Introduction
An external cardiac pacemaker, or a transcutaneous or artificial, is an electrodes-based medical device that regulates myocardiocyte contractility to maintain adequate heart rate and cardiac output. While pathologic bradyarrhythmias occur for a variety of reasons, clear indications exist for the use of external or transcutaneous pacing. This topic discusses those indications and other modalities that can be used alongside external pacing as potentially life-saving treatment. Technical details of external pacing and a comprehensive review of studies examining external pacing are also included in the discussion.[1][2][3] Although this emergency treatment is life-saving, it can not be relied upon for an extended duration. A transvenous pacing or other permanent treatment should replace this temporary bridge to maintain hemodynamic balance.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Normal electrical conduction through the heart originates in the sinoatrial node. This is located in the superior aspect of the right atrium. Conduction then spreads through the atrium to the atrioventricular node at the inferior portion of the right atria. From there, it travels down the His bundle, followed by the right and left bundle branches in the interventricular septum. Lastly, it spreads across the ventricles via the Purkinje fibers. While in external cardiac pacing, pacer pads activate a focal point in the left ventricle. Electricity then spreads to the rest of the ventricular myocardium from that focal point. Direct capture of the atria is very difficult to obtain regardless of pad placement. Indirect capture can occasionally be obtained via retrograde conduction through the atrioventricular node. Compared to normal atrioventricular pacing, transcutaneous cardiac pacing provides greater cardiac output due to strong diaphragmatic and skeletal muscle contractions despite decreased left ventricular systolic pressure and a reduced stroke index.[4]
Indications
External pacing is the fastest way to synchronize cardiac rhythm in all bradyarrhythmias, as the American Heart Association (AHA) indicates.[5] This temporary method maintains cardiac output in all those irreversible conditions requiring a permanent pacemaker or those reversible situations where permanent pacing is contraindicated (see Image. Pacemaker Table).[6] Bradycardia is a heart rate of less than 60 beats per minute. However, not all cases of bradycardia require pacing. Rather, transcutaneous pacing should only be applied in situations that include systolic blood pressure less than 90, heart rate less than 40, or if an arrhythmia compromises organ perfusion. Before the initiation of pacing, atropine can be given to improve or reverse the bradycardia. Standard dosing is 0.5 milligrams intravenously. However, larger doses can be given to a patient who shows no improvement with the standard dose.
External pacing can be done in patients having Atrioventricular Nodal dysfunction caused by an acute myocardial infarction, chest or cardiac trauma, infections (Lyme disease or bacterial endocarditis), sepsis, etc. Bradycardic patients secondary to electrolyte disturbances, metabolic abnormalities, drugs (such as beta-blockers), or hypothermia are also strong candidates for this pacing method.[7] It is important to emphasize that external pacing never replaces permanent invasive transvenous pacing. Third-degree heart block, a particular type of AV block characterized by an unstable rhythm with a high risk of degeneration to ventricular tachycardia or ventricular fibrillation, is also an indication of transcutaneous pacing.
Certain cases of ventricular tachycardia such as postoperative atrial flutter, Torsades de Pointes may also be improved with external pacing after all other options have been exhausted. Recurrence of the arrhythmia was prevented from recurring in 14 of 16 cases using transcutaneous overdrive pacing.[8][9][10]
Contraindications
Generally, cardiac pacing should not be considered in asymptomatic hemodynamically stable patients to treat bradycardia. No definitive contraindications exist for external pacing when clinically indicated.[11] Some negative sequelae associated with cardioversion have been seen. These outcomes include failure of an implanted ventricular lead and an implanted atrial lead. While these adverse reactions are from a very limited number of cases secondary to cardioversion, it is possible to extrapolate that external pacing may result in the same complications.
Preparation
If possible, the skin should be prepared before placing the pacer pads. Hair should be removed but not shaved, as this can create a nidus for infection. The skin should be cleansed with an alcohol wipe to remove dirt, debris, or sweat whenever possible to ensure maximum conduction between the pads and the skin.
