Introduction
A healthy optic nerve is a crucial conduit for impulses generated within the layers of the retina to leave the eye. Electrical signals are initiated by the photoreceptors in response to incident light, modified by retinal bipolar cells, and transmitted through the optic nerves to the lateral geniculate bodies. Damage to the nerve fiber layer or optic nerve may compromise the quality of these signals.
The term optic neuritis (ON) is used to describe a variety of conditions affecting the optimal function of the optic nerve. A wide range of conditions including infections, trauma, vascular insufficiency, metastases, toxins, or nutritional deficiencies may cause optic neuropathies but this article focuses on optic neuritis (ON), an inflammatory condition that demyelinates the optic nerve and degrades vision in one or both eyes.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The mechanism responsible for acute optic neuritis (ON) has not been definitively identified but it is believed that an autoimmune reaction damages the myelin sheath that encompasses neurons within the optic nerve. Patients with documented autoimmune diseases [1] have a greater propensity for ON and there is a causal relationship between HLA DRB1,[2] HLA-B27[3] and ON. Some studies suggest that viral illnesses, which are known to precipitate auto-immune reactions, may induce ON attacks. ON may be one manifestation of a demyelinating disease that affects several areas of the central nervous system; ON is often the first clinical manifestation of demyelination.
Epidemiology
The annual incidence of new-onset ON has been reported between 0.56 and 5.1 cases per 100,000 [4].
Risk factors for ON include age (20 to 40 years), sex (female:male = 2:1), and race (Caucasian).
Children infrequently develop bilateral ON but childhood disease is not believed to foreshadow the development of multiple sclerosis [5],[6].
An increased incidence of multiple sclerosis (MS) in temperate climates has been proposed[3],[5].
Studies have identified that the northern United States and western Europe have more cases relative to equatorial regions [6].
Pathophysiology
Optic neuritis (ON) is one manifestation of central nervous system inflammation with resultant demyelination. Recurrent episodes of ON indicate a propensity toward developing more generalized diseases [7] including MS, neuromyelitis optica spectrum disorders (NMOSC), and myelin oligodendrocyte glycoprotein-IgG (MOG)[8]. The extent of axonal damage due to optic neuritis (ON) differs according to the causative condition.
Optic neuritis is the initial inflammatory event in 15-20% of patients with MS [9],[10], and half of MS patients will eventually have had at least one ON attack within the prior 15 years. Multiple sclerosis (MS) occurs more commonly in temperate climates [11],[12] with more cases seen in the northern United States and western Europe as opposed to equatorial regions [13]. Oligoclonal bands within the cerebral spinal fluid are pathognomonic for MS.
Optic neuritis related vision loss in patients with NMOSD and MOG is usually more severe and results in larger scotomas. Since both disorders affect the optic nerve, chiasm, and optic tracts, bilateral vision loss is common. Damage often extends longitudinally into the spinal cord in both conditions.
NMOSD is characterized by frequent ON attacks that cause severe bilateral vision loss with little chance of functional improvement. Spinal cord lesions that extend beyond three vertebral segments are typical of NMOSD and debilitating transverse myelitis often limits physical activities. Detection of AQP4-IgG antibodies confirms the diagnosis of NMOSD.
MOG is also associated with significant bilateral visual impairment but marked ON-related papillitis occurs less frequently than with NMOSD. Marked enhancement of the optic nerve, nerve sheath, and periocular tissues is evident with neural imaging studies. Compared to those with NMOSD, patients with MOG are more likely to experience improved visual function after ON and they may have lower spinal cord involvement. Males and females are affected with equal frequencies [14],[15].
History and Physical
Optic neuritis usually presents with the acute onset of monocular eye pain and vision loss in a young adult. Pain is usually associated with eye movements and often precedes loss of vision. Patients often report having had similar events in the same or fellow eye.
The degree of vision impairment may range from near-normal acuity to no light perception [16]. Nearly any visual field defect may be seen on automated visual field testing but central scotomas are most common. Color perception is significantly impaired (red hues are notably desaturated) and contrast sensitivity is diminished. Patients may experience recurring photopsias. Vision loss may be exacerbated after exercise or elevation of body temperature (Uhthoff phenomenon).
Optic disc swelling is seen on fundoscopy in one-third of patients during the active phase. In the absence of observable papillitis, signs and symptoms of ON are usually sufficient to establish the diagnosis of retrobulbar neuritis.
