Introduction
Patellar instability, by definition, is a condition where the patella bone pathologically disarticulates out from the patellofemoral joint, either subluxation or complete dislocation. This most often involves multiple factors, from acute trauma, chronic ligamentous laxity, bony malalignment, connective tissue disorder, or anatomical pathology. Over time, patients with patellar instability can have debilitating pain, limitations in basic function, and long-term arthritis.[1][2][3][4]
Epidemiology
Patella dislocations account for 3% of all knee injuries.[5] The majority of injuries and pathology occurs in young individuals. In particular, most patients with patellar instability are aged 10 to 16 years old and female.[6][5] The incidence of patellar instability in the general population is 5.8 per 100,000 and 29 per 100,000 in the 10 to 17-year-old age group.[5][2] Many cases of first-time dislocations without loose bodies or articular damage are treated conservatively. However, the recurrence rate after conservative treatment can be up to 15 to 44%.[2] Patients with a history of two or more dislocations have a 50% chance of recurrent dislocation episodes.[5] A previous patellar dislocation is associated with the highest risk of persistent patellar instability later in life. Furthermore, in patients with a known medial patellofemoral ligament (MPFL) injury confirmed on MRI, the recurrence rates are even higher.[7] With these recurrence rates, first-time dislocators can continue to have pain, functional limitations, and instability.
Patellar instability can be summarized, and each entity will be discussed further below:
- Young patients (10 to 17 years old)
- Acute traumatic episode
- Chronic patholaxity - Ehlers-Danlos syndrome
- Bony malalignment - femoral anteversion, genu valgum, and external tibial torsion / pronated feet. The three bony malalignments combined are termed "Miserable Malalignment Syndrome" and lead to an increased Q angle.
- Anatomical pathology - trochlear dysplasia
- Eventual progression to pain, functional decline, and long-term arthritis
Classification
Patellofemoral instability is classified descriptively.[8][9] These classifications are listed below:
- Acute (first dislocation)
- Subluxation or dislocation
- Traumatic
- Patellar instability
- Recurrent
- Habitual dislocation - involuntary dislocation of the patella
- Passive patellar dislocation - with the aid of apprehension maneuver
- Syndromic - patellar dislocation associated with a neuromuscular disorder, connective tissue disorder, or syndrome
Mechanism
- Traumatic mechanisms can occur with a direct blow with a knee-to-knee collision or a helmet to the side of the knee injury
- Noncontact twisting injury with the knee extended and the foot externally rotated
Evaluation
- Presentation: [10] [1]
- Patient age and gender
- More likely in females
- More likely in younger age groups (10-17 years old)
- Record the number of previous dislocation or subluxation events
- Complaints of instability
- History of general ligamentous laxity
- Any previous surgery
- Pain location
- Anterior knee pain
- Patient age and gender
- Physical Examination: Examination will evaluate a number of areas.[10][1]
- Evaluate overall limb alignment
- Hip and knee rotation should be noted
- Excessive femoral anteversion will show the patient's toes pointed in or "pigeon toed"
- Presence of large hemarthrosis
- Evidence of an acute injury
- The absence of signs of trauma supports a chronic ligamentous laxity mechanism or a habitual mechanism
- Medial-sided tenderness over the medial patellofemoral ligament (MPFL)
- Increase in passive patellar translation compared to the contralateral side
- Midline is considered '0' quadrants of movement
- Normal is < 2 quadrants of patellar translation
- Lateral translation of the medial border of the patella to the lateral edge of the trochlea is '2' quadrants of motion and considered abnormal
- Apprehension sign - patella apprehension with passive lateral translation results in guarding and lack of a firm endpoint
- J sign - excessive lateral translation in extension, which then causes the patella to "pop" into the trochlear groove as the patella engages the trochlea early in flexion
- Assess the Q-angle
- The angle formed by a line from the ASIS to the center of the patella and from the center of the patella to the tibial tubercle
- The Q-angle in full extension can be falsely normal because the patella is not engaged in the trochlea and not on tension. Therefore it is recommended to assess the Q-angle in slight flexion, which is more reliable and accurate.
- Imaging: Radiographic examination will divulge several factors.[1]
- Radiographs will rule out loose bodies
- Most common is the medial patellar facet
- Lateral femoral condyle
- AP radiographs
- Best for evaluating overall lower extremity alignment
- Lateral radiographs
- Patellar height (Patella Alta versus Baja)
- Blumensaats line should extend to the inferior pole of the patella at 30 degrees of knee flexion
- Multiple ratios can be calculated and give an idea about the level of the patella. Ideally, the following ratio should be calculated with the knee in 30 degrees of flexion. Either on a lateral radiograph, Sagittal CT, or MRI images.