Technique or Treatment
Pacing pads are positioned on the patient's chest in either anterolateral or anteroposterior. Multiple variations of pacer pad placement are equally effective. "Negative electrode in the left parasternal region, the positive electrode in the right subscapular region; a negative electrode in the left parasternal region, a positive electrode in the left subscapular region; or negative electrode at the cardiac apex or the position of lead V3, a positive electrode in the right parasternal region." As long as the apical/anterior pad is negative, precise electrode placement is not essential. The rate should be set between 60 to 90 beats per minute with the electrical output, also known as the current, set to its lowest setting. The rate should slowly increase until a pacer spike is seen on the monitor. Continue to increase the rate until a QRS complex follows each spike. This indicates electrical capture. Confirmation of mechanical capture should be done by feeling for a pulse. Mechanical capture can also be confirmed using ultrasound and observing ventricular contraction. If the patient is conscious, little sedation can reduce discomfort associated with cardiac pacing.[12]
Complications
Pacing may significantly reduce stroke volume in subjects with normal left ventricular function. This change was also seen in patients with heart failure. Both external and internal pacing reduced ejection fraction. There were no significant differences between the reduction caused by external pacing and the internal reduction caused by pacing. The rate of pacing can be increased to maintain approximate cardiac output.
Side effects of transcutaneous pacing include cutaneous burns and muscle contractions. Superficial injury from the pacing pads resembles mild folliculitis. It is well known that muscle contractions can be extremely painful. To the point that sedation/anesthesia may be required. While the muscle contractions can be painful, no skeletal or myocardial muscle injury (as measured by CK, CK-MB, and troponin blood levels) developed after 30 minutes of pacing at 38 to 70mA with rates 10-20% above resting heart rate. Most cases of cutaneous burns are mild. However, many cases of third-degree burns have been reported in neonates, children, and geriatric age groups after cardiac pacing.[13][14] The risk of burns likely increases when pacer pads are used against manufacture instructions and are reapplied for multiple uses.
Two promising new ways of non-invasive pacing are currently being studied to mitigate the side effects of transcutaneous pacing techniques. The first uses high-intensity frequency ultrasound to stimulate pacing. The second uses iron microparticles injected intravenously and a generated magnetic field to pace in a concept known as mechano-electrical feedback.[10][15]
Clinical Significance
External pacing is 1 of the quickest and easiest methods for treating multiple conduction abnormalities. Everything from bradycardia to ventricular tachycardia can be managed with external pacing until definitive treatment can be implemented. Furthermore, it can be used under various circumstances, ranging from drug-induced electrical disturbances to conduction system inhibition secondary to myocardial infarction. It can be applied in the hospital setting or used by emergency medical service (EMS) providers when transporting critically ill patients to maintain an adequate cardiac output to ensure enough organ perfusion.[6]
Enhancing Healthcare Team Outcomes
External pacing is a procedure that is sometimes required on the medical and surgical floors. Clinicians must closely monitor the patients; to do so, they must be familiar with external pacing and its indications. Before the pacing is initiated, the patient should be educated about potential complications such as burns or failure to capture. The patient should also be informed about the potential discomfort of tingling or small shock-like nerve impulses. The clinician has to be fully aware that transcutaneous pacing may not always work and must be prepared to have a transvenous pacer system kit and atropine at the bedside. Finally, the clinician should ensure that no person may use their mobile phones or other electronic devices near the patient as this may interfere with the pacing unit. An appropriate warning sign needs to be placed on the door.[16][17][18] Studies have shown that the hemodynamic effects are similar between external and internal right ventricular pacing. However, currently available studies do not show that transcutaneous pacing improves patient outcomes. The data available is very limited. Most studies available have sample sizes of less than 150 patients and the time to apply the pacing was over 20 minutes. Larger studies with earlier application times are needed to confirm the effect of transcutaneous pacing on patient outcomes.[19] Healthcare outcomes can also be improved by good coordination and communication between the health professional team. A strong doctor-patient relationship must be there.
