Introduction
Os peroneum is one of several accessory ossicles of the foot and ankle, located lateral to the cuboid within the distal peroneus longus tendon.[1] Like most accessory ossicles, os peroneum is generally asymptomatic and detected incidentally on imaging, though its intratendinous location can result in its involvement in pathologies affecting the peroneus longus tendon. Painful os peroneum syndrome is a general term referring to conditions presenting as lateral midfoot pain associated with the os peroneum, such as acute fracture, stress fracture related to chronic repetitive trauma, contusion, avascular necrosis, or tendinosis, tenosynovitis, tendon tears, and subluxation involving the peroneal tendons. Other causes of lateral midfoot pain also include ligamentous injury (talofibular or calcaneofibular), fractures of the base of the fourth or fifth metatarsal bone, anterior calcaneus, or cuboid.[2][3]
Routine foot radiographs are a common first step in assessing lateral midfoot pain. Abnormalities in the morphology and location of the os peroneum can easily be identified on radiographs, specifically the oblique view, thereby elevating clinical suspicion for a peroneus longus tendon injury.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Accessory ossicles are common, generally asymptomatic, normal variants seen throughout the musculoskeletal system, with several examples within the foot and ankle. Awareness of their presence and location is essential to limit the misdiagnosis of these normal variants for pathology. The origin of many of these ossicles is debated in the literature. One proposed mechanism is from the non-union of secondary ossification centers.[5] However, a recent cadaveric study suggests that a precursor of the os peroneum is present in the fetal period in some patients. Additionally, experts have proposed that the os peroneum develops as a response to local stresses within the tendon.[6][7] A fibrocartilaginous node is a fibrous, non-ossified structure analogous to the os peroneum appreciated on MRI as a focal T1/T2 hypointense oval structure within the peroneus longus tendon.[2][8]
Ossicles and sesamoids are known to be associated with painful symptoms such as the os navicular, os trigonum, and hallux sesamoids.[2] Likewise, the os peroneum can be symptomatic or associated with pathology. Painful os peroneum syndrome is described as lateral foot pain, which may be attributed to several causes, including acute os peroneum fracture, peroneal tendon rupture, and chronic tendinopathy.[9][10] Fractures of the os peroneum may be associated with peroneus longus tendon rupture in the acute setting or may be associated with chronic degeneration and tendinopathy.[1] Acute fracture of the os peroneum is most commonly caused by strong contraction of the peroneus longus muscle with associated inversion or supination.
Epidemiology
Among the numerous foot and ankle ossicles, os peroneum is relatively common, with prevalence figures ranging from 5% to 30%.[5] A bilateral presentation may be noted in 60% of adults with os peroneum. Bipartite/multipartite appearance has been reported in up to 30% of cases.[11] The peroneus quartus is a common accessory muscle seen along the posterolateral foot with an incidence ranging from 6% to 21%, also implicated in lateral foot/ankle pain in some patients.[3]
Inversion injuries to the foot and ankle are a common cause of patient presentation to the emergency department. The ankle joint is the most commonly injured joint in the extremities, and lateral ankle sprains are the most common traumatic joint disorder.[3] Most patients respond to conservative treatment in the absence of a fracture; however, 10% to 20% will have continued pain and instability.[3] When patients do not respond to conservative treatment and ligamentous instability is not evident on exam findings, the peroneus tendon and os peroneum should be considered. Failure to consider alternative, less common etiologies can lead to a delayed diagnosis.