- Insall-Salvati ratio (0.8 - 1.2)
- It is the ratio of the patellar tendon length to the length of the patella (Figure 2)
- If the ratio is >1.2, this indicates Patella Alta
- Blackburn-Peel ratio (0.5-1)
- It is the ratio of the perpendicular distance between the tibial plateau and patellar articular surface to the length of the patella articular surface. (Figure 3) A ratio >1 indicates Patella Alta
- Caton-Deschamps - (0.6-1.3)
- It is the ratio of the distance between the most inferior point of the patella articular surface to the anterior angle of the tibial plateau and the length of the patellar articular surface. ( Figure 4). A ratio > 1.3 indicates Patella Alta
- The Caton-Deschamps and Blackburn-Peel measurements have higher reliability and can show change after a tibial tubercle osteotomy is performed
- Patellar tilt
- Trochlear dysplasia
- Crossing sign - seen on lateral radiograph, the trochlear groove lies in the same plane as the anterior border of the lateral femoral condyle
- Represents a flat trochlear groove
- Double contour sign - the anterior border of the lateral femoral condyle lies anterior to the anterior border of the medial femoral condyle
- Represents a convex trochlear groove/hypoplastic medial femoral condyle
- Supratrochlear spur
- Crossing sign - seen on lateral radiograph, the trochlear groove lies in the same plane as the anterior border of the lateral femoral condyle
- Patellar height (Patella Alta versus Baja)
- Sunrise/merchant views
- Best assessment for patellar tilt
- Lateral patellofemoral angle
- A line parallel to the lateral patellar facet and a line drawn across the posterior femoral condyles
- The normal angle is >11 degrees opening laterally
- Congruence angle is an index of subluxation
- Measured from a line through the apex of the patella to a line bisecting the trochlea
- If the congruence angle is lateral to the congruence line, it is considered positive
- If the congruence angle is medial to the congruence line, it is considered negative
- The normal angle is < (-)6 meaning the more positive the angle, the more subluxed the patella is laterally
- CT scan
- Evaluates femoral anteversion
- Evaluation of tibial rotation
- TT-TG distance (tibial tubercle to trochlear groove)
- Must be measured on axial images - it is calculated by taking a line on axial CT perpendicular to the posterior femoral condyles through the trochlear notch and a line through the middle of the tibial tubercle
- TT-TG distance is normally around 9 mm[11]
- TT-TG distance > 20mm is abnormal and has > 90% association with patellar instability[12]
- MRI
- Evaluation of loose bodies
- Osteochondral lesions
- The medial patellar facet is the most common
- Lateral femoral condyle bone bruising
- Most of the traumatic lesions occur during re-location impact
- Best for assessing MPFL[13]
- Location of injury
- The most common injury occurs at the femoral origin (Schottles point)
- Patellar attachment
- Midsubstance
- Combination
- Location of injury
- Evaluation of loose bodies
- Radiographs will rule out loose bodies
Treatment
- Nonoperative [10] [14][15]
- Closed reduction (majority spontaneously reduce on their own), NSAIDs, activity modification, and physical therapy
- Indications:
- First-time dislocation
- No loose bodies or articular damage
- No osteochondral fragments
- Habitual dislocators
- Patients with connective tissue disease - Ehlers Danlos
- Physical therapy should focus on closed chain exercises and quadriceps strengthening. Core hip strengthening and gluteal muscle strengthening will improve external rotators of the hip, thus externally rotating the femur and decreasing the Q-angle.
- Patella sleeve - 'J' sleeve
- Patellar taping
- Indications:
- Closed reduction (majority spontaneously reduce on their own), NSAIDs, activity modification, and physical therapy
- Operative [16]
- General indications for surgery:
- Arthroscopic debridement with removal of loose bodies[17]
- Indications:
- Loose bodies or osteochondral damage on imaging
- Open reduction internal fixation if there is sufficient bone available for fixation
- Screws and pins
- Indications:
- Medial patellofemoral ligament (MPFL) repair[18]
- Indications:
- Acute first-time dislocation with a bony fragment
- Direct repair with surgery can be performed within the first days after injury
- No study supports this method over nonoperative treatment
- Indications:
- MPFL reconstruction with autograft versus allograft[19]
- Indications:
- Recurrent instability and no malalignment or trochlear dysplasia
- Gracillis and semitendinosus commonly used
- Femoral origin can be reliably found (Schottles point)
- Schottle point is described as 1 mm anterior to the posterior cortex line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the posterior point of Blumensaats line
- Tensioning the graft should be done between 60 to 90 degrees of knee flexion is recommended
- Indications:
- Fulkerson-type osteotomy (anterior and medial tibial tubercle transfer)[20]
- Indications:
- Malalignment - Patellofemoral maltracking with degenerative changes on the distal and lateral aspects of the patella
- TT-TG > 20 mm
- Decreases pressure on the lateral patellar facet and overall trochlea
- Fulkerson showed poorer results with Outerbridge grade 3 or 4 lesions and lesions in the center of the trochlea or medial aspect of the trochlea
- Likely will fail when there are large central grade 3 or 4 lesions on the trochlea or medial, proximal, or diffuse patella arthritis
- Indications:
- Lateral soft tissue release[21]
- The lateral release has been shown to be ineffective for the treatment of patellar instability
- Used for lateral compression syndrome where there is combined or isolated patellar tilt or excessive tightness after medialization procedure
- Usually, this is combined with a medialization procedure and not done in isolation
- Trochleoplasty - sulcus deepening of the distal femoral trochlea[16]
- Limited use in the U.S. due to serious irreversible articular and subchondral injury to the trochlea
- Indicated for abnormal patellar tracking with J sign caused by femoral trochlear dysplasia
- Radiographic evidence of trochlear dysplasia
- The cancellous bone is exposed in the trochlea, and a strip of cortical bone on the edge of the trochlea is elevated. The new trochlea sulcus is created, and the trochlear bone shell is impacted and secured to the new sulcus fixed with staples or sutures.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The makeup of the patellofemoral joint is the undersurface of the patella and the cartilaginous anterior surface of the distal femur, comprising the trochlear groove. The proper biomechanics of the patellofemoral joint requires an intact and anatomic trochlear groove and inline congruent forces acting on the patella so that it can glide across the trochlear groove smoothly. Any disruption in this mechanism will produce dislocation of the patella out of the trochlear groove.