Media
(Click Image to Enlarge)
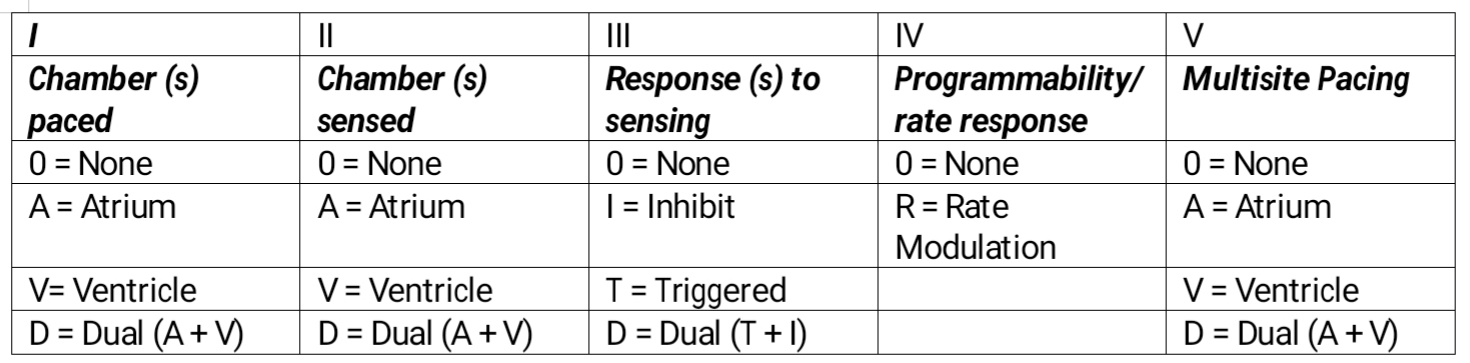
Pacemaker Table. External pacing is the fastest available method to synchronize cardiac rhythm in all the bradyarrhythmias indicated by the American Heart Association. This temporary method is used to maintain cardiac output in all those irreversible conditions where there is a need for a permanent pacemaker or those reversible situations where permanent pacing is contraindicated.
Contributed by M Ellison, MD, FASA
References
Kashou AH, Braiteh N, Kashou HE. Reversible atrioventricular block and the importance of close follow-up: Two cases of Lyme carditis. Journal of cardiology cases. 2018 May:17(5):171-174. doi: 10.1016/j.jccase.2018.01.001. Epub 2018 Feb 13 [PubMed PMID: 30279884]
Level 3 (low-level) evidencePuette JA, Malek R, Ellison MB. Pacemaker. StatPearls. 2024 Jan:(): [PubMed PMID: 30252257]
Halbfass P, Sonne K, Nentwich K, Ene E, Deneke T. Current developments in cardiac rhythm management devices. Clinical research in cardiology : official journal of the German Cardiac Society. 2018 Aug:107(Suppl 2):100-104. doi: 10.1007/s00392-018-1313-4. Epub 2018 Jun 27 [PubMed PMID: 29951805]
Feldman MD, Zoll PM, Aroesty JM, Gervino EV, Pasternak RC, McKay RG. Hemodynamic responses to noninvasive external cardiac pacing. The American journal of medicine. 1988 Mar:84(3 Pt 1):395-400 [PubMed PMID: 3348243]
Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Faxon DP, Halperin JL, Hiratzka LF, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW, American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices), American Association for Thoracic Surgery, Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008 May 27:117(21):e350-408. doi: 10.1161/CIRCUALTIONAHA.108.189742. Epub 2008 May 15 [PubMed PMID: 18483207]
Level 1 (high-level) evidenceMurdock DK, Moran JF, Speranza D, Loeb HS, Scanlon PJ. Augmentation of cardiac output by external cardiac pacing: pacemaker-induced CPR. Pacing and clinical electrophysiology : PACE. 1986 Jan:9(1 Pt 1):127-9 [PubMed PMID: 2419842]
Level 3 (low-level) evidenceHo JD, Heegaard WG, Brunette DD. Successful transcutaneous pacing in 2 severely hypothermic patients. Annals of emergency medicine. 2007 May:49(5):678-81 [PubMed PMID: 17141142]
Level 3 (low-level) evidenceDalia T, Amr BS. Pacemaker Indications. StatPearls. 2024 Jan:(): [PubMed PMID: 29939600]
Leong D, Sovari AA, Ehdaie A, Chakravarty T, Liu Q, Jilaihawi H, Makkar R, Wang X, Cingolani E, Shehata M. Permanent-temporary pacemakers in the management of patients with conduction abnormalities after transcatheter aortic valve replacement. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2018 Jun:52(1):111-116. doi: 10.1007/s10840-018-0345-z. Epub 2018 Mar 12 [PubMed PMID: 29532275]