Bilateral presentation, profound loss of vision, and absence of eye pain prior to vision loss, together with atypical neurologic findings should prompt the search for an alternative etiology. Visual symptoms due to ON tend to resolve over several weeks to months and visual function improves to near-normal levels after six months in the majority of cases. There are, however, instances in which qualitative visual changes persist for the duration of a patient’s life [17], [18].
Evaluation
Clinical evaluation of suspected optic neuritis should include the following:
- Best-corrected visual acuity.
- Automated visual field testing.
- Color vision testing with particular attention to red desaturation.
- Pupillary examination with measurement of a relative afferent pupillary defect (RAPD).
- Note: A RAPD may not be present with bilateral, symmetric optic nerve involvement.
- Optic nerve examination.
- Optical coherence tomography (OCT) evaluation of the retinal nerve fiber layer (RNFL).
If clinical findings are consistent with ON, additional testing should include:
- Magnetic resonance imaging (MRI) of the brain and orbits with and without contrast to look for demyelinating disease.
- In the active phase, the affected optic nerve will enhance.
- Demyelinating lesions within the brain confirm the diagnosis of multiple sclerosis (MS).
- Optic neuritis with two or more typical lesions (one of which is contrast enhancing) is sufficient to diagnose MS (McDonald criteria)
- Clinical findings suggestive of neuromyelitis optica spectrum disorder (NMOSD) should prompt serum NMO-IgG testing.
Treatment / Management
Visual function will return to near-normal levels over weeks to months whether or not treatment any treatment is initiated. However, visual recovery is hastened when treated with corticosteroid therapy.
Based on the long-term results of the Optic Neuritis Treatment Trial (ONTT), the protocol for treating optic neuritis (ON) is widely accepted throughout the medical community.
- Intravenous methylprednisolone (500-1000mg once daily) for three day
- followed by oral prednisone (1mg/kg once daily) for eleven days.
- Note that oral prednisone alone was found to increase the rate of recurrent ON attacks.
If lesions characteristic of multiple sclerosis (MS) are evident with magnetic resonance imaging (MRI), then immune-modulating therapies should be considered to delay subsequent attacks.
Differential Diagnosis
The differential diagnosis of optic neuritis includes the following conditions:
- Inflammatory, demyelinating disease (classic)
- Idiopathic optic neuritis
- Multiple sclerosis
- Neuromyelitis optica
- Myelin oligodendrocyte glycoprotein (MOG) antibody disorder
- Ischemic optic neuropathy
- Autoimmune disorders
- Systemic lupus erythematosus
- Giant cell arteritis
- Sarcoidosis
- Behcet’s disease
- Infectious [19]
- Viral
- Herpes simplex1 and 2
- Varicella-Zoster
- Cytomegalovirus
- Less frequent:
- Human immunodeficiency, Epstein-Barr, Dengue fever, West Nile, Chikungunya
- Measles, Mumps, Rubella, Influenza
- Bacterial
- Bartonella henselae (Cat-scratch disease)
- Treponema pallidum (Syphilis)
- Borrelia burgdorferi (Lyme disease)
- Mycobacterium tuberculosis (Tuberculosis)
- Less frequent:
- Rickettsioses, Coxiella burnetti (Q fever), Tropheryma whippleii (Whipple disease)
- Leptospira, Brucella, Mycobacterium leprae (Leprosy)
- Fungal
- Cryptococcus neoformans (Cryptococcus)
- Candidiasis
- Histoplasma capsulatum (Histoplasmosis)
- Aspergillus fumigatus (Aspergillus)
- Mucormycosis
- Parasitic
- Toxoplasma gondii (Toxoplasmosis)
- Toxocara canis (Toxocariasis)
- Diffuse unilateral subacute necrosis (DUSN)
- Drugs
- Ethambutol/isoniazid
- Chloramphenicol, sulfonamides
- Amiodarone, digitalis
- Quinine, chloroquine, hydroxychloroquine
- Methotrexate, vincristine, tamoxifens
- Nutritional/toxic
- Vitamin B deficiencies, particularly vitamin B12
- Methanol/alcohol
- Tobacco
- Compressive optic nerve lesions
- Most often associated with a slow, subtle onset of signs and symptoms
Pertinent Studies and Ongoing Trials
The standard treatment of acute ON was oral corticosteroids when the collaborative, multicenter Optic Neuritis Treatment Trial (ONTT) [20]sought to clarify the role of corticosteroid therapy. More than 450 patients were enrolled at 15 sites between 1988 and 1991. The average age of enrolled subjects was 32, and most were Caucasian (85%) and female (77%). Subjects were randomized to receive oral prednisone (1 mg/kg daily for two weeks) or intravenous methylprednisolone (250 mg every 6 hours for three days) followed by either oral prednisone for the balance of the two weeks or an oral placebo.
