Introduction
Nursemaid's elbow, or "radial head subluxation" is a common injury in young children in which the radial head slips under the annular ligament resulting in pain and inability to supinate the forearm. Diagnosis is usually based on clinical exam and history, and reduction can typically be easily performed in the clinical setting.[1][2][3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The annular ligament encircles the radial head and holds it against the ulna. Axial traction on a pronated forearm and extended elbow causes the annular ligament to slip over the head of the radius and become trapped in the radiohumeral joint between the radial head and capitellum.
Epidemiology
Radial head subluxation (RHS) is common in children 1 to 4 years of age and represents more than 20% of upper extremity injuries in children. It occurs less commonly in children older than the age of 5 because the annular ligament strengthens with age. There is a slight female predominance, and the left arm is more commonly affected than the right. Recurrence rate is approximately 20%
Pathophysiology
The injury occurs when a child is swung around by the arms, or lifted by one arm. Even seemingly innocuous acts such as pulling on a child’s arm to keep them from falling can lead to radial head subluxation. The displacement of the annular ligament causes discomfort and pain when the child tries to move the arm.
Less common mechanisms of injury include falling onto the elbow or twisting of the forearm. Radial head subluxation can also occur due to longitudinal traction when a child less than six months of age rolls over in bed onto their arm.
History and Physical
Caregivers may describe that just prior to symptom onset the child's arm was pulled upwards by the wrist or the child was swung around by the arms. Caregivers may not be aware of the incident that caused the injury and may report no known trauma. The onset of symptoms may also occur after a fall on an outstretched arm.
On physical exam, the child will often be nervous and may be supporting the affected arm in a protective manner with the opposite hand. The affected arm is often held in complete or almost complete extension and pronation. The patient may refuse to move the arm and may become upset when it is examined, but generally, will not have pain unless the arm is manipulated. There may be tenderness at the radial head, and the patient will resist forearm pronation, supination, flexion, and extension. Generally speaking, ecchymosis, erythema, edema, or signs of trauma are absent. Circulation, sensation and motor ability will be intact distal to the elbow, though the child may not be cooperative with the exam.
It is not uncommon for the radial head subluxation to spontaneously reduce before being seen by a physician. In this case, the caregivers will report that the patient was refusing to move the arm and seemed very upset by any attempt of the parent to manipulate or touch the arm. It can be very disconcerting to parents, especially when the child’s symptoms seem to miraculously disappear. In this case providing reassurance to the parents about the probable diagnosis after doing a proper physical exam is all that is required.
Evaluation
The examination should include a thorough inspection of the affected arm as well as the ipsilateral clavicle. The entire arm should be palpated to assess for tenderness of the bones and joints. The diagnosis of radial head subluxation can typically be made clinically. Imaging should be performed if there is suspicion for fracture, elbow dislocation, or if edema or deformity are present on exam. Imaging is also indicated if the mechanism did not involve the typical axial traction of the arm or nonaccidental trauma is a concern. Radiographs are typically normal in radial head subluxation, but the displacement of the radiocapitellar line may be seen on plain film x-rays.[5][6][7][8][9]
Treatment / Management
Treatment involves closed reduction, and this can be performed in a few seconds without sedation. Even though it is brief, it can be painful as the annular ligament reduces to its proper position. It should be explained to parents that the child will likely be upset, but that once the elbow is properly reduced, the pain should resolve and the child will likely be back to baseline within a few minutes.
In order to minimize trauma and increase comfort for the patient, the caregiver should hold the child in their arms, and the examiner should sit facing the child.
Hyperpronation and supination/flexion are two common techniques preferred for reduction of a subluxed radial head. The hyperpronation technique has a higher reported first attempt success rate than the supination/flexion technique. Studies have also suggested that the hyperpronation technique may be less painful than the supination/flexion technique. If it is unsuccessful, the supination/flexion technique may be attempted.
To perform the hyperpronation method, moderate pressure should be applied to the radial head while the child's elbow is supported with the same hand. The forearm should be hyperpronated by applying force to the wrist with the opposite hand. A click is usually felt over the radial head which indicates the maneuver was successful.
To perform the supination/flexion method, slight pressure should be applied to the radial head with the physician's thumb while supporting the elbow with the same hand. The other hand should grasp the patient’s distal forearm. The patient's forearm should then be supinated and fully flexed with gentle traction applied. A click may be felt or heard if the maneuver is successful.
A successful reduction should result in immediate cessation of pain. Most children will begin to use their arm within 5-10 minutes, and within 30 minutes 90% of children will be asymptomatic. It may take a few minutes for the children to realize that it is no longer painful to move the arm. If the patient does not regain function of the arm, imaging studies to assess for fracture or orthopedic consult may be warranted. If the patient refuses to use the arm after several minutes and imaging are normal, the arm should be placed in a sling, and the patient should be referred to an orthopedic surgeon.
If reduction was successful, no splinting or sling is necessary, and the prognosis is excellent. Because of possible recurrence, parents should be instructed to avoid activities that cause axial traction to the arm such as lifting, jerking or swinging the child by the hands, wrists or forearms.
