Introduction
Traumatic injuries can range from minor wounds to major, complex injuries causing shock and multi-system organ dysfunction. Trauma is the leading cause of death of patients between the ages of 15 and 24. It accounts for approximately 30% of all ICU admissions annually.[1] Pelvic trauma raises concern due to the high energy that is generally required to cause the injury. It is frequently associated with additional injuries, transfusions requirements, and prolonged rehabilitation.
The pelvis is a ring structure composed of bone. It consists of the sacrum, coccyx, and the innominate bones: the pubis, ischium, and ilium. The innominate bones join to form the acetabulum. The innominate bones join anteriorly at the pubic symphysis. It contains blood vessels, nerves, urogenital organs, and the rectum.
The pelvis is anatomically associated with a number of vascular structures. The aorta divides into the common iliac arteries at about the L4 level. The common iliac arteries then further divide into the internal and external branches at the sacroiliac joint. The superior gluteal artery is the most commonly injured vessel in pelvic trauma; it branches from the internal iliac artery and exits the pelvis at the sciatic notch. Other intrapelvic arteries that are associated with injuries include the inferior gluteal artery, rectal arteries, obturator artery, and the vesical artery. Veins accompany the arteries and are also prone to injury. The proximity of the veins and arteries accounts for the high incidence of combined injury. The seriousness of pelvic fractures comes from the association of other injuries, as well as the potential for hematoma and hemorrhagic shock.[2] Hemorrhage from pelvic fractures is a major cause of morbidity and mortality.
Nerve injuries are less common than vascular injuries with pelvic trauma. Lumbosacral plexus injuries account for the majority of nerve injuries after pelvic trauma. The plexus is in close proximity to the sacroiliac joint and the acetabulum, two of the more common pelvic injury locations. Root avulsion is possible and is typically only seen in more severe pelvic trauma. The lumbar plexus can be injured, though this is less common. Usually, injury occurs from traction or compression from a retroperitoneal bleed.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The pelvic ring is a very solid structure, requiring a great force to disrupt the complex. Therefore pelvic fractures are relatively uncommon. The majority of pelvic fractures result from motor vehicle collisions (MVCs), falls from height, or a pedestrian or cyclist struck by a vehicle.[4][5] There is, however, a high rate of associated injuries, occurring in 12% to 62% of patients with pelvic fractures.
Epidemiology
Pelvic fractures make up about 10% of fractures in blunt trauma patients. Over 16% of patients with pelvic fractures have at least one associated injury.[6] The most commonly injured structures are intraabdominal, with the liver, spleen, and kidneys occurring most often. Urogenital lesions account for over 40% of associated injuries. It is estimated that up to 24% of pelvic trauma patients have a urethral injury, and 20% have an associated bladder laceration. Most urethral injuries in males are located at the bulbomembranous junction.[7] One to two percent of traumatic rectal injuries are due to pelvic fractures.[8] Vaginal lacerations are reported in 2% to 4% of pelvic fractures. The American Association for the Surgery of Trauma (AAST) divides vaginal injuries into three degrees: I-III. First-degree includes contusion, hematoma, and superficial laceration involving only the mucosa. A second-degree laceration involves deep fat or muscle. Third-degree lacerations involve the cervix or peritoneum or injury into adjacent organs.[9]
Pelvic nerves and vascular lesions are also relatively common.[10] The most commonly injured arteries are anterior branches of the internal iliac artery: superior gluteal artery, lateral sacral artery, and the pedestal and obturator arteries. The most common veins injured are the presacral plexus and the prevesical veins.[11] Blood loss can also come from the fractured bones.[12]
Pathophysiology
Disruption of the pelvic ring causes an increase in the internal volume of the pelvis. The increased volume will decrease the tamponade effect of the retroperitoneal space, allowing increased blood loss.[4][13]
There are two main classification systems of pelvic fractures: the Tile and the Young-Burgess classification systems. Tile et al. described three types of underlying mechanisms for pelvic fractures. Type A is a rotationally and vertically stable fracture. Type B is rotationally unstable but vertically stable. Finally, type C is both rotationally and vertically unstable.[4] The Young-Burgess classification consists of anteroposterior compression (APC), lateral compression (LC), vertical shear (VS), or a combined mechanism (CM). Anteroposterior compression fractures are often unstable; these are the “open book” pelvic fractures. They are associated with pelvic and retroperitoneal hemorrhage. They typically occur from a head-on MVC. Lateral compression is the most common. These fractures are often stable but can be associated with a bladder rupture. These commonly result from a T-bone MVC or a pedestrian hit from the side. A vertical shear injury is usually unstable. They require a substantial force on one or both hemipelves, such as a jump from a tall height or being hit by a falling tree. They cause complete ligamentous injury.[14][15]
The Young-Burgess and Tile classification both classify pelvic fractures on the anatomic classification of injuries but fail to consider hemodynamic stability. The World Society of Emergency Surgery (WSES) created a classification that is based on anatomic classification as well as the hemodynamic stability of the patient; this helps with consideration of a treatment algorithm. The WSES classification divides pelvic injuries into three categories: mild, moderate, and severe.
- Minor: WSES grade I; the fracture is stable, and the patient is hemodynamically stable
- Grade I: APC I and LC I fractures
- Moderate: WSES grade II and grade III; the fracture is unstable, but the patient is hemodynamically stable
- Grade II: APC II, APC III, and LC II, LC III fractures
- Grade III: VS and CM fractures
- Severe: WSES grade IV: the fracture is either stable or unstable, but the patient is hemodynamically unstable.