Most subjects in each cohort recovered visual function in the first 1 to 3 months. Visual improvement occurred more rapidly in subjects treated with intravenous methylprednisolone, but there was no difference in the cohorts receiving oral corticosteroids and placebo. Visual acuity did not fully return in many subjects with initial visual acuities of 20/200 or worse. Visual outcomes at six months were similar in all cohorts but optic neuritis recurred twice as often in subjects who received prednisone.
At one year there were no differences in visual function (acuity, visual field, color discrimination, and contrast sensitivity) between subjects who received placebo and corticosteroids (VA of 20/40 or better: placebo (95%), intravenous methylprednisolone (94%), and oral prednisone (91%) [21]. Visual recovery [22],[23],[24],[25], visual field results [26],[27], and neurologic consequences of ON [28],[29],[30],[31],[10],[32]have been reported at three years 7864737[33],[34] and 15 years [35],[36].
Diagnostic and treatment guidelines of ON have evolved over time [37],[38],[39],[40]to help physicians differentiate typical ON from the atypical variants associated with more complex neurologic disorders.
Prognosis
The prognosis for patients with ON depends on the underlying etiology.
Short-term: Pain with eye movement usually resolves within days to weeks. Visual acuity and color perception improve over two weeks to three months, and nearly 90% of patients achieve near-normal function by six months. Only 3% of patients have BCVA of 20/200 or worse after 5 years [22].
Long-term: In 15-20% of cases optic neuritis precedes the development of multiple sclerosis [9],[10], and recurrent ON increases the risk of developing MS or neuromyelitis optica spectrum disorders (NMOSD) [7]. Approximately 50% of patients with MS have had at least one ON attack within the prior 15 years.
Pearls and Other Issues
To reduce the potential for visual impairment, neurologic disabilities, and physical limitations, optic neuritis must be recognized quickly and accurately.
Patients with acute optic neuritis and the following characteristics have a lower risk of developing multiple sclerosis:
- No demyelinating lesions on MRI.
- Optic disc swelling.
- Male gender.
Other causes of optic nerve disease should be considered when:
- Vision loss is bilateral, especially in older patients.
- Deterioration in visual due to presumed optic neuritis persists without improvement after five weeks.
- Vision loss is not accompanied by eye pain.
- Retinal hemorrhage or marked optic disc edema is present.
Enhancing Healthcare Team Outcomes
The management of the patient with optic neuritis (ON) requires the close coordination of a variety of healthcare professionals.
The initial treatment is managed by a neuro-ophthalmologist or a neurology team familiar with the guidelines derived by the Optic Neuritis Treatment Trial (ONTT).
The probability of developing multiple sclerosis (MS) within 15 years of the initial ON attack is 50%[10].
For patients with MS or at high risk for developing MS, an array of healthcare specialists come together to provide comprehensive care.
The healthcare team provides a wide range of services, some of which are listed below.
A complete team will include a combination of the following providers:
- Neurology team to manage the diagnosis and treatment.
- Neurologist
- Advanced practice professionals (APP)
- Nurse practitioners and advanced practice nurses (NP)
- Physician assistants (PA)
- Rehabilitation specialists to enhance strength, physical stability, and musculoskeletal function.
- Physical medicine and rehabilitation (PMR) physician management.
- Physical therapists (PT) to facilitate strength, balance, range of motion, and alleviate musculoskeletal pain.
- Occupational therapists (OT) to facilitate activities of daily living skills.
- Medical specialists
- Mental health specialists
- Psychiatrists/psychologists to manage mental health concerns.
- Clinical social workers to provide appropriate resources, advocate for patient rights.
- Neuro-ophthalmologists to manage visual deficiencies related to neurologic disease.
- Low vision specialists present aids to ameliorate the barriers inherent to diminished visual function.
- Urologists/gynecologists
- Mental health specialists
- Pharmacists to provide patient education and monitor the complex medication regimen.
- Primary care providers coordinate overall health status and manage concomitant conditions.
- Well-being professionals provide lifestyle modifications that benefit nutrition, fitness, and resilience.