The bony structures of the patellofemoral joint do provide inherent stability to the patella, and any defect in the bony surface will result in instability. The majority of the patella articulation occurs between the lateral facet and the lateral trochlear groove. The normal trochlear groove has a large depth and steepness that provides inherent stability to the patellofemoral joint.[22] Trochlear dysplasia and flattening of this groove will cause patellar instability. The cartilage on the undersurface of the patella is 6 to 7 mm thick, the thickest in the body. The patella itself is a sesamoid bone enveloped in the quadriceps tendon. The major function of the patella is to increase the mechanical advantage of the muscle for knee extension.[11] The patella has seven facets. The major facets are medial and lateral, which are further divided into thirds. A seventh facet is on the most medial edge of the patella and is called the odd facet. Any osteochondral fracture or defect will lead to pain and instability and requires fixation.
Besides bony support, even more important to the stability of the patella is the soft tissue envelope. The quadriceps insert at the superior patella and encase the patella until it merges with the patellar tendon. The patellar tendon originates at the inferior aspect of the patella and inserts onto the tibial tubercle. The quadriceps tendon, patella, and patellar tendon combined make up the extensor mechanism of the knee. Disruption of the extensor mechanism along its length will result in significant patellar instability and maltracking.
The medial ligamentous constraints are just as important. The medial patellofemoral ligament (MPFL), patellomeniscal ligament, patellotibial ligament, and retinaculum of the knee capsule all play roles in preventing lateral patella motion and keeping the patella congruent in the trochlear groove. The strongest of these is the MPFL, which originates from the adductor tubercle to insert onto the superior medial border of the patella. The MPFL is the primary restraint to lateral patellar instability.[23] The major focus in treatment when performing an MPFL reconstruction is the location and ideal femoral position to restore normal anatomic knee biomechanics. The width of the femoral attachment of the MPFL is 11 to 20 mm between the medial epicondyle and adductor magnus insertion.[24][25][26]
Radiographically, Schottles point can be determined on fluoroscopy and is an accurate reproducible location for the femoral attachment. Schottles point is described as 1 mm anterior to the posterior cortex line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the posterior point of Blumensaats line.[27] (Figure 5). The MPFL contributes 50 to 60% of resistance to lateral translation of the patella.[28] Any laceration, avulsion, or traumatic disruption of MPFL will lead to lateral patellar instability. Once the patella begins to enter the trochlea at 20 to 30 degrees of flexion, the bony anatomy begins to be the major stabilizer as the patella sits in the trochlear groove. With patella alta, the patella does not engage in the groove until higher than normal knee flexion, and this predisposes the patella to dislocation.[29][1]
Lateral soft tissue restraints also can contribute to patellar instability but to a lesser degree. Studies have shown lateral structures to contribute to 22% of lateral translation and stability in lateral patellar dislocations.[1] These include the deep lateral transverse retinaculum, epicondylopatellar ligament, and patellotibial band. The epicondylopatellar ligament travels from the lateral femoral epicondyle and attaches directly to the tibia via the iliotibial band (ITB). Therefore, the tightness of the ITB influences lateral stability as well.
Dynamic stability is also a contributor to patellar stability. The vastus medialis muscle confers medial restraint to lateral translation. The vastus lateralis confers a lateral restraint to medial translation.
