Introduction
The peroneal nerve, or the fibular nerve, is a significant nerve innervating the lower extremity. With fibers originating from the posterior divisions of L4–S2, the peroneal and tibial nerves are the primary branches of the sciatic nerve, which bifurcates into the tibial and common peroneal nerves proximal to the popliteal fossa in the distal posterior thigh. The common peroneal nerve (CPN) then courses posterolaterally behind the long head of the biceps femoris muscle before moving anteriorly to wrap around the fibular neck and pass beneath the lateral compartment of the calf. The CPN divides into deep and superficial branches after curving around the fibular neck. The deep peroneal nerve (DPN) courses between the tibialis anterior and hallucis longus muscles in the anterior compartment of the leg, then continues along the anterior tibia before terminating in the webspace between the first and second toes. The superficial peroneal nerve (SPN) descends through the lateral compartment of the leg before terminating at the dorsum of the ankle and foot.[1] Anatomical variation is possible. As an example, the accessory fibular nerve, present in approximately 25% of the general population, is an anatomic variant innervating the extensor digitorum brevis muscle.[2]
The peroneal nerve subserves both sensory and motor functions. Motor function of the DPN permits dorsiflexion of the foot and extension of the great toe; the SPN subserves ankle eversion. Sensory function of the SPN supplies the dorsum of the foot except for the interdigital space between the first and second toes, which is supplied by the DPN.
After median and ulnar neuropathies, peroneal neuropathy is the most common focal neuropathy; peroneal neuropathy is the most common compressive neuropathy of the lower extremity.[3] Symptoms of CPN mononeuropathy classically include numbness of the dorsum of the foot and the lateral leg along with foot drop—the latter occurring secondary to paresis of ankle and toe dorsiflexion plus weakness of foot eversion—with its distinctive accompanying steppage gait.[3]
Traumatic and behavioral causes alike can precipitate peroneal neuropathy, with trauma usually occurring acutely, whereas behavior contributes more to chronic presentations. Compressive peroneal neuropathy commonly afflicts athletes and individuals whose work otherwise necessitates substantial kneeling and squatting.
This topic reviews injuries to the common peroneal nerve and its branches, including etiology, epidemiology, salient features of the history and physical exam findings, plus diagnosis and treatment.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Peroneal nerve injury has been attributed to numerous causes, both traumatic and atraumatic.[4][5][6] Common causes of damage to the peroneal nerve include the following:
- Anatomic risk factors
- A fibrous band at the origin of the peroneus longus muscle near the fibrillar head predisposes to compressive neuropathy of the CPN [7][8]
- The extensor retinaculum atop the ankle can entrap the DPN between it and the underlying navicular and talus bones, causing the relatively rare condition known as anterior tarsal tunnel syndrome [9]
- Fabella syndrome occurs when the fabella, a sesamoid bone present in the gastrocnemius muscle in 1% to 30% of the general population, compresses the CPN through direct articular contact with the lateral femoral condyle [10][11]
- Trauma or injury to the knee joint
- Knee dislocation causes CPN injury in up to 40% of patients experiencing acute dislocations[12][13]
- Direct impact, penetrating trauma, or laceration predisposes to CPN injury as the nerve courses around the fibular head/neck
- Fracture of the fibula, especially at the proximal fibula
- Fracture of the tibia, including the tibial plateau
- External compression sources
- Tight splints or casts
- Compression wrappings or bandages
- Habitual leg crossing
- Prolonged bed rest, including in comatose patients or those intubated for long periods.
- Positioning during anesthesia and surgery can lead to compression injury, especially in the setting of inadequately padded bony prominences like the fibular head.