Media
(Click Image to Enlarge)
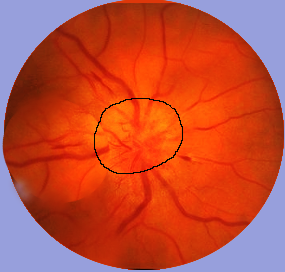
Optic Neuritis as an Indicator of Multiple Sclerosis. Optic neuritis can be visualized through fundoscopy, which may indicate the presence of multiple sclerosis.
Contributed by S Bhimji, MD
References
Soelberg K,Nilsson AC,Nielsen C,Jarius S,Reindl M,Wildemann B,Lillevang ST,Asgari N, Autoimmune and immunogenetic profile of patients with optic neuritis in a population-based cohort. Multiple sclerosis and related disorders. 2018 Apr; [PubMed PMID: 29544193]
Tuwir I,Dunne C,Crowley J,Saddik T,Murphy R,Cassidy L, The relationship between HLA-DRB1 alleles and optic neuritis in Irish patients and the risk of developing multiple sclerosis. The British journal of ophthalmology. 2007 Oct; [PubMed PMID: 17895416]
Zhao S,Zhou H,Peng X,Zhu J,Wang W,Kang H,Chen T,Xu Q,Wei S, Optic neuritis with positive HLA-B27: Characteristic phenotype in the Chinese population. Journal of the neurological sciences. 2016 Mar 15; [PubMed PMID: 26944126]
Martínez-Lapiscina EH,Fraga-Pumar E,Pastor X,Gómez M,Conesa A,Lozano-Rubí R,Sánchez-Dalmau B,Alonso A,Villoslada P, Is the incidence of optic neuritis rising? Evidence from an epidemiological study in Barcelona (Spain), 2008-2012. Journal of neurology. 2014 Apr; [PubMed PMID: 24532201]
Level 2 (mid-level) evidencePérez-Cambrodí RJ,Gómez-Hurtado Cubillana A,Merino-Suárez ML,Piñero-Llorens DP,Laria-Ochaita C, Optic neuritis in pediatric population: a review in current tendencies of diagnosis and management. Journal of optometry. 2014 Jul-Sep; [PubMed PMID: 25000867]
Lucchinetti CF,Kiers L,O'Duffy A,Gomez MR,Cross S,Leavitt JA,O'Brien P,Rodriguez M, Risk factors for developing multiple sclerosis after childhood optic neuritis. Neurology. 1997 Nov; [PubMed PMID: 9371931]
Level 2 (mid-level) evidenceSellner J,Boggild M,Clanet M,Hintzen RQ,Illes Z,Montalban X,Du Pasquier RA,Polman CH,Sorensen PS,Hemmer B, EFNS guidelines on diagnosis and management of neuromyelitis optica. European journal of neurology. 2010 Aug; [PubMed PMID: 20528913]
Shen T,You Y,Arunachalam S,Fontes A,Liu S,Gupta V,Parratt J,Wang C,Barnett M,Barton J,Chitranshi N,Zhu L,Fraser CL,Graham SL,Klistorner A,Yiannikas C, Differing Structural and Functional Patterns of Optic Nerve Damage in Multiple Sclerosis and Neuromyelitis Optica Spectrum Disorder. Ophthalmology. 2019 Mar; [PubMed PMID: 30060979]
S�rensen TL,Frederiksen JL,Br�nnum-Hansen H,Petersen HC, Optic neuritis as onset manifestation of multiple sclerosis: a nationwide, long-term survey. Neurology. 1999 Aug 11; [PubMed PMID: 10449106]
Level 3 (low-level) evidenceMultiple sclerosis risk after optic neuritis: final optic neuritis treatment trial follow-up. Archives of neurology. 2008 Jun; [PubMed PMID: 18541792]
Level 1 (high-level) evidenceSimpson S Jr,Blizzard L,Otahal P,Van der Mei I,Taylor B, Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. Journal of neurology, neurosurgery, and psychiatry. 2011 Oct; [PubMed PMID: 21478203]
Level 2 (mid-level) evidenceTao C,Simpson S Jr,van der Mei I,Blizzard L,Havrdova E,Horakova D,Shaygannejad V,Lugaresi A,Izquierdo G,Trojano M,Duquette P,Girard M,Grand'Maison F,Grammond P,Alroughani R,Terzi M,Oreja-Guevara C,Sajedi SA,Iuliano G,Sola P,Lechner-Scott J,Pesch VV,Pucci E,Bergamaschi R,Barnett M,Ramo C,Singhal B,LA Spitaleri D,Slee M,Verheul F,Fernández Bolaños R,Amato MP,Cristiano E,Granella F,Hodgkinson S,Fiol M,Gray O,McCombe P,Saladino ML,Sánchez Menoyo JL,Shuey N,Vucic S,Shaw C,Deri N,Arruda WO,Butzkueven H,Spelman T,Taylor BV, Higher latitude is significantly associated with an earlier age of disease onset in multiple sclerosis. Journal of neurology, neurosurgery, and psychiatry. 2016 Dec; [PubMed PMID: 27810919]