History and Physical
Os peroneum is typically asymptomatic but can be fractured or displaced in the setting of a peroneus longus tendon tear, either from direct injury or indirectly from abrupt foot dorsiflexion or inversion.[1][10] Os peroneum fractures may present in the setting of an acute traumatic injury or with chronic symptoms, occasionally without a known history of trauma.[9][10] Presenting symptoms often include lateral foot/ankle pain, instability, swelling, and tenderness to palpation.[5][9]
Physical examination findings related to a peroneus longus tear include edema, tenderness, and weakness in eversion and plantar flexion.[4][5][12] Evaluation for cavovarus alignment on standing examination of the patient may also be beneficial, given a known association of peroneal tendon abnormalities with hindfoot varus.[12]
Evaluation
Os peroneum is identified radiographically as an oval or round well-corticated accessory ossicle adjacent to the cuboid, near the calcaneocuboid joint, and is best seen on oblique views of the foot .[12][5][9] A bipartite or multipartite os peroneum will demonstrate a fragmented appearance, but its well-corticated, smooth borders can help distinguish it from a fracture, which will demonstrate sharp, irregular, jagged margins.[1][10][12] Fragment separation of greater than 6 mm is suggestive of os peroneum fracture with an associated tendon tear, while a separation of 2 mm or less can be seen in non-displaced fractures or normal variant bipartite os peroneum (see Image. Oblique Left Foot Radiograph Demonstrates a Fragmented Os Peroneus).[11] Chronic stress injury to the os peroneum can manifest as an enlarged, sclerotic ossicle.[10] An intact os peroneum that has changed in position relative to a comparison radiograph, proximal to the calcaneocuboid joint, may be seen in peroneal tendon rupture with retraction.[13]
Distinguishing between a bipartite or multipartite os peroneum and a fracture can be difficult on radiographs, specifically in the absence of a prior comparison study. Since the os peroneum is commonly bilateral, radiographs of the contralateral foot can sometimes be enlightening. In challenging cases, CT can provide a more detailed evaluation of osseous margins allowing for the distinction between a non-displaced fracture versus a bipartite or multipartite os peroneum.[10]
On ultrasound, the os peroneum, if present, may be seen as a hyperechoic structure with posterior shadowing, with only its outer cortex visible; it is best evaluated by following the peroneus longus tendon distal to the peroneal tubercle of the calcaneus.[10] A fractured os peroneum may sonographically demonstrate an elongated appearance or irregular cortical contours.[4][11] Associated pathology of the peroneus longus tendon may demonstrate fluid in the tendon sheath as well as a hypoechoic enlargement in tendinosis or a hypoechoic/anechoic cleft within the tendon in the case of a partial tear.[4][11][12] A complete peroneus longus tear may show a disrupted tendon and/or retraction.[11] Comparison with the contralateral tendon side can aid in the diagnosis of tendinosis. Additionally, peroneal subluxation associated with injury to the superior peroneal retinaculum can be demonstrated on ultrasound with provocative maneuvers.[3]
Magnetic resonance imaging of the os peroneus will demonstrate marrow characteristics similar to the cuboid, with a hyperintense signal on T1-weighted and a hypointense signal on T2-weighted fat-suppressed sequences.[10] An unossified fibrocartilaginous node in place of a fully-formed os peroneus is a deceptive mimic of a peroneus longus tendon tear due to the node’s intermediate signal on all sequences.[10] Injury of the os peroneus can result in edematous marrow changes, hypointense on T1 sequences, and hyperintense on T2 fat-suppressed sequences, though the os peroneus itself may be difficult to visualize.[10][13] Assessment of the cortex is best performed using radiography and/or CT.[10] MR is useful in the assessment of associated peroneus longus tendon injury and may show hyperintense intratendinous signal on T1, and T2 fat-suppressed sequences, fluid within the tendon sheath, abnormal morphology (tendon enlargement, flattening, or chevron shape), and partial/complete tendon discontinuity may also be noted.[10][13]
A classification scheme has been developed to describe peroneus longus tendon injuries and helps describe/explain the radiographic appearance of the os peroneum. The tears have been divided into three subtypes: proximal to the os peroneum (type 1), at the level of the os peroneum (type 2), or distal to the os peroneum (type 3). Isolated tears of the peroneus longus tendon proximal to the os peroneum generally present as an os peroneum with normal morphology and position. Type 2 tears occurring at the os peroneum are normally associated with fractures or distraction of bi- or multipartite fragments. Distraction of the os peroneum fragments greater than 6 mm is highly suspicious for complete disruption of the peroneus longus tendon. If comparison radiographs are available, the new or increasing distraction of the fragments is concerning for tendon injury (partial or complete depending on the extent of distraction). When the tendon injury is distal to the os peroneum, it can be displaced proximally. The ossicle is rarely displaced proximally to the peroneus tubercle (< 2 cm) along the lateral margin of the calcaneus unless there is a strong contraction force of the tendon. It should be noted that in the acute setting, the os peroneum may not be displaced or only minimally displaced; however, short interval follow-up may show new or increasing displacement as the torn tendon continues to retract.[14]
