: 33139262]
Weinreb JC, Rodby RA, Yee J, Wang CL, Fine D, McDonald RJ, Perazella MA, Dillman JR, Davenport MS. Use of Intravenous Gadolinium-based Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Radiology. 2021 Jan:298(1):28-35. doi: 10.1148/radiol.2020202903. Epub 2020 Nov 10 [PubMed PMID: 33170103]
Level 3 (low-level) evidenceCheong BY, Muthupillai R. Nephrogenic systemic fibrosis: a concise review for cardiologists. Texas Heart Institute journal. 2010:37(5):508-15 [PubMed PMID: 20978560]
Lunyera J,Mohottige D,Alexopoulos AS,Campbell H,Cameron CB,Sagalla N,Amrhein TJ,Crowley MJ,Dietch JR,Gordon AM,Kosinski AS,Cantrell S,Williams JW Jr,Gierisch JM,Ear B,Goldstein KM, Risk for Nephrogenic Systemic Fibrosis After Exposure to Newer Gadolinium Agents: A Systematic Review. Annals of internal medicine. 2020 Jul 21; [PubMed PMID: 32568573]
Level 1 (high-level) evidenceShankar PR, Davenport MS. Risk of Nephrogenic Systemic Fibrosis in Stage 4 and 5 Chronic Kidney Disease Following Group II Gadolinium-based Contrast Agent Administration: Subanalysis by Chronic Kidney Disease Stage. Radiology. 2020 Nov:297(2):447-448. doi: 10.1148/radiol.2020201492. Epub 2020 Aug 18 [PubMed PMID: 32808890]