Knee alignment is a key factor in patellar stability. The normal alignment of the knee joint is at 6 degrees of valgus. The mechanical axis of the knee is a line drawn from the center of the hip to the center of the ankle. This should cross through the center of the knee. The anatomic axis of the knee is a line that goes through the center of the femoral and tibial shaft. In general, the anatomic axis of the femur is 6 degrees from the mechanical axis. Therefore, the knee angle (femorotibial angle) is approximately 6 degrees of valgus (in relation to the mechanical axis). An increased valgus at the knee off normal will force the patella out of the trochlear groove laterally and contribute to patellar instability.[30]
Normal femoral anteversion is 15 to 20 degrees. Femoral anteversion > 20 degrees increases the risk for patellar dislocation laterally because it produces a high laterally directed force across the patella.[31][32] It also increases the Q-angle leading to increased lateral force across the patella.
External tibial torsion also will contribute to lateral patellar instability. Normal tibial external rotation during childhood is 15 degrees.[33] The indications for tibial derotational osteotomy are poorly defined. Staheli recommends surgical correction for severe rotational deformities > 30 degrees. Typically external tibial torsion requires surgical correction with either a supramalleolar derotational osteotomy or a proximal tibial derotational osteotomy.[33][34]
The combination of increased femoral anteversion, increased genu valgus, and increased external tibia torsion is named "miserable malalignment syndrome." All these entities increase the Q-angle and subsequently increase the risk for patellar instability.[35][36]
Trochlear dysplasia is a disease characterized by a shallow trochlear groove. It is thought to be caused by either congenital factors or lateral patellar tracking. Lateral patellar tracking will eventually flatten the trochlear groove leading to patellar instability. Regardless of the cause, trochlear dysplasia results in a loss of the inherent bony stability of the patellofemoral joint.
Lastly, disorders that affect collagen include Ehlers-Danlos syndrome or Down Syndrome. These diseases cause a chronic progression of ligamentous laxity. When the soft tissue structures around the knee become lax, the patella loses its restraints, and these patients typically will complain of habitual dislocations. These patients will have a classic presentation of Ehlers-Danlos with hyperelastic skin, joint hypermobility, and generalized ligamentous laxity. The classic findings from Beighton are passive hyperextension of the digits >90 degrees, passive abduction of the thumb to the forearm, hyperextension of the knee, hyperextension of the elbows, and forward bending with palms on the floor.
Other anatomical factors:
- Patella alta - causes the patella to not articulate with the sulcus
- Excessive lateral patellar tilt caused by poor quadriceps flexibility and tight lateral structures
- Lateral femoral condyle hypoplasia
- Muscular
- Dysplasia of the vastus medialis oblique (VMO) muscle
- Overpull of ITB or vastus lateralis muscle[10]
Technique or Treatment
Reduction Technique
For simple lateral dislocations (most common), many dislocations will spontaneously reduce. A non-analgesic reduction attempt is encouraged. Calm and reassuring education can easily prepare the ideal patient. This education requires only a brief explanation of the presumed diagnosis, a description of the rapid reduction process, and the dramatic reduction in pain upon completion. The patient is placed in a supine, seated position. The patient should have their hips in slight flexion, helping to avoid contraction of the patellar tendon.[37][38][39]
For lateral dislocations, passively extend the knee into slight hyperextension while applying gentle medial pressure to the lateral edge of the patella. For a one-person reduction, maintain one supporting hand near the posterior ankle, giving weighted leverage to the patient’s leg. This technique seems to allow both better leverage and monitoring/sensing for resisting quadricep tension development which can make reduction more challenging. More challenging patients or patients with increased anxiety/pain may require a small analgesic to accomplish the same above method.
Post reduction views should include AP, lateral, and sunrise/merchant views to ensure successful reduction and assess for patellar avulsion or osteochondral injury of the lateral femoral condyle.