Treatment / Management
Treatment options are focused on the pathology of the peroneus longus tendon, which is typically managed conservatively via immobilization, oral anti-inflammatories (NSAIDs), and/or steroid injections and may be followed with a course of physical therapy.[4][1][3][13] Surgical treatment may be performed after the failure of conservative methods or in the event of intractable pain or impaired function.[13] Early surgical intervention may also be considered in high-level athletes. Surgical options include primary tendon repair or grafting, excision of the fractured os peroneum if present with tendon repair or tenodesis, internal fixation of the fractured os peroneum, or tendon debridement/tenosynovectomy.[13][15] (B2)
The type of surgical intervention will depend on the location and extent of the tendon injury.[15] One proposed algorithm for surgical management of peroneal tendon injuries classifies patients into three categories: type 1, both tendons intact; type 2, one tendon is torn, the other intact; type 3, both tendons are torn. In this algorithm, type 1 patients undergo primary repair, type 2 tenodesis, and type 3 tendon transfer.[16](B2)
Differential Diagnosis
A presenting symptom of lateral foot pain and/or ankle instability elicits a broad range of possible etiologies, including peroneal tendinopathy or subluxation, lateral ankle ligamentous injury (including the anterior and posterior talofibular and the calcaneofibular ligaments), sinus tarsi syndrome, cuboid syndrome, osseous fractures, and peroneal neuropathy, among numerous other considerations.[16] A peroneal tendon injury may be overlooked in favor of a lateral ankle ligament injury and should be considered in a patient with persistent pain.[16][17] Magnetic resonance imaging provides an optimal anatomic evaluation of the lateral ankle structures and thus can be particularly helpful in elucidating the etiology. See Image. Lateral Ankle Radiograph, Os Peroneum.
As previously explained, an os peroneum fracture may be confused with a bipartite/multipartite os peroneum.[1][10][12] An os vesalianum and os cuboideum secundarium are other accessory ossicles that can be found near the expected location of an os peroneum.[5] In a distal peroneus longus tendon rupture, the os peroneum with extreme proximal displacement can be confused with an os trigonum.[4][14] Additional considerations include a fracture of the adjacent cuboid or an avulsion fracture from the base of the fifth metatarsal.[4]
Prognosis
Insufficient high-quality evidence exists for determining the efficacy of conservative and surgical therapies for peroneal tendon injuries. However, select studies of post-surgical outcomes showed figures such as 87% of patients returning to sporting activities within 3.5 months of surgery and 91% achieving normal/moderate peroneal strength.[12]
Complications
Patients with suspected or diagnosed peroneal tendon injuries may experience chronic lateral foot/ankle pain and instability with a lack of treatment or after the failure of conservative therapies. Delays in diagnosis are not uncommon, with one study reporting the duration of symptoms persisting from 7 to 48 months before the correct diagnosis was made.[12]
An untreated os peroneus fracture can result in degeneration and tearing of the peroneus longus tendon related to chronic frictional forces.[1] In patients with repeat ankle injuries in the setting of a peroneal tendon rupture, serial radiographs may demonstrate the migration of the os peroneum if intact or, if fractured, diastasis of the fracture fragments.[9][10]
Intraoperative findings during repair of a primary peroneus longus tendon injury and associated os peroneum abnormality often include the discovery of additional tendinous and/or osseous pathologies, such as peroneus brevis tear, hypertrophied peroneal tubercle of the calcaneus, and subluxation or dislocating peroneal tendons.[15]
Insufficient data exist regarding the efficacy of surgical treatments. However, reported postoperative complications of repair of peroneal tendon rupture include superficial wound infection, wound dehiscence, repair failure, sural neuritis, adhesive tendinitis, and chronic regional pain syndrome.[17]
Consultations
- Podiatrists
- Orthopedic surgeons
- Physical therapists
- Pedorthists
- Sports medicine clinicians
Deterrence and Patient Education
Os peroneum is an accessory ossicle bone, or “extra bone,” in the foot. It is found next to the cuboid bone and within the peroneus longus tendon in the lateral region of the foot. While they are generally painless, pathological conditions such as fractures, tendonitis, or tendon tears of the peroneus longus related to this accessory ossicle are generally referred to as os peroneum syndrome. A radiograph of the affected foot and possibly an ultrasound or MRI are often necessary to determine the extent of bone and soft tissue involvement. Symptoms of os peroneum syndrome include swelling, tenderness, and instability to the outside of the foot with weakness in eversion and plantarflexion of the foot.