- Grade IV: any fracture pattern in a hemodynamically unstable patient
Minor injuries are typically treated with nonoperative management. Moderate injuries are given a pelvic binder in the field, and then should be considered for angioembolization if a blush is seen on CT scan. Severe injuries require more intense intervention. A pelvic binder should be placed in the field. Upon arrival, the patient should be treated with preperitoneal packing, resuscitative endovascular balloon occlusion of the aorta (REBOA), or angioembolization.[4] These treatment options will be discussed in more detail below.
History and Physical
The initial approach to any trauma patient is described in the Advanced Trauma Life Support (ATLS) course; it is a structured and standardized approach. The approach is meant to recognize and stabilize life-threatening injuries first. It is important to note an initial detailed history is not essential to begin evaluating a patient with acute injuries. The emergency medical system (EMS) personnel bringing the patient to the trauma/resuscitation area of the emergency department (ED) will provide a brief history of present illness. After the initial evaluation and stabilization of the patient, a detailed history can be obtained. A few useful facts include the mechanism of injury, whether the patient was ambulatory at the scene, bowel or bladder incontinence, and any numbness or weakness. In an awake trauma patient, the history and physical exam are highly sensitive for pelvic trauma.[16]
Evaluation
The initial evaluation of the trauma patient is the primary survey. The mnemonic ABCDE is a helpful way to remember the order of the evaluation.
- A: Airway and cervical spine protection. An easy way to assess the airway is to have the patient speak. Ask them their name.
- B: Breathing. Listen for bilateral breath sounds and look at the chest wall motion during the respiratory cycle
- C: Circulation. This helps determine whether the patient is in shock.
- D: Disability. This is the Glasgow coma scale (GCS)
- E: Exposure and environmental control. Here the examiner undresses the patient the provide head-to-toe evaluation for injury.
The secondary survey follows the primary survey.[17] This is a head-to-toe complete exam. A digital rectal exam should also be performed during the secondary survey. Gross blood indicates a gastrointestinal injury. A high riding prostate, blood at the urethral meatus, an inability to void, or gross hematuria could be another indication of a urethral injury.[4][18] The pelvis is assessed with anteroposterior compression. Perineal hematoma and edema should also raise suspicion for pelvic content injuries. Any instability indicates a pelvic fracture. Any compressive force causing movement of the pelvis can disrupt any hemostasis that has occurred, so this force is generally limited to a single attempt.[17][19]
Laboratory markers are often useful in traumatic settings. Sensitive markers for hemorrhage include serum lactate level and a base deficit, which can both be obtained from an arterial blood gas. Serum lactate and base deficit can also be used to monitor resuscitation. It is important to remember hemoglobin or hematocrit levels are not sensitive for identifying acute traumatic hemorrhage.[4][5] Other useful laboratory markers are coagulation panels, such as PTT, PT/INR, and fibrinogen levels. Patients that have undergone a traumatic injury are susceptible to coagulopathy, increasing their mortality risk.[4] Thromboelastography (TEG) or rotational thromboelastometry (ROTEM) are useful tools to allow targeted resuscitation with blood products.[20]
Multiple imaging modalities can be useful in evaluating pelvic trauma. An ultrasound can be used to perform a Focused Assessment with Sonography in Trauma (FAST) exam while in the trauma/resuscitation area. A FAST exam is used to identify free fluid. It cannot differentiate bowel contents from blood.[21] Pelvic x-rays in a hemodynamically unstable patient may help identify potentially life-threatening causes of injury. If the patient is unstable, a quick x-ray can direct care. It is still important to remember there are likely additional injuries, so a pelvic fracture may not be the sole cause of instability. A pelvic x-ray is also useful to evaluate for hip pathology, such as a fracture or dislocation that needs quick reduction.[22]
X-ray, while useful for quick evaluation in an unstable patient, is still inferior to computed tomography (CT) for the evaluation of fractures.[22] CT scanning remains the gold standard. A CT scan not only identifies fractures but has the ability for three-dimensional bone reconstruction. 3-D reconstruction allows better operative planning for patients.[4] The ability to add contrast increases the ability to find injuries. A triple-phase contrast-enhanced CT consists of an arterial phase, a portal phase, and a delayed phase.[4][23] A blush on the arterial phase indicates active arterial bleedings; it can be seen as a hyperdensity within a hematoma. A delayed phase will show injuries to urologic structures. CT scan also has the benefit of adding rectal contrast in cases where a rectal injury is suspected.
A urethrogram can help diagnose a urethral injury. As urethral injuries alone are not life-threatening, any vascular or visceral injury should be managed prior to undergoing urethrogram. In the trauma setting, a urethrogram should be performed in a fluoroscopic suite by a trained radiologist. In an ascending study, a 6-8 French Foley catheter is inserted into the fossa navicularis, which is just beyond the meatus. The foley balloon is filled with 2 to 3 mL of water. A C-arm is brought over the bed and is rotated to either the left or right 30 degrees to an anterior oblique position. The patient then elevates his left side to the same degree. 30 mL of iodinated contrast is slowly injected into the foley catheter until the contrast is visualized within the bladder. A descending study fills the bladder with 400 mL of contrast. The patient is then asked to micturate into a bottle in a standing oblique position. An injury is visualized as contrast extravasation. A complete urethral transection typically requires both an ascending and descending urethrogram to estimate the length of transection.[18][24][25]
Treatment / Management
Pelvic fractures, no matter the grade, have the potential to become life-threatening. Treatment for pelvic fractures starts with the ABCs (airway, breathing, and circulation) during the primary survey. Adequate resuscitation is crucial in any trauma patient. Two large-bore IVs should be placed in all patients arriving at the trauma bay. Hypotension should be addressed with aggressive fluid resuscitation, followed by blood products if the patient remains hypotensive.