Rodriguez M,Siva A,Cross SA,O'Brien PC,Kurland LT, Optic neuritis: a population-based study in Olmsted County, Minnesota. Neurology. 1995 Feb; [PubMed PMID: 7854520]
Jurynczyk M,Messina S,Woodhall MR,Raza N,Everett R,Roca-Fernandez A,Tackley G,Hamid S,Sheard A,Reynolds G,Chandratre S,Hemingway C,Jacob A,Vincent A,Leite MI,Waters P,Palace J, Clinical presentation and prognosis in MOG-antibody disease: a UK study. Brain : a journal of neurology. 2017 Dec 1; [PubMed PMID: 29136091]
de Seze J, MOG-antibody neuromyelitis optica spectrum disorder: is it a separate disease? Brain : a journal of neurology. 2017 Dec 1; [PubMed PMID: 29194504]
Bermel RA,Balcer LJ, Optic neuritis and the evaluation of visual impairment in multiple sclerosis. Continuum (Minneapolis, Minn.). 2013 Aug; [PubMed PMID: 23917102]
Level 3 (low-level) evidenceBeck RW,Cleary PA,Backlund JC, The Course of Visual Recovery after Optic Neuritis: Experience of the Optic Neuritis Treatment Trial. Ophthalmology. 2020 Apr; [PubMed PMID: 32200819]
Longbrake EE,Lancia S,Tutlam N,Trinkaus K,Naismith RT, Quantitative visual tests after poorly recovered optic neuritis due to multiple sclerosis. Multiple sclerosis and related disorders. 2016 Nov; [PubMed PMID: 27919490]
Kahloun R,Abroug N,Ksiaa I,Mahmoud A,Zeghidi H,Zaouali S,Khairallah M, Infectious optic neuropathies: a clinical update. Eye and brain. 2015; [PubMed PMID: 28539795]
Beck RW,Cleary PA,Anderson MM Jr,Keltner JL,Shults WT,Kaufman DI,Buckley EG,Corbett JJ,Kupersmith MJ,Miller NR, A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. The New England journal of medicine. 1992 Feb 27; [PubMed PMID: 1734247]
Level 1 (high-level) evidenceBeck RW,Cleary PA, Optic neuritis treatment trial. One-year follow-up results. Archives of ophthalmology (Chicago, Ill. : 1960). 1993 Jun; [PubMed PMID: 8512477]
Level 1 (high-level) evidenceBeck RW,Cleary PA,Backlund JC, The course of visual recovery after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Ophthalmology. 1994 Nov; [PubMed PMID: 7800355]
Level 1 (high-level) evidenceLong DT,Beck RW,Moke PS,Blair RC,Kip KE,Gal RL,Katz BJ, The SKILL Card test in optic neuritis: experience of the Optic Neuritis Treatment Trial. Smith-Kettlewell Institute Low Luminance. Optic Neuritis Study Group. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2001 Jun; [PubMed PMID: 11450903]
Beck RW,Gal RL,Bhatti MT,Brodsky MC,Buckley EG,Chrousos GA,Corbett J,Eggenberger E,Goodwin JA,Katz B,Kaufman DI,Keltner JL,Kupersmith MJ,Miller NR,Moke PS,Nazarian S,Orengo-Nania S,Savino PJ,Shults WT,Smith CH,Trobe JD,Wall M,Xing D, Visual function more than 10 years after optic neuritis: experience of the optic neuritis treatment trial. American journal of ophthalmology. 2004 Jan; [PubMed PMID: 14700647]
Level 1 (high-level) evidenceKupersmith MJ,Gal RL,Beck RW,Xing D,Miller N, Visual function at baseline and 1 month in acute optic neuritis: predictors of visual outcome. Neurology. 2007 Aug 7; [PubMed PMID: 17679669]
Keltner JL,Johnson CA,Spurr JO,Beck RW, Comparison of central and peripheral visual field properties in the optic neuritis treatment trial. American journal of ophthalmology. 1999 Nov; [PubMed PMID: 10577521]