Conservative treatment is usually attempted first, focusing on the peroneus longus tendon pathology, with immobilization, oral anti-inflammatories, steroid injections, and physical therapy. Surgical management is considered in severe pain, debilitation, or failed conservative therapy. Surgical options include primary tendon repair or grafting, excision of the fractured os peroneum if present with tendon repair or tenodesis, internal fixation of the fractured os peroneum, or tendon debridement/tenosynovectomy.
Patients can benefit from a directed home exercise program and, in some cases, wearing orthotics; this can prevent exacerbation of existing cases and occasionally help mitigate symptoms. If os peroneum is found incidentally, these measures can help patients prevent it from becoming symptomatic.
Pearls and Other Issues
- Evaluation of foot radiographs in patients with lateral foot and/or ankle pain should include an assessment of the presence and morphology of an os peroneum, particularly on oblique views.
- Correlation with past imaging and with radiographs of the contralateral side can be useful in assessing for ossicle migration, asymmetry in the setting of chronic stress injury, or whether a fragmented appearance represents a bipartite/multipartite os peroneum versus an acutely fractured ossicle.
- Abnormalities in the os peroneum are suggestive of associated peroneal tendon injury.
- There are numerous causes of lateral foot pain, with delays in diagnosis not uncommon.
Enhancing Healthcare Team Outcomes