Pelvic binders should be placed when there are signs of pelvic ring disruption in either stable or unstable patients. The binder acts in two ways to decrease bleeding. It compresses the bleeding from the bones, but they also decrease the volume within the pelvis. By decreasing the volume, it promotes a tamponade effect. Pelvic binders are a temporary measure until a more definitive repair can occur. The pelvic binder is only useful if it is applied correctly; The binder must be placed around the greater trochanter and pubic symphysis to adduct the legs and decrease pelvic volume correctly.[4][26] A pelvic binder should not be placed in a lateral fracture, as this can increase bleeding.[27](B2)
Hemodynamically Stable Pelvic Fractures
Evidence of arterial bleed on CT should go directly for angioembolization. Pelvic angiography is usually performed by interventional radiology (IR). Angioembolization is successful in 85% to 100% of cases.[28] Angioembolization is usually performed via a femoral artery approach. If the femoral is unavailable, the left brachial or axillary artery may be used. In the best circumstances, a single bleeding vessel is visualized and embolized. In some circumstances, there are multiple bleeding vessels, or the single bleeding vessel cannot be accessed. In this situation, a nonselective, or “shotgun” approach can be performed. This is possible due to the vast collateral network within the pelvis. The most common vessels for embolization are the internal iliac artery and its branches: the superior gluteal artery, the obturator artery, and the internal pudendal artery. Absorbable gelatin compressed sponge and coils are typically used for embolization. Absorbable gelatin compressed sponge is a temporary agent that is inexpensive and readily available. Coils are permanent. Coils only work if the coagulation pathway is intact, as they induce a thrombotic effect leading to clot formation and occlusion.[29] After embolization, a completion angiogram is used to confirm the bleeding has stopped.[30][27] Studies have shown angioembolization within 90 minutes of arrival to the hospital had improved survival rates.[31] Angioembolization can be repeated in patients with continued hemorrhage and hemodynamic instability after first embolization. (A1)
Patients with hemodynamic stable pelvic fractures should be admitted to the hospital for observation.
Hemodynamically Unstable Pelvic Fractures
Generally, patients will go for immediate laparotomy if they remain unstable with concern for injury. However, many authors argue angioembolization should be done prior to going to the operating room (OR). The basis of the argument is there is a high likelihood of finding an arterial bleeding source, and because there is a strong correlation between time to embolization and survival as stated above.
Preperitoneal packing (PPP) involves putting packing up against the peritoneum to create a tamponade effect. It is less time consuming than angioembolization. Preperitoneal packing is useful for hemodynamically unstable patients at centers without IR. It can also be used as a bridge to more time-consuming procedures, such as angioembolization, at level 1 trauma centers. Another important use is in patients that are hemodynamically unstable and require other life-saving surgical intervention. Packing is performed through a vertical midline incision of 6 to 8 cm or Pfannenstiel incision. Dissection continues down to fascia; fascia is then incised in the midline to access the preperitoneal space. Ringed forceps are then used to put three surgical pads into the space, with the first being pushed all the way to the sacrum. The same is performed on the contralateral side. Six surgical pads are typically enough to complete the packing. The fascia is then quickly closed over the surgical pads, and the skin is closed in a running fashion.[32]
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is an alternative to cross-clamping the aorta. REBOA has emerged in recent years at trauma centers around the world. It uses a balloon catheter to occlude the aorta in an attempt to minimize life-threatening hemorrhage. It has been speculated that REBOA can be useful in pelvic trauma. Literature has shown zone III (infra-renal) occlusion is useful in pelvic trauma as it has little visceral organ insult.[4][33] The common femoral artery is typically used for access. If there is a suspected femoral or iliac injury, one side of the contralateral side should be accessed. An 18G needle is used to access the artery. A guidewire is introduced into the needle and advanced into the vascular system. The needle is removed, and the tract is dilated until a 7 Fr sheath can be inserted into the vessel. The catheter position is measured by measuring the distance from the umbilicus to the femoral catheter insertion site and is then inflated until moderate resistance is felt or there is a loss in the contralateral pulse, typically 15 to 20 mL in the balloon for zone III deployments. The patient should then be expedited to either IR or the OR for definitive treatment. REBOA inflation time is ideally less than 30 minutes but can be used for up to 60 minutes. Upon deflating REBOA, hemodynamic changes can be noted. The balloon can be intermittently reinflated to allow resuscitation and reduce reperfusion injury. The femoral artery access site may require surgical repair.[34] If a common femoral access site is not available, then the left brachial or left common carotid artery may be used.[35][36][37](A1)
Unstable pelvic fractures require surgical fixation. Early fixation has been shown to improve pain, improved fracture reduction, earlier mobilization, and control of bleeding from fractured bones.[4][38] There are a few surgical options available. External fixation allows initial stabilization in hemodynamically unstable patients and those with pelvic contamination. It is generally placed within the operating room. The common pin locations are the iliac wings and the anterior inferior iliac spine. The iliac wing is accessed by making an incision about 2 cm posterior to the anterior superior iliac spine down to the bone. The gluteal ridge is the target insertion spot due to its strength. The pin is inserted manually.[39] Anterior inferior iliac spine pins have greater pullout strength and provide better access for reduction. These two options only provide anterior pelvis fixation. For VS injuries, posterior stabilization is required with skeletal traction.[40][41] Generally, iliac wing fracture or acetabular fracture are contraindications to external fixation.