Mulpuru SK, Madhavan M, McLeod CJ, Cha YM, Friedman PA. Cardiac Pacemakers: Function, Troubleshooting, and Management: Part 1 of a 2-Part Series. Journal of the American College of Cardiology. 2017 Jan 17:69(2):189-210. doi: 10.1016/j.jacc.2016.10.061. Epub [PubMed PMID: 28081829]
Zoll PM, Zoll RH, Falk RH, Clinton JE, Eitel DR, Antman EM. External noninvasive temporary cardiac pacing: clinical trials. Circulation. 1985 May:71(5):937-44 [PubMed PMID: 3886190]
Level 3 (low-level) evidenceThomas SP, Thakkar J, Kovoor P, Thiagalingam A, Ross DL. Sedation for electrophysiological procedures. Pacing and clinical electrophysiology : PACE. 2014 Jun:37(6):781-90. doi: 10.1111/pace.12370. Epub 2014 Feb 20 [PubMed PMID: 24697803]
Singleton MJ, Schoenfeld MH, Bhave PD, Beaty EH, Whalen SP. Third-degree burns caused by transcutaneous pacing for third-degree heart block. HeartRhythm case reports. 2020 Aug:6(8):495-498. doi: 10.1016/j.hrcr.2020.05.006. Epub 2020 May 18 [PubMed PMID: 32817826]
Walund DC, Lynn AM, Hall DG. A third-degree burn associated with external cardiac pacing in a five-year-old boy. The Journal of thoracic and cardiovascular surgery. 1992 Dec:104(6):1754-5 [PubMed PMID: 1453745]
Level 3 (low-level) evidenceFilipovic K, Bellmann B, Lüker J, Steven D, Sultan A. External electrical cardioversion of persistent atrial fibrillation in a patient with a Micra™ Transcatheter Pacing System. Indian pacing and electrophysiology journal. 2018 Jan-Feb:18(1):44-46. doi: 10.1016/j.ipej.2017.12.002. Epub 2017 Dec 18 [PubMed PMID: 29269168]
Kawata H, Pretorius V, Phan H, Mulpuru S, Gadiyaram V, Patel J, Steltzner D, Krummen D, Feld G, Birgersdotter-Green U. Utility and safety of temporary pacing using active fixation leads and externalized re-usable permanent pacemakers after lead extraction. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2013 Sep:15(9):1287-91. doi: 10.1093/europace/eut045. Epub 2013 Mar 12 [PubMed PMID: 23482613]
Sahinoglu E, Wool TJ, Wool KJ. Failure of communication and capture: The perils of temporary unipolar pacing system. Journal of arrhythmia. 2015 Jun:31(3):167-9. doi: 10.1016/j.joa.2014.09.004. Epub 2014 Oct 30 [PubMed PMID: 26336552]
Arilla Iturri S, Artázcoz Artázcoz MA. [External temporary pacemakers]. Revista de enfermeria (Barcelona, Spain). 2008 Nov:31(11):54-7 [PubMed PMID: 19203121]
Ortiz Díaz-Miguel R, Gómez Grande ML. Temporary internal pacing. Medicina intensiva. 2014 Dec:38(9):575-9. doi: 10.1016/j.medin.2014.02.006. Epub 2014 Apr 29 [PubMed PMID: 24786750]