Clinical or radiologic suspicion for a peroneal tendon injury with or without an os peroneus fracture may warrant consultation with a podiatrist or orthopedic surgeon and/or advanced imaging (MRI or ultrasound), specifically in the setting of patients that failed conservative therapy. Nurses and physical therapists are also valuable assets in caring for these patients. These healthcare professionals need to function as a cohesive interprofessional team. Operative outcomes are based on level-IV and level-V studies. Thus, an interprofessional approach individualized to the patient’s case and involving a primary care provider, an orthopedic surgeon, a radiologist, and a physical therapist will provide the most optimal course of treatment.[17]
Media
(Click Image to Enlarge)

Lateral Ankle Radiograph, Os Peroneum
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
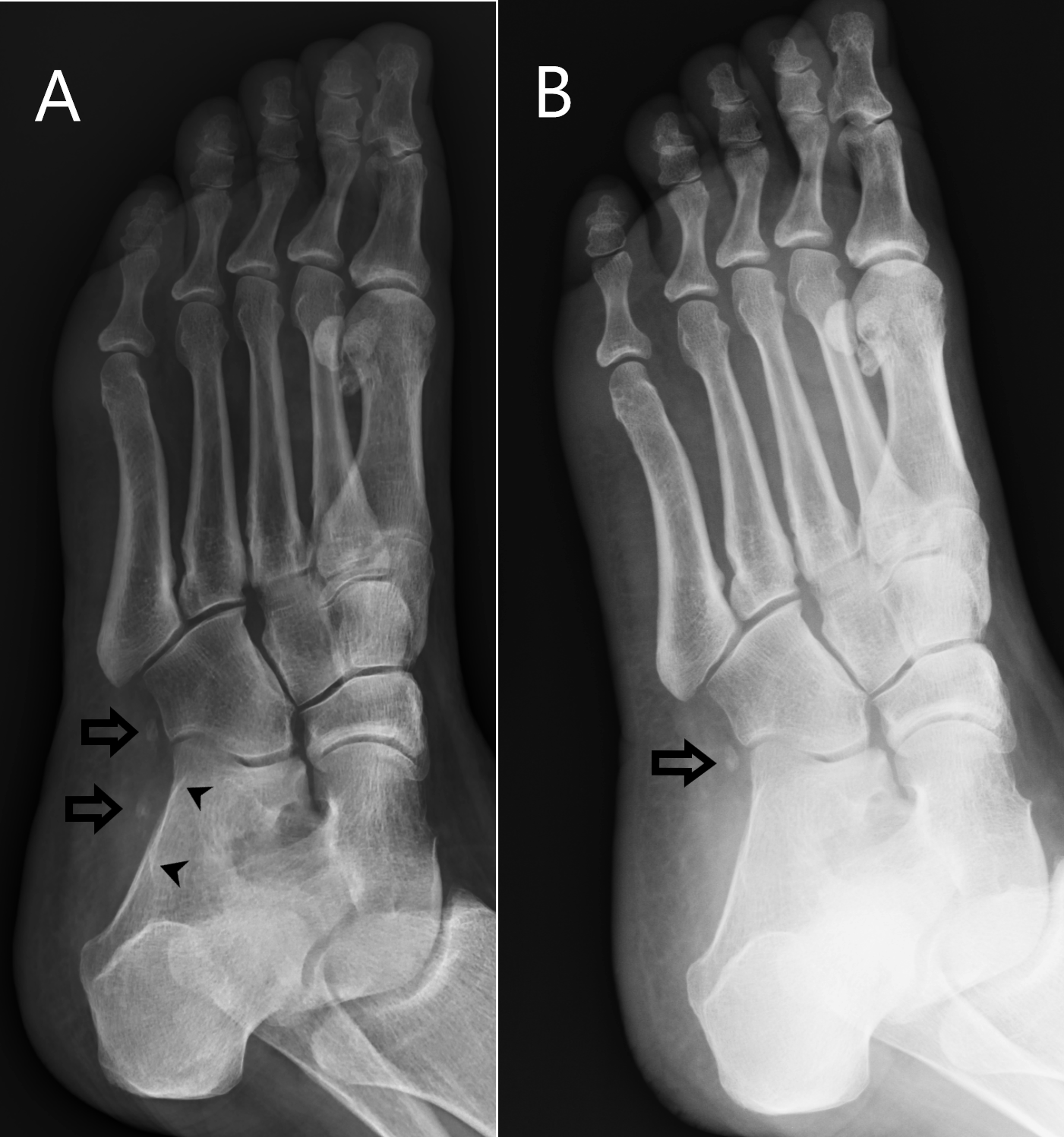
Oblique Left Foot Radiograph Demonstrates a Fragmented Os Peroneus. (A) Oblique left foot radiograph demonstrates a fragmented os peroneus (arrows) with 12 mm distraction of a proximal fracture fragment to the level of the peroneal tubercle, a curved prominence on the lateral aspect of the calcaneus (arrowheads). A peroneal tendon injury is suggested with distraction of os peroneus fracture fragments greater than 6 mm, or with migration of an os peroneus proximal to the peroneal tubercle. A subsequent foot MRI of this patient demonstrated a complete peroneal tendon tear with proximal retraction of tendon fibers. (B) Radiographs of the same patient 7 years prior demonstrate an intact os peroneus distal to the peroneal tubercle (arrow).