Definitive repair, if needed, is undertaken once the patient has been adequately resuscitated and stabilized. Patients that are hemodynamically stable or “borderline” can be safely taken for definitive repair within 24 hours of injury. Physiologically deranged polytrauma patients should not be taken for definitive repair until they are stable. Studies show post-injury complication rates are increased if definitive repair is completed within four days of injury in polytrauma patients. Complications decreased when surgery was delayed until six to eight days post-injury. [42] Therefore, it is recommended to wait at least four days to proceed with any definitive treatment of pelvic fractures. Posterior ring injury reconstructions are most important for functional outcomes. APC I and LC I are managed nonoperatively. APC II is typically managed with anterior symphyseal plating. APC III is treated with either anterior symphyseal multihole plating or external fixation with posterior stabilization with sacroiliac screws. LC II is treated with ORIF of the ilium. LC III and VS require posterior stabilization with sacroiliac screws. It can be done open or percutaneous based.[43][44][45] Open reduction and internal fixation provides a better repair and allows earlier mobilization. Percutaneous fixation of the posterior ring can be useful in patients with traumatic posterior skin injuries.[38](B2)
Associated bladder injuries may require repair. The location of the injury dictates the management. Generally, extraperitoneal bladder injuries are treated nonoperatively; intraperitoneal bladder injuries require surgical repair. A foley catheter remains in place for about 14 days. A repeat cystogram should be performed prior to catheter removal.[46] Urethral injuries are possible with pelvic fractures. Complete transection of the urethra should be treated with a suprapubic catheter and delayed repair; partial transection is manageable with a foley catheter. [25] Any associated perineal injury should be closely monitored for vesicocutaneous or urethrocutaneous fistula formation.[47](B2)
Sigmoid and intraperitoneal rectal injuries should be debrided and primarily repaired when able. An injury comprising less than 50% circumference is eligible for primary repair. This has been shown to reduce complications. For injuries that cannot be primarily repaired, resection with primary anastomosis is usually performed with or without fecal diversion.[48] For injuries that are greater than 50%, the colon or rectum should be debrided to healthy tissue. Then a primary anastomosis or diversion can be performed. Extraperitoneal rectal injuries are treated with primary repair with a diverting colostomy.[49] Recent studies have shown no use for presacral drainage or distal washout for extraperitoneal rectal injuries.[50](B2)
Vaginal laceration treatment is dependent on the degree. First-degree injuries generally only require gauze packing. Second and third-degree injuries require surgical repair, typically by a gynecologist.[9](B2)
Differential Diagnosis
- Acetabular pelvic fracture
- Bladder injury
- Hip fracture
- Hip dislocation
- Urethral transection
- Open book pelvic fracture
- Rectal injury
- Sigmoid injury
- Urethral transection
- Vertical shear pelvic fracture
Prognosis
Unstable pelvic fractures have a mortality of about 8%. Patients that are in hemorrhagic shock at presentation have increased mortality. Patients that present with an open pelvic fracture have a mortality risk of up to 45%. As noted earlier, the seriousness of pelvic fractures stems from the associated injuries; the risk of death from isolated pelvic fracture ranges from 0.4% to 0.8%.[12][51][52]
Complications
The associated injuries with pelvic fractures make prognostic measurements difficult. One study showed that over 60% of patients with traumatic pelvic fractures experience chronic pelvic pain. Chronic pain is associated with depression and anxiety. External fixation is associated with pin site infections that can be treated with PO or IV antibiotics +/- debridement of site. Lateral femoral cutaneous nerve injury can also occur from external fixation.[53]
Urogenital injuries can be associated with sexual dysfunction, such as dyspareunia, erectile dysfunction, and restricted motion. Urinary and fecal incontinence are also possible. Urethral strictures have been reported in 31% to 69% of complete urethral transections.[18] Urethral strictures can be treated conservatively with dilation. However, if dilation fails repair with posterior urethroplasty, also called bulbomembranous anastomosis (BMA), may be required. BMA success rates are over 90%.[25]
Urinary incontinence is initially treated conservatively. Pelvic floor strengthening and biofeedback are used initially. Duloxetine, a selective serotonin/norepinephrine reuptake inhibitor is used in combination with physiotherapy successfully in many patients.[54] A sacral nerve stimulator can be implanted within the upper buttock and has been used to treat incontinence successfully.[55] Urinary incontinence can be treated with artificial urinary sphincter implantation when other methods fail.[7]
Similarly, fecal incontinence starts with nonoperative management. Dietary changes and fiber supplements can optimize stool consistency and limit urgency. Medications can be used to slow the bowels. Examples include the antidiarrheals Imodium and Lomotil, the bile acid binder cholestyramine, and medications the reduce the reflexive relaxation of the sphincter, such as amitriptyline. Physical therapy and biofeedback have been used successfully to strengthen the pelvic floor. If conservative treatments fail, a sphincteroplasty can be performed. Other options include implanting artificial anal sphincters or magnetic anal sphincters. Sacral nerve stimulators can also be successful.[56]
It is important to note a pelvic binder itself can cause complications. A pelvic binder should not be placed for more than 24 hours. The binder can cause skin necrosis and pressure ulcers as soon as 2 to 3 hours after placement.[4] There is a high risk of deep venous thrombosis with all trauma patients; this risk is compounded by decreased mobility and bone fractures. Patients should be treated with mechanical serial compression devices and chemoprophylaxis until they are ambulatory.
Complications from angioembolization occur in up to 5% of cases. Complications can occur at the access site and include hematoma, pseudoaneurysm, dissection, or thrombus. Pelvic tissue necrosis can be a life-threatening complication and requires exploration and repair. Patients can have a reaction to the contrast itself or develop contrast nephropathy and an acute kidney injury.