Keltner JL,Johnson CA,Cello KE,Dontchev M,Gal RL,Beck RW, Visual field profile of optic neuritis: a final follow-up report from the optic neuritis treatment trial from baseline through 15 years. Archives of ophthalmology (Chicago, Ill. : 1960). 2010 Mar; [PubMed PMID: 20212204]
Level 1 (high-level) evidenceRolak LA,Beck RW,Paty DW,Tourtellotte WW,Whitaker JN,Rudick RA, Cerebrospinal fluid in acute optic neuritis: experience of the optic neuritis treatment trial. Neurology. 1996 Feb; [PubMed PMID: 8614496]
Level 1 (high-level) evidenceBeck RW, Clinically definite multiple sclerosis following optic neuritis. Annals of neurology. 1997 Nov; [PubMed PMID: 9392585]
Level 3 (low-level) evidenceBeck RW,Trobe JD,Moke PS,Gal RL,Xing D,Bhatti MT,Brodsky MC,Buckley EG,Chrousos GA,Corbett J,Eggenberger E,Goodwin JA,Katz B,Kaufman DI,Keltner JL,Kupersmith MJ,Miller NR,Nazarian S,Orengo-Nania S,Savino PJ,Shults WT,Smith CH,Wall M, High- and low-risk profiles for the development of multiple sclerosis within 10 years after optic neuritis: experience of the optic neuritis treatment trial. Archives of ophthalmology (Chicago, Ill. : 1960). 2003 Jul; [PubMed PMID: 12860795]
Level 2 (mid-level) evidenceBeck RW,Smith CH,Gal RL,Xing D,Bhatti MT,Brodsky MC,Buckley EG,Chrousos GA,Corbett J,Eggenberger E,Goodwin JA,Katz B,Kaufman DI,Keltner JL,Kupersmith MJ,Miller NR,Moke PS,Nazarian S,Orengo-Nania S,Savino PJ,Shults WT,Trobe JD,Wall M, Neurologic impairment 10 years after optic neuritis. Archives of neurology. 2004 Sep; [PubMed PMID: 15364684]
Beck RW,Arrington J,Murtagh FR,Cleary PA,Kaufman DI, Brain magnetic resonance imaging in acute optic neuritis. Experience of the Optic Neuritis Study Group. Archives of neurology. 1993 Aug; [PubMed PMID: 8352671]
Level 1 (high-level) evidenceBeck RW, The optic neuritis treatment trial: three-year follow-up results. Archives of ophthalmology (Chicago, Ill. : 1960). 1995 Feb; [PubMed PMID: 7864737]
Level 3 (low-level) evidenceCleary PA,Beck RW,Bourque LB,Backlund JC,Miskala PH, Visual symptoms after optic neuritis. Results from the Optic Neuritis Treatment Trial. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 1997 Mar; [PubMed PMID: 9093956]
Level 2 (mid-level) evidenceVisual function 15 years after optic neuritis: a final follow-up report from the Optic Neuritis Treatment Trial. Ophthalmology. 2008 Jun; [PubMed PMID: 17976727]
Level 1 (high-level) evidenceBeck RW,Gal RL, Treatment of acute optic neuritis: a summary of findings from the optic neuritis treatment trial. Archives of ophthalmology (Chicago, Ill. : 1960). 2008 Jul; [PubMed PMID: 18625951]
Level 1 (high-level) evidenceKatz B,Trobe JD,Beck RW, The optic neuritis treatment trial: implications for clinicians. Seminars in ophthalmology. 1995 Sep; [PubMed PMID: 10159746]
Beck RW,Trobe JD, What we have learned from the Optic Neuritis Treatment Trial. Ophthalmology. 1995 Oct; [PubMed PMID: 9097798]
Level 1 (high-level) evidenceGal RL,Vedula SS,Beck R, Corticosteroids for treating optic neuritis. The Cochrane database of systematic reviews. 2012 Apr 18; [PubMed PMID: 22513900]
Level 1 (high-level) evidenceVedula SS,Brodney-Folse S,Gal RL,Beck R, Corticosteroids for treating optic neuritis. The Cochrane database of systematic reviews. 2007 Jan 24; [PubMed PMID: 17253459]
Level 1 (high-level) evidence