Differential Diagnosis
- Elbow fracture
- Fractured wrist
- Green stick fracture
- Hand injury
- Monteggia fracture
- Supracondylar fracture
- Soft tissue damage of hand
Enhancing Healthcare Team Outcomes
The diagnosis and management of nurse maid's elbow requires an interprofessional team that includes a sports physician, primary care provider, emergency department physician, orthopedic surgeon, and a nurse practitioner.
Treatment involves closed reduction, and this can be performed in a few seconds without sedation. Even though it is brief, it can be painful as the annular ligament reduces to its proper position. It should be explained to parents that the child will likely be upset, but that once the elbow is properly reduced, the pain should resolve and the child will likely be back to baseline within a few minutes.
If reduction was successful, no splinting or sling is necessary, and the prognosis is excellent. Because of possible recurrence, parents should be instructed to avoid activities that cause axial traction to the arm such as lifting, jerking or swinging the child by the hands, wrists or forearms.[10]
Media
(Click Image to Enlarge)
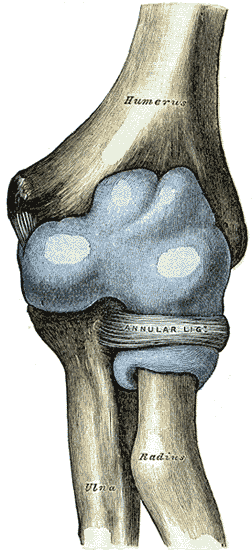
Capsule of elbow-joint (distended). Anterior aspect. (Nursemaid's elbow involves the head of radius slipping out from the anular ligament of radius.)
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mohd Miswan MF, Othman MS, Muhamad Effendi F, Ibrahim MI, Rozali KN. Pulled/nursemaid's elbow. Malaysian family physician : the official journal of the Academy of Family Physicians of Malaysia. 2017:12(1):26-28 [PubMed PMID: 28503271]
Wong K, Troncoso AB, Calello DP, Salo D, Fiesseler F. Radial Head Subluxation: Factors Associated with Its Recurrence and Radiographic Evaluation in a Tertiary Pediatric Emergency Department. The Journal of emergency medicine. 2016 Dec:51(6):621-627. doi: 10.1016/j.jemermed.2016.07.081. Epub 2016 Sep 27 [PubMed PMID: 27687166]
Mak S, Beltran LS, Bencardino J, Orr J, Jazrawi L, Cerezal L, Beltran J. MRI of the annular ligament of the elbow: review of anatomic considerations and pathologic findings in patients with posterolateral elbow instability. AJR. American journal of roentgenology. 2014 Dec:203(6):1272-9. doi: 10.2214/AJR.13.12263. Epub [PubMed PMID: 25415705]
Karasick D. Nursemaid elbow revisited and a review of congenital radioulnar synostosis. Radiographics : a review publication of the Radiological Society of North America, Inc. 2004 Nov-Dec:24(6):1608-10; author reply 1608-10 [PubMed PMID: 15537970]
Level 3 (low-level) evidenceChen H, Shao Y, Li S. Replacement or repair of terrible triad of the elbow: A systematic review and meta-analysis. Medicine. 2019 Feb:98(6):e13054. doi: 10.1097/MD.0000000000013054. Epub [PubMed PMID: 30732120]
Level 1 (high-level) evidenceWang Q, Du MM, Pei XJ, Luo JZ, Li YZ, Liu YC, Wang X, Cao JC, Han JH. External Fixator-assisted Ulnar Osteotomy: A Novel Technique to Treat Missed Monteggia Fracture in Children. Orthopaedic surgery. 2019 Feb:11(1):102-108. doi: 10.1111/os.12426. Epub 2019 Feb 4 [PubMed PMID: 30714691]
Cope B, Tracy M. Not just another nursemaid's: an enigmatic paediatric humeral fracture. BMJ case reports. 2018 Oct 2:2018():. pii: bcr-2017-222925. doi: 10.1136/bcr-2017-222925. Epub 2018 Oct 2 [PubMed PMID: 30279246]
Level 3 (low-level) evidencePawelec B, Waśko MK, Pomianowski S. Neglected Iatrogenic Elbow Joint Dislocation. Didactic Case Report. Ortopedia, traumatologia, rehabilitacja. 2018 Feb 27:20(1):57-63. doi: 10.5604/01.3001.0011.5877. Epub [PubMed PMID: 30152761]
Level 3 (low-level) evidenceGalbiatti JA, Cardoso FL, Ferro JAS, Godoy RCG, Belluci SOB, Palacio EP. Terrible triad of the elbow: evaluation of surgical treatment. Revista brasileira de ortopedia. 2018 Jul-Aug:53(4):460-466. doi: 10.1016/j.rboe.2018.05.012. Epub 2018 Jun 11 [PubMed PMID: 30027079]
Hill CE, Cooke S. Common Paediatric Elbow Injuries. The open orthopaedics journal. 2017:11():1380-1393. doi: 10.2174/1874325001711011380. Epub 2017 Nov 30 [PubMed PMID: 29290878]