Potential REBOA complications are numerous and mainly involve vessel injuries. The balloon can cause an arterial rupture, perforation, or dissection. The catheter itself can create lower extremity ischemia and subsequent reperfusion injury and compartment syndrome. Balloon occlusion also leads to distal ischemia. Prolonged occlusion leads to organ ischemia, which can be irreversible. Organ reperfusion can lead to multiorgan dysfunction or failure, including acute kidney injury, liver failure, intestinal ischemia, spinal cord infarction, and death. Access site complications can be treated with patch repairs, arterial reconstructions with native or artificial tissue, or bypasses. If these measures fail, then the limb would require amputation. Aortic injuries from REBOA are generally life or limb-threatening. Multiorgan dysfunction is generally treated medically.[35][36]
Deterrence and Patient Education
Cell phone use while driving causes an estimated 1.6 million car crashes annually. About 1 in 4 crashes are related to texting while driving. Drivers should always obey the speed limit, avoid driving under the influence, and should not be distracted while driving. Pedestrians should always be aware of the traffic around them. It should not be assumed a car will see them or give the pedestrian the right of way.
It is important to set patients’ expectations. The patient will need extended rehabilitation and physical therapy from a complex pelvic fracture. They should be educated on the possibility of chronic pain and should receive information on pain management options, as well as options for the possible depression and anxiety that may follow. Patients with colostomies from colonic injuries should receive ostomy training. The possibility of sexual dysfunction should be addressed with appropriate referrals to OB/GYN or urology.
Pearls and Other Issues
- Pelvic injuries are associated with high mortality, associated internal injuries, and significant bleeding.
- A plain pelvic x-ray is quick; however, a CT scan is the gold standard for fractures. A scan ideally should be performed with IV contrast with an arterial phase, a portal phase, and a delayed phase.
- Obtain consults to orthopedics and urology, if needed, early for optimal care and timely management of the patient.
- Early involvement of physical and occupational therapy are crucial for recovery.
- It is essential to counsel patients on potential complications and to set recovery expectations.
Enhancing Healthcare Team Outcomes
Managing traumatic pelvic fractures requires an interprofessional team approach. The emergency medicine and trauma surgery teams should recognize the risk factors for pelvic fractures and involve the orthopedic teams early when fractures are identified. Potential complications should be common knowledge for the teams involved, allowing for early detection. Physical and occupational therapy should be involved early. Pelvic trauma patients truly do require an interprofessional team to achieve the best results.
Media
(Click Image to Enlarge)

Pelvic Radiograph, Left Hip Fracture
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)

Pelvic Radiograph, Right Hip Fracture
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)
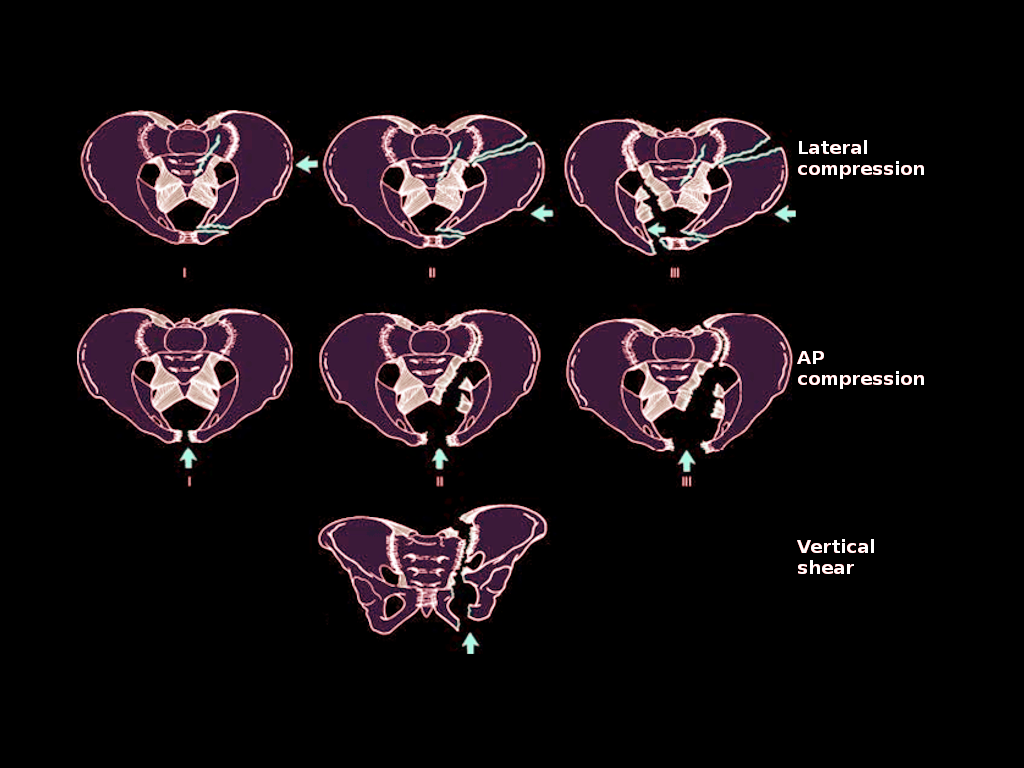
Pelvic Ring Injuries. Pelvic ring injuries depicting lateral compression, AP compression, and vertical shear.