Complications
- Arthritis
- Arthrofibrosis
- Osteonecrosis
- Overconstraining the patella during MPFL reconstruction - tighten the MPFL at 60-90 degrees of flexion
- Excessive lateral release can cause medial instability or dislocation
- Recurvatum deformity after tibial tubercle procedures
- Recurrent dislocation
- Infection
Enhancing Healthcare Team Outcomes
Patellar dislocation is quite common and is best managed by an interprofessional team that may include a family clinician, physical therapist, and orthopedic nurses. Most simple cases of patella dislocation will spontaneously reduce, but recurrent cases should be referred to the orthopedic surgeon. The dislocation may often be associated with a knee pathology and lead to chronic pain, limitations in activity, and chronic arthritis. All interprofessional team members need to communicate with the rest of the interprofessional team regarding any changes in patient status and must keep meticulous and accurate patient records so that everyone on the case has access to the same updated patient data. This approach to these injuries will help achieve optimal patient outcomes. [Level 5]
Media
(Click Image to Enlarge)
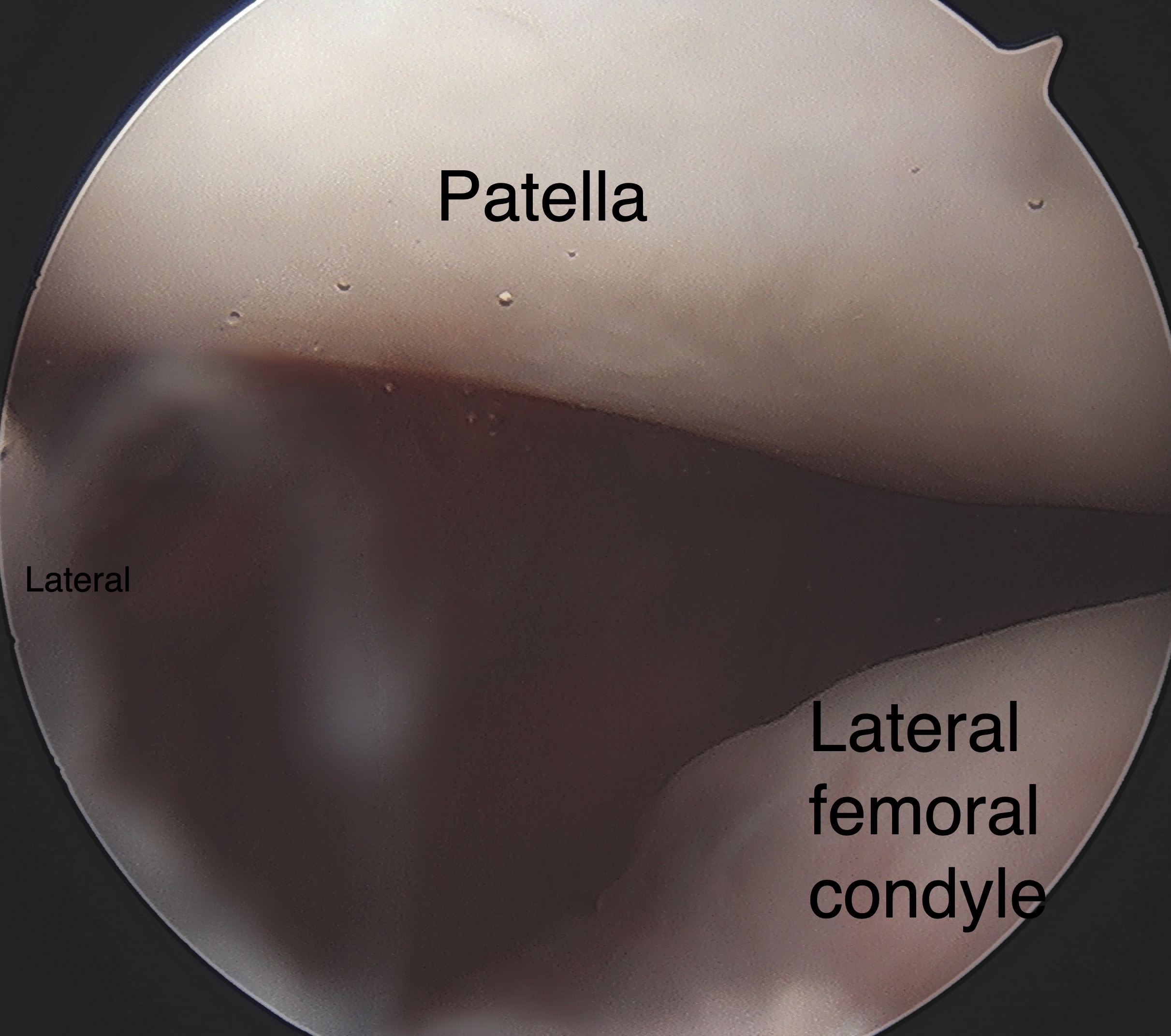
Right knee arthroscopic image demonstrating static lateral patellar subluxation during a diagnostic knee arthroscopy followed by medial patellofemoral ligament reconstruction using semitendinosus allograft tendon. Contributed by Matthew A Varacallo, MD
(Click Image to Enlarge)
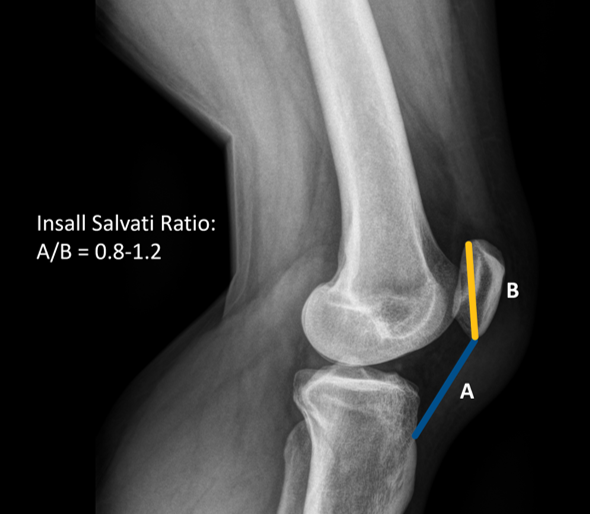
Insall Salvati Ratio Contributed by Ahmed Mabrouk
(Click Image to Enlarge)
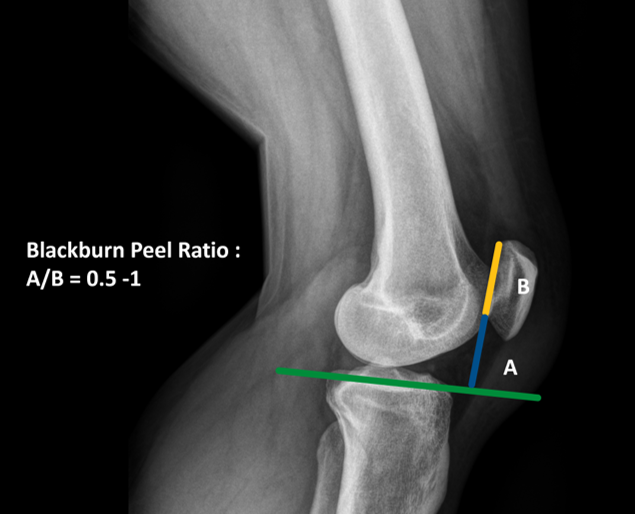
Blackburn Peel Ratio Contributed by Ahmed Mabrouk
(Click Image to Enlarge)
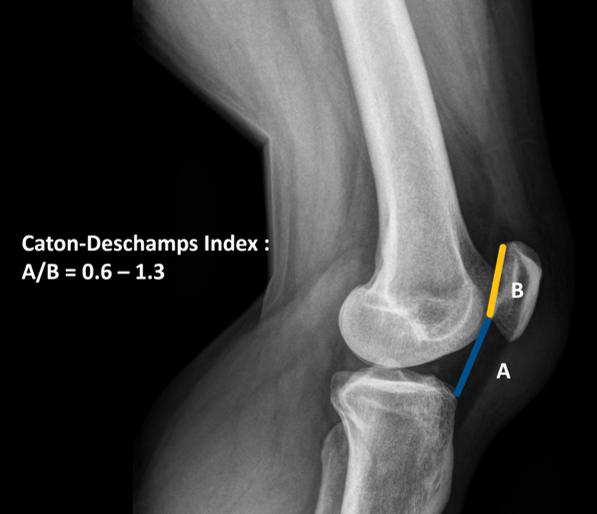
Caton-Deschamps Index Contributed by Ahmed Mabrouk
(Click Image to Enlarge)
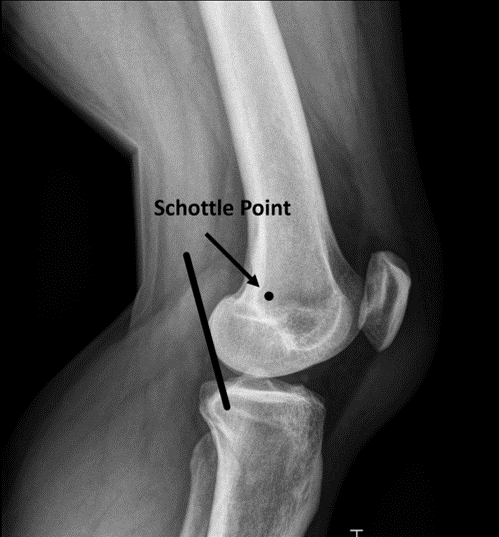
Schottle Point Contributed by Ahmed Mabrouk
References
Koh JL, Stewart C. Patellar instability. The Orthopedic clinics of North America. 2015 Jan:46(1):147-57. doi: 10.1016/j.ocl.2014.09.011. Epub [PubMed PMID: 25435044]
Hawkins RJ, Bell RH, Anisette G. Acute patellar dislocations. The natural history. The American journal of sports medicine. 1986 Mar-Apr:14(2):117-20 [PubMed PMID: 3717480]
Atkin DM, Fithian DC, Marangi KS, Stone ML, Dobson BE, Mendelsohn C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. The American journal of sports medicine. 2000 Jul-Aug:28(4):472-9 [PubMed PMID: 10921637]
Arnbjörnsson A, Egund N, Rydling O, Stockerup R, Ryd L. The natural history of recurrent dislocation of the patella. Long-term results of conservative and operative treatment. The Journal of bone and joint surgery. British volume. 1992 Jan:74(1):140-2 [PubMed PMID: 1732244]