Contributed by D Byerly, MD
References
Peterson JJ, Bancroft LW. Os peroneal fracture with associated peroneus longus tendinopathy. AJR. American journal of roentgenology. 2001 Jul:177(1):257-8 [PubMed PMID: 11418450]
Level 3 (low-level) evidenceChagas-Neto FA, de Souza BN, Nogueira-Barbosa MH. Painful Os Peroneum Syndrome: Underdiagnosed Condition in the Lateral Midfoot Pain. Case reports in radiology. 2016:2016():8739362. doi: 10.1155/2016/8739362. Epub 2016 Jul 5 [PubMed PMID: 27478674]
Level 3 (low-level) evidenceSmith JT, Johnson AH, Heckman JD. Nonoperative treatment of an os peroneum fracture in a high-level athlete: a case report. Clinical orthopaedics and related research. 2011 May:469(5):1498-501. doi: 10.1007/s11999-011-1812-3. Epub 2011 Feb 17 [PubMed PMID: 21328020]
Level 3 (low-level) evidenceSpontaneous Fracture of the Os Peroneum With Rupture of the Peroneus Longus Tendon., Schick F,Karanjia H,Daniel J,Dheer S,Langman C,Taweel N,Sullivan P,Lebaron T,, The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons, 2018 Jul - Aug [PubMed PMID: 29631970]
Keles-Celik N, Kose O, Sekerci R, Aytac G, Turan A, Güler F. Accessory Ossicles of the Foot and Ankle: Disorders and a Review of the Literature. Cureus. 2017 Nov 26:9(11):e1881. doi: 10.7759/cureus.1881. Epub 2017 Nov 26 [PubMed PMID: 29387510]
Mittal PS, Joshi SS, Chhaparwal R, Joshi SD. Prevalence and Mophometry of Os Peroneum amongst Central Indians. Journal of clinical and diagnostic research : JCDR. 2014 Nov:8(11):AC08-10. doi: 10.7860/JCDR/2014/10452.5079. Epub 2014 Nov 20 [PubMed PMID: 25584203]
Guimerá V, Lafuente A, Zambrana L, Rodriguez-Niedenführ M, Sañudo JR, Vazquez T. The peroneocuboid joint: morphogenesis and anatomical study. Journal of anatomy. 2015 Jan:226(1):104-12. doi: 10.1111/joa.12249. Epub 2014 Nov 10 [PubMed PMID: 25384452]
Didolkar MM,Malone AL,Nunley JA 2nd,Dodd LG,Helms CA, Pseudotear of the peroneus longus tendon on MRI, secondary to a fibrocartilaginous node. Skeletal radiology. 2012 Nov; [PubMed PMID: 22349597]
Level 2 (mid-level) evidenceBrigido MK, Fessell DP, Jacobson JA, Widman DS, Craig JG, Jamadar DA, van Holsbeeck MT. Radiography and US of os peroneum fractures and associated peroneal tendon injuries: initial experience. Radiology. 2005 Oct:237(1):235-41 [PubMed PMID: 16183934]
Level 2 (mid-level) evidenceFavinger JL, Richardson ML, Chew FS. Progressive retraction of a fractured os peroneum suggesting repetitive injury to the peroneus longus tendon. Radiology case reports. 2018 Feb:13(1):216-219. doi: 10.1016/j.radcr.2017.11.006. Epub 2017 Dec 9 [PubMed PMID: 29487659]
Level 3 (low-level) evidenceSmania L, Craig JG, von Holsbeeck M. Ultrasonographic findings in peroneus longus tendon rupture. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2007 Feb:26(2):243-6 [PubMed PMID: 17255188]
Level 3 (low-level) evidenceBrodsky JW,Zide JR,Kane JM, Acute Peroneal Injury. Foot and ankle clinics. 2017 Dec; [PubMed PMID: 29078831]
Vethanayagamony T, Patel H, Lomasney LM, Demos TC, Rottier FJ. What's your diagnosis? Migration of the Os peroneum associated with rupture of the peroneus longus tendon. Orthopedics. 2013 Oct 1:36(10):741, 807-10. doi: 10.3928/01477447-20130920-01. Epub [PubMed PMID: 24093685]
Level 3 (low-level) evidenceBianchi S, Bortolotto C, Draghi F. Os peroneum imaging: normal appearance and pathological findings. Insights into imaging. 2017 Feb:8(1):59-68. doi: 10.1007/s13244-016-0540-3. Epub 2017 Jan 5 [PubMed PMID: 28058662]
Stockton KG, Brodsky JW. Peroneus longus tears associated with pathology of the os peroneum. Foot & ankle international. 2014 Apr:35(4):346-52. doi: 10.1177/1071100714522026. Epub 2014 Feb 6 [PubMed PMID: 24505044]
Level 2 (mid-level) evidenceChoudhary S,McNally E, Review of common and unusual causes of lateral ankle pain. Skeletal radiology. 2011 Nov; [PubMed PMID: 20972871]
Heckman DS, Reddy S, Pedowitz D, Wapner KL, Parekh SG. Operative treatment for peroneal tendon disorders. The Journal of bone and joint surgery. American volume. 2008 Feb:90(2):404-18. doi: 10.2106/JBJS.G.00965. Epub [PubMed PMID: 18245603]