Contributed by O Chaigasame, MD
References
Mackenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, Salkever DS, Weir S, Scharfstein DO. The National Study on Costs and Outcomes of Trauma. The Journal of trauma. 2007 Dec:63(6 Suppl):S54-67; discussion S81-6 [PubMed PMID: 18091213]
Wijffels DJ, Verbeek DO, Ponsen KJ, Carel Goslings J, van Delden OM. Imaging and Endovascular Treatment of Bleeding Pelvic Fractures: Review Article. Cardiovascular and interventional radiology. 2019 Jan:42(1):10-18. doi: 10.1007/s00270-018-2071-4. Epub 2018 Sep 17 [PubMed PMID: 30225676]
Chiodo A. Neurologic injury associated with pelvic trauma: radiology and electrodiagnosis evaluation and their relationships to pain and gait outcome. Archives of physical medicine and rehabilitation. 2007 Sep:88(9):1171-6 [PubMed PMID: 17826464]
Level 2 (mid-level) evidenceCoccolini F, Stahel PF, Montori G, Biffl W, Horer TM, Catena F, Kluger Y, Moore EE, Peitzman AB, Ivatury R, Coimbra R, Fraga GP, Pereira B, Rizoli S, Kirkpatrick A, Leppaniemi A, Manfredi R, Magnone S, Chiara O, Solaini L, Ceresoli M, Allievi N, Arvieux C, Velmahos G, Balogh Z, Naidoo N, Weber D, Abu-Zidan F, Sartelli M, Ansaloni L. Pelvic trauma: WSES classification and guidelines. World journal of emergency surgery : WJES. 2017:12():5. doi: 10.1186/s13017-017-0117-6. Epub 2017 Jan 18 [PubMed PMID: 28115984]
Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J, Fernández-Mondéjar E, Hunt BJ, Komadina R, Nardi G, Neugebauer E, Ozier Y, Riddez L, Schultz A, Stahel PF, Vincent JL, Spahn DR, Task Force for Advanced Bleeding Care in Trauma. Management of bleeding following major trauma: an updated European guideline. Critical care (London, England). 2010:14(2):R52. doi: 10.1186/cc8943. Epub 2010 Apr 6 [PubMed PMID: 20370902]
Demetriades D, Karaiskakis M, Toutouzas K, Alo K, Velmahos G, Chan L. Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. Journal of the American College of Surgeons. 2002 Jul:195(1):1-10 [PubMed PMID: 12113532]
Zhang F,Liao L, Artificial urinary sphincter implantation: an important component of complex surgery for urinary tract reconstruction in patients with refractory urinary incontinence. BMC urology. 2018 Jan 8 [PubMed PMID: 29310634]
Giannoudis PV, Grotz MR, Tzioupis C, Dinopoulos H, Wells GE, Bouamra O, Lecky F. Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. The Journal of trauma. 2007 Oct:63(4):875-83 [PubMed PMID: 18090020]
Level 3 (low-level) evidenceLi P, Zhou D, Fu B, Song W, Dong J. Management and outcome of pelvic fracture associated with vaginal injuries: a retrospective study of 25 cases. BMC musculoskeletal disorders. 2019 Oct 22:20(1):466. doi: 10.1186/s12891-019-2839-y. Epub 2019 Oct 22 [PubMed PMID: 31640643]
Level 2 (mid-level) evidenceSiegmeth A, Müllner T, Kukla C, Vécsei V. [Associated injuries in severe pelvic trauma]. Der Unfallchirurg. 2000 Jul:103(7):572-81 [PubMed PMID: 10969545]
Pereira SJ,O'Brien DP,Luchette FA,Choe KA,Lim E,Davis K Jr,Hurst JM,Johannigman JA,Frame SB, Dynamic helical computed tomography scan accurately detects hemorrhage in patients with pelvic fracture. Surgery. 2000 Oct; [PubMed PMID: 11015102]
Level 2 (mid-level) evidenceGrotz MR, Allami MK, Harwood P, Pape HC, Krettek C, Giannoudis PV. Open pelvic fractures: epidemiology, current concepts of management and outcome. Injury. 2005 Jan:36(1):1-13 [PubMed PMID: 15589906]
Blackmore CC, Cummings P, Jurkovich GJ, Linnau KF, Hoffer EK, Rivara FP. Predicting major hemorrhage in patients with pelvic fracture. The Journal of trauma. 2006 Aug:61(2):346-52 [PubMed PMID: 16917449]
Level 2 (mid-level) evidenceAlton TB, Gee AO. Classifications in brief: young and burgess classification of pelvic ring injuries. Clinical orthopaedics and related research. 2014 Aug:472(8):2338-42. doi: 10.1007/s11999-014-3693-8. Epub 2014 May 28 [PubMed PMID: 24867452]
Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: value of plain radiography in early assessment and management. Radiology. 1986 Aug:160(2):445-51 [PubMed PMID: 3726125]
Shlamovitz GZ, Mower WR, Bergman J, Chuang KR, Crisp J, Hardy D, Sargent M, Shroff SD, Snyder E, Morgan MT. How (un)useful is the pelvic ring stability examination in diagnosing mechanically unstable pelvic fractures in blunt trauma patients? The Journal of trauma. 2009 Mar:66(3):815-20. doi: 10.1097/TA.0b013e31817c96e1. Epub [PubMed PMID: 19276759]
Level 2 (mid-level) evidenceCoughenour J. Initial Evaluation and Management of the Injured Patient. Missouri medicine. 2018 Sep-Oct:115(5):429-433 [PubMed PMID: 30385990]
Ingram MD, Watson SG, Skippage PL, Patel U. Urethral injuries after pelvic trauma: evaluation with urethrography. Radiographics : a review publication of the Radiological Society of North America, Inc. 2008 Oct:28(6):1631-43. doi: 10.1148/rg.286085501. Epub [PubMed PMID: 18936026]