Fithian DC, Paxton EW, Stone ML, Silva P, Davis DK, Elias DA, White LM. Epidemiology and natural history of acute patellar dislocation. The American journal of sports medicine. 2004 Jul-Aug:32(5):1114-21 [PubMed PMID: 15262631]
Hsiao M, Owens BD, Burks R, Sturdivant RX, Cameron KL. Incidence of acute traumatic patellar dislocation among active-duty United States military service members. The American journal of sports medicine. 2010 Oct:38(10):1997-2004. doi: 10.1177/0363546510371423. Epub 2010 Jul 8 [PubMed PMID: 20616375]
Level 2 (mid-level) evidenceSillanpää PJ, Peltola E, Mattila VM, Kiuru M, Visuri T, Pihlajamäki H. Femoral avulsion of the medial patellofemoral ligament after primary traumatic patellar dislocation predicts subsequent instability in men: a mean 7-year nonoperative follow-up study. The American journal of sports medicine. 2009 Aug:37(8):1513-21. doi: 10.1177/0363546509333010. Epub 2009 Apr 17 [PubMed PMID: 19376939]
Level 2 (mid-level) evidenceParikh SN, Lykissas MG. Classification of Lateral Patellar Instability in Children and Adolescents. The Orthopedic clinics of North America. 2016 Jan:47(1):145-52. doi: 10.1016/j.ocl.2015.08.016. Epub [PubMed PMID: 26614929]
Redler LH, Wright ML. Surgical Management of Patellofemoral Instability in the Skeletally Immature Patient. The Journal of the American Academy of Orthopaedic Surgeons. 2018 Oct 1:26(19):e405-e415. doi: 10.5435/JAAOS-D-17-00255. Epub [PubMed PMID: 30134308]
Colvin AC, West RV. Patellar instability. The Journal of bone and joint surgery. American volume. 2008 Dec:90(12):2751-62. doi: 10.2106/JBJS.H.00211. Epub [PubMed PMID: 19047722]
Rhee SJ, Pavlou G, Oakley J, Barlow D, Haddad F. Modern management of patellar instability. International orthopaedics. 2012 Dec:36(12):2447-56. doi: 10.1007/s00264-012-1669-4. Epub 2012 Oct 7 [PubMed PMID: 23052278]
Level 3 (low-level) evidenceDejour H, Walch G, Nove-Josserand L, Guier C. Factors of patellar instability: an anatomic radiographic study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 1994:2(1):19-26 [PubMed PMID: 7584171]
Putney SA, Smith CS, Neal KM. The location of medial patellofemoral ligament injury in adolescents and children. Journal of pediatric orthopedics. 2012 Apr-May:32(3):241-4. doi: 10.1097/BPO.0b013e3182471d72. Epub [PubMed PMID: 22411327]
Level 2 (mid-level) evidenceMäenpää H, Lehto MU. Patellar dislocation. The long-term results of nonoperative management in 100 patients. The American journal of sports medicine. 1997 Mar-Apr:25(2):213-7 [PubMed PMID: 9079176]
McConnell J. Rehabilitation and nonoperative treatment of patellar instability. Sports medicine and arthroscopy review. 2007 Jun:15(2):95-104 [PubMed PMID: 17505325]