Geeraerts T, Chhor V, Cheisson G, Martin L, Bessoud B, Ozanne A, Duranteau J. Clinical review: initial management of blunt pelvic trauma patients with haemodynamic instability. Critical care (London, England). 2007:11(1):204 [PubMed PMID: 17300738]
Gonzalez E, Moore EE, Moore HB. Management of Trauma-Induced Coagulopathy with Thrombelastography. Critical care clinics. 2017 Jan:33(1):119-134. doi: 10.1016/j.ccc.2016.09.002. Epub [PubMed PMID: 27894492]
Friese RS, Malekzadeh S, Shafi S, Gentilello LM, Starr A. Abdominal ultrasound is an unreliable modality for the detection of hemoperitoneum in patients with pelvic fracture. The Journal of trauma. 2007 Jul:63(1):97-102 [PubMed PMID: 17622875]
Level 2 (mid-level) evidenceGuillamondegui OD, Pryor JP, Gracias VH, Gupta R, Reilly PM, Schwab CW. Pelvic radiography in blunt trauma resuscitation: a diminishing role. The Journal of trauma. 2002 Dec:53(6):1043-7 [PubMed PMID: 12478025]
Level 2 (mid-level) evidenceVerbeek DO, Burgess AR. Importance of Pelvic Radiography for Initial Trauma Assessment: An Orthopedic Perspective. The Journal of emergency medicine. 2016 Jun:50(6):852-8. doi: 10.1016/j.jemermed.2015.03.048. Epub 2016 Apr 25 [PubMed PMID: 27133737]
Level 3 (low-level) evidenceBarratt RC, Bernard J, Mundy AR, Greenwell TJ. Pelvic fracture urethral injury in males-mechanisms of injury, management options and outcomes. Translational andrology and urology. 2018 Mar:7(Suppl 1):S29-S62. doi: 10.21037/tau.2017.12.35. Epub [PubMed PMID: 29644168]
Dixon AN, Webb JC, Wenzel JL, Wolf JS Jr, Osterberg EC. Current management of pelvic fracture urethral injuries: to realign or not? Translational andrology and urology. 2018 Aug:7(4):593-602. doi: 10.21037/tau.2018.01.14. Epub [PubMed PMID: 30211049]
Ben-Menachem Y,Coldwell DM,Young JW,Burgess AR, Hemorrhage associated with pelvic fractures: causes, diagnosis, and emergent management. AJR. American journal of roentgenology. 1991 Nov; [PubMed PMID: 1927786]
Agri F, Bourgeat M, Becce F, Moerenhout K, Pasquier M, Borens O, Yersin B, Demartines N, Zingg T. Association of pelvic fracture patterns, pelvic binder use and arterial angio-embolization with transfusion requirements and mortality rates; a 7-year retrospective cohort study. BMC surgery. 2017 Nov 9:17(1):104. doi: 10.1186/s12893-017-0299-6. Epub 2017 Nov 9 [PubMed PMID: 29121893]
Level 2 (mid-level) evidenceChou CH, Wu YT, Fu CY, Liao CH, Wang SY, Bajani F, Hsieh CH. Hemostasis as soon as possible? The role of the time to angioembolization in the management of pelvic fracture. World journal of emergency surgery : WJES. 2019:14():28. doi: 10.1186/s13017-019-0248-z. Epub 2019 Jun 13 [PubMed PMID: 31210779]
Broadwell SR, Ray CE. Transcatheter embolization in pelvic trauma. Seminars in interventional radiology. 2004 Mar:21(1):23-35. doi: 10.1055/s-2004-831402. Epub [PubMed PMID: 21331106]
Miller PR,Moore PS,Mansell E,Meredith JW,Chang MC, External fixation or arteriogram in bleeding pelvic fracture: initial therapy guided by markers of arterial hemorrhage. The Journal of trauma. 2003 Mar; [PubMed PMID: 12634521]
Balogh Z, Caldwell E, Heetveld M, D'Amours S, Schlaphoff G, Harris I, Sugrue M. Institutional practice guidelines on management of pelvic fracture-related hemodynamic instability: do they make a difference? The Journal of trauma. 2005 Apr:58(4):778-82 [PubMed PMID: 15824655]
Level 1 (high-level) evidenceShim H, Jang JY, Kim JW, Ryu H, Jung PY, Kim S, Kwon HY, Kim KM, Chung H, Bae KS. Effectiveness and postoperative wound infection of preperitoneal pelvic packing in patients with hemodynamic instability caused by pelvic fracture. PloS one. 2018:13(11):e0206991. doi: 10.1371/journal.pone.0206991. Epub 2018 Nov 5 [PubMed PMID: 30395596]
Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. The Journal of trauma. 2011 Dec:71(6):1869-72. doi: 10.1097/TA.0b013e31823fe90c. Epub [PubMed PMID: 22182896]
Jarvis S,Kelly M,Mains C,Corrigan C,Patel N,Carrick M,Lieser M,Banton K,Bar-Or D, A descriptive survey on the use of resuscitative endovascular balloon occlusion of the aorta (REBOA) for pelvic fractures at US level I trauma centers. Patient safety in surgery. 2019 [PubMed PMID: 31857823]
Level 3 (low-level) evidenceMoore LJ, Martin CD, Harvin JA, Wade CE, Holcomb JB. Resuscitative endovascular balloon occlusion of the aorta for control of noncompressible truncal hemorrhage in the abdomen and pelvis. American journal of surgery. 2016 Dec:212(6):1222-1230. doi: 10.1016/j.amjsurg.2016.09.027. Epub 2016 Sep 30 [PubMed PMID: 28340927]
Ribeiro Junior MAF, Feng CYD, Nguyen ATM, Rodrigues VC, Bechara GEK, de-Moura RR, Brenner M. The complications associated with Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). World journal of emergency surgery : WJES. 2018:13():20. doi: 10.1186/s13017-018-0181-6. Epub 2018 May 11 [PubMed PMID: 29774048]