He W, Yang YM, Liu M, Wang AY, Liu YJ. Reconstruction of the medial patellofemoral ligament using hamstring tendon graft with different methods: a biomechanical study. Chinese medical sciences journal = Chung-kuo i hsueh k'o hsueh tsa chih. 2013 Dec:28(4):201-5 [PubMed PMID: 24382220]
Donell ST, Joseph G, Hing CB, Marshall TJ. Modified Dejour trochleoplasty for severe dysplasia: operative technique and early clinical results. The Knee. 2006 Aug:13(4):266-73 [PubMed PMID: 16635572]
Schöttle PB, Fucentese SF, Pfirrmann C, Bereiter H, Romero J. Trochleaplasty for patellar instability due to trochlear dysplasia: A minimum 2-year clinical and radiological follow-up of 19 knees. Acta orthopaedica. 2005 Oct:76(5):693-8 [PubMed PMID: 16263617]
Fulkerson JP, Becker GJ, Meaney JA, Miranda M, Folcik MA. Anteromedial tibial tubercle transfer without bone graft. The American journal of sports medicine. 1990 Sep-Oct:18(5):490-6; discussion 496-7 [PubMed PMID: 2252090]
Level 3 (low-level) evidenceKuroda R, Kambic H, Valdevit A, Andrish JT. Articular cartilage contact pressure after tibial tuberosity transfer. A cadaveric study. The American journal of sports medicine. 2001 Jul-Aug:29(4):403-9 [PubMed PMID: 11476376]
Goyal D. Medial patellofemoral ligament reconstruction: the superficial quad technique. The American journal of sports medicine. 2013 May:41(5):1022-9. doi: 10.1177/0363546513477828. Epub 2013 Mar 4 [PubMed PMID: 23460327]
Amis AA, Oguz C, Bull AM, Senavongse W, Dejour D. The effect of trochleoplasty on patellar stability and kinematics: a biomechanical study in vitro. The Journal of bone and joint surgery. British volume. 2008 Jul:90(7):864-9. doi: 10.1302/0301-620X.90B7.20447. Epub [PubMed PMID: 18591593]
Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. The American journal of sports medicine. 1998 Jan-Feb:26(1):59-65 [PubMed PMID: 9474403]
Chahla J, Smigielski R, LaPrade RF, Fulkerson JP. An Updated Overview of the Anatomy and Function of the Proximal Medial Patellar Restraints (Medial Patellofemoral Ligament and the Medial Quadriceps Tendon Femoral Ligament). Sports medicine and arthroscopy review. 2019 Dec:27(4):136-142. doi: 10.1097/JSA.0000000000000252. Epub [PubMed PMID: 31688531]
Baldwin JL. The anatomy of the medial patellofemoral ligament. The American journal of sports medicine. 2009 Dec:37(12):2355-61. doi: 10.1177/0363546509339909. Epub 2009 Sep 2 [PubMed PMID: 19729366]
LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. The Journal of bone and joint surgery. American volume. 2007 Sep:89(9):2000-10 [PubMed PMID: 17768198]
Schöttle PB, Schmeling A, Rosenstiel N, Weiler A. Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. The American journal of sports medicine. 2007 May:35(5):801-4 [PubMed PMID: 17267773]