Gamberini E, Coccolini F, Tamagnini B, Martino C, Albarello V, Benni M, Bisulli M, Fabbri N, Hörer TM, Ansaloni L, Coniglio C, Barozzi M, Agnoletti V. Resuscitative Endovascular Balloon Occlusion of the Aorta in trauma: a systematic review of the literature. World journal of emergency surgery : WJES. 2017:12():42. doi: 10.1186/s13017-017-0153-2. Epub 2017 Aug 29 [PubMed PMID: 28855960]
Level 1 (high-level) evidenceHalawi MJ, Pelvic ring injuries: Surgical management and long-term outcomes. Journal of clinical orthopaedics and trauma. 2016 Jan-Mar; [PubMed PMID: 26908968]
Calafi LA, Routt ML. Anterior pelvic external fixation: is there an optimal placement for the supra-acetabular pin? American journal of orthopedics (Belle Mead, N.J.). 2013 Dec:42(12):E125-7 [PubMed PMID: 24471155]
Lee C, Sciadini M. The Use of External Fixation for the Management of the Unstable Anterior Pelvic Ring. Journal of orthopaedic trauma. 2018 Sep:32 Suppl 6():S14-S17. doi: 10.1097/BOT.0000000000001251. Epub [PubMed PMID: 30095676]
Gordon WT, Fleming ME, Johnson AE, Gurney J, Shackelford S, Stockinger ZT. Pelvic Fracture Care. Military medicine. 2018 Sep 1:183(suppl_2):115-117. doi: 10.1093/milmed/usy111. Epub [PubMed PMID: 30189052]
Pape HC, Griensven MV, Hildebrand FF, Tzioupis CT, Sommer KL, Krettek CC, Giannoudis PV, Epoff Study group. Systemic inflammatory response after extremity or truncal fracture operations. The Journal of trauma. 2008 Dec:65(6):1379-84. doi: 10.1097/TA.0b013e31818c8e8c. Epub [PubMed PMID: 19077630]
Level 2 (mid-level) evidenceHak DJ, Baran S, Stahel P. Sacral fractures: current strategies in diagnosis and management. Orthopedics. 2009 Oct:32(10):. pii: orthosupersite.com/view.asp?rID=44034. doi: 10.3928/01477447-20090818-18. Epub [PubMed PMID: 19824583]
Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management. The Journal of the American Academy of Orthopaedic Surgeons. 2013 Aug:21(8):458-68. doi: 10.5435/JAAOS-21-08-458. Epub [PubMed PMID: 23908252]
Mehta S, Auerbach JD, Born CT, Chin KR. Sacral fractures. The Journal of the American Academy of Orthopaedic Surgeons. 2006 Nov:14(12):656-65 [PubMed PMID: 17077338]
Inaba K, McKenney M, Munera F, de Moya M, Lopez PP, Schulman CI, Habib FA. Cystogram follow-up in the management of traumatic bladder disruption. The Journal of trauma. 2006 Jan:60(1):23-8 [PubMed PMID: 16456432]
Level 2 (mid-level) evidenceChung PH, Wessells H, Voelzke BB. Updated Outcomes of Early Endoscopic Realignment for Pelvic Fracture Urethral Injuries at a Level 1 Trauma Center. Urology. 2018 Feb:112():191-197. doi: 10.1016/j.urology.2017.09.032. Epub 2017 Oct 25 [PubMed PMID: 29079211]
Maxwell RA, Fabian TC. Current management of colon trauma. World journal of surgery. 2003 Jun:27(6):632-9 [PubMed PMID: 12724824]
Navsaria PH, Edu S, Nicol AJ. Civilian extraperitoneal rectal gunshot wounds: surgical management made simpler. World journal of surgery. 2007 Jun:31(6):1345-51 [PubMed PMID: 17457641]
Level 2 (mid-level) evidenceBosarge PL, Como JJ, Fox N, Falck-Ytter Y, Haut ER, Dorion HA, Patel NJ, Rushing A, Raff LA, McDonald AA, Robinson BR, McGwin G Jr, Gonzalez RP. Management of penetrating extraperitoneal rectal injuries: An Eastern Association for the Surgery of Trauma practice management guideline. The journal of trauma and acute care surgery. 2016 Mar:80(3):546-51. doi: 10.1097/TA.0000000000000953. Epub [PubMed PMID: 26713970]
Yoshihara H, Yoneoka D. Demographic epidemiology of unstable pelvic fracture in the United States from 2000 to 2009: trends and in-hospital mortality. The journal of trauma and acute care surgery. 2014 Feb:76(2):380-5. doi: 10.1097/TA.0b013e3182ab0cde. Epub [PubMed PMID: 24398776]
Level 2 (mid-level) evidenceVaidya R, Scott AN, Tonnos F, Hudson I, Martin AJ, Sethi A. Patients with pelvic fractures from blunt trauma. What is the cause of mortality and when? American journal of surgery. 2016 Mar:211(3):495-500. doi: 10.1016/j.amjsurg.2015.08.038. Epub 2015 Dec 31 [PubMed PMID: 26781723]
McDonald C, Firoozabadi R, Routt ML Jr, Kleweno C. Complications Associated With Pelvic External Fixation. Orthopedics. 2017 Nov 1:40(6):e959-e963. doi: 10.3928/01477447-20170918-02. Epub 2017 Sep 22 [PubMed PMID: 28934542]
Bauer RM, Bastian PJ, Gozzi C, Stief CG. Postprostatectomy incontinence: all about diagnosis and management. European urology. 2009 Feb:55(2):322-33. doi: 10.1016/j.eururo.2008.10.029. Epub 2008 Oct 23 [PubMed PMID: 18963418]
Bananzadeh A, Hosseini SV, Izadpanah A, Izadi A, Khazraei H, Zamani M, Bahrami F. Outcomes of Implementation of Sacral Nerve Stimulation in Incontinent Patients in Shiraz. Advanced biomedical research. 2019:8():21. doi: 10.4103/abr.abr_202_18. Epub 2019 Mar 20 [PubMed PMID: 31016179]
Saldana Ruiz N, Kaiser AM. Fecal incontinence - Challenges and solutions. World journal of gastroenterology. 2017 Jan 7:23(1):11-24. doi: 10.3748/wjg.v23.i1.11. Epub [PubMed PMID: 28104977]