Amis AA, Firer P, Mountney J, Senavongse W, Thomas NP. Anatomy and biomechanics of the medial patellofemoral ligament. The Knee. 2003 Sep:10(3):215-20 [PubMed PMID: 12893142]
Geenen E, Molenaers G, Martens M. Patella alta in patellofemoral instability. Acta orthopaedica Belgica. 1989:55(3):387-93 [PubMed PMID: 2603680]
Level 2 (mid-level) evidenceWilson PL, Black SR, Ellis HB, Podeszwa DA. Distal Femoral Valgus and Recurrent Traumatic Patellar Instability: Is an Isolated Varus Producing Distal Femoral Osteotomy a Treatment Option? Journal of pediatric orthopedics. 2018 Mar:38(3):e162-e167. doi: 10.1097/BPO.0000000000001128. Epub [PubMed PMID: 29324527]
Lee TQ, Anzel SH, Bennett KA, Pang D, Kim WC. The influence of fixed rotational deformities of the femur on the patellofemoral contact pressures in human cadaver knees. Clinical orthopaedics and related research. 1994 May:(302):69-74 [PubMed PMID: 8168325]
Weber AE, Nathani A, Dines JS, Allen AA, Shubin-Stein BE, Arendt EA, Bedi A. An Algorithmic Approach to the Management of Recurrent Lateral Patellar Dislocation. The Journal of bone and joint surgery. American volume. 2016 Mar 2:98(5):417-27. doi: 10.2106/JBJS.O.00354. Epub [PubMed PMID: 26935465]
Staheli LT. Torsion--treatment indications. Clinical orthopaedics and related research. 1989 Oct:(247):61-6 [PubMed PMID: 2676305]
Rattey T, Hyndman J. Rotational osteotomies of the leg: tibia alone versus both tibia and fibula. Journal of pediatric orthopedics. 1994 Sep-Oct:14(5):615-8 [PubMed PMID: 7962504]
Hughston JC. Subluxation of the patella. The Journal of bone and joint surgery. American volume. 1968 Jul:50(5):1003-26 [PubMed PMID: 5676827]
Hughston JC. Patellar subluxation. A recent history. Clinics in sports medicine. 1989 Apr:8(2):153-62 [PubMed PMID: 2752433]
Level 2 (mid-level) evidenceVermeulen D, van der Valk MR, Kaas L. Plaster, splint, brace, tape or functional mobilization after first-time patellar dislocation: what's the evidence? EFORT open reviews. 2019 Mar:4(3):110-114. doi: 10.1302/2058-5241.4.180016. Epub 2019 Mar 27 [PubMed PMID: 30993012]
Purohit N, Hancock N, Saifuddin A. Surgical management of patellofemoral instability. I. Imaging considerations. Skeletal radiology. 2019 Jun:48(6):859-869. doi: 10.1007/s00256-018-3123-1. Epub 2018 Dec 12 [PubMed PMID: 30542758]
Arendt EA, Askenberger M, Agel J, Tompkins MA. Risk of Redislocation After Primary Patellar Dislocation: A Clinical Prediction Model Based on Magnetic Resonance Imaging Variables. The American journal of sports medicine. 2018 Dec:46(14):3385-3390. doi: 10.1177/0363546518803936. Epub 2018 Nov 6 [PubMed PMID: 30398902]