- Intraneural ganglion cysts [14]
- Peripheral nerve tumors [15]
- Iatrogenic injury following surgery on the hip, knee (including total knee arthroplasty and arthroscopic lateral meniscus repair), or ankle [16]
The common peroneal nerve is most vulnerable to injury as it passes around the fibular neck. Therefore, it is most susceptible to injury at the lateral aspect of the knee.[17][18]
Significant trauma around the knee can also result in peroneal nerve injury due to the nerve’s proximity to the knee joint and its superficial location; this can include a direct impact on the fibular neck, lacerations, and knee dislocations. CPN injuries are often encountered in athletes, especially football or soccer players, where they are most commonly associated with knee dislocation and ligamentous injury or occur in isolation.[18]
Several systemic illnesses can cause compressive peroneal neuropathy and injury to the common peroneal nerve, including:
Epidemiology
Peroneal nerve injury is recognized as the most common neuropathy of the lower extremity and the third most common neuropathy overall, with only neuropathy of the median and ulnar nerves occurring more often.[3] Traumatic injuries to the CPN usually occur in young athletic patients (eg, football and soccer players) and in adult patients following high-energy trauma (eg, motor vehicle collisions), with CPN injury reportedly occurring in 16% to 40% of patients following knee dislocations.[13] Low-energy knee dislocations can occur in morbidly obese patients during basic activities of daily living.[21]
Given the lack of prospectively acquired data, the overall incidence of peroneal nerve injury secondary to closed fractures is challenging to elucidate. Fractures of the tibia (including tibial plateau) and fibula are reportedly associated with approximately a 1% to 2% rate of peroneal nerve injury.[22] There are reports of even rarer incidences following total knee arthroplasty or arthroscopic lateral meniscal repair.[18] For foot drop, the most recognizable consequence of peroneal nerve injury, data regarding overall incidence has not been reported to date.[23]
History and Physical
A thorough history and physical exam to assess the status and functional integrity of the CPN is always required when injury is possible. Presentation varies according to the underlying locus of compression or other injury to the nerve.[7]
The examining clinician should always seek information about prior history of total knee arthroplasty, exposure to epidural anesthesia, prior knee conditions such as valgus deformity, periods of higher body weight, and the presence of diabetes.
The most common presentation of CPN injury is a weakness of ankle dorsiflexion leading to the classic foot drop, which often causes patients to catch their toes on the ground while ambulating or ambulate with a high steppage gait to prevent dragging their toes on the ground. Foot drop may develop acutely or over days to weeks, depending on the etiology. It can also be complete or partial in severity. Accompanying numbness or paresthesia may occur along the lateral leg, dorsal foot, and first toe webspace. Pain may be present in traumatic cases, but this is not universal.[18]
In the setting of traumatic injuries to the knee, including knee dislocations, the initial examination must rule out an acute neurovascular injury that could potentially compromise the lower extremity. Knee dislocations can notoriously compromise the neurovascular structures passing from the thigh and knee to the lower limb. If not addressed urgently, neurovascular compromise can lead to acute compartment syndrome, which can result in long-term compromise to the lower limb, even requiring amputation.[24][25]
To test for the motor involvement of the SPN and DPN, one must assess foot eversion (SPN) and dorsiflexion of the ankle and toe joints (DPN). A finding of weak foot eversion in the company of weak ankle and toe dorsiflexion suggests a lesion involving the CPN.[18] More proximal lesions, often secondary to traumatic knee dislocations, may present with varying degrees of numbness in both SPN and DPN distributions.
The Tinel sign is also a reliable clinical sign for localization of the area of nerve irritation or entrapment. The examiner performs the Tinel test by tapping along the course of the nerve, particularly around the fibular neck. Tingling or paresthesia elicited distally to the point of compression by tapping denotes a positive Tinel sign.[26]
The following tests can quickly evaluate the motor and sensory integrity of the CPN and its branches:
Motor
- Common peroneal nerve: none
- Superficial peroneal nerve: eversion of the foot
- Deep peroneal nerve: dorsiflexion of the foot and great toe extension
Sensory
- Common peroneal nerve: lateral aspect of the leg just distal to the knee
- Superficial peroneal nerve: the anterolateral distal third of the leg and the majority of the dorsum of the foot (except the first webspace)
- Deep peroneal nerve: first dorsal webspace
Evaluation
The CPN’s superficial location and proximity to the fibular neck make the nerve particularly susceptible to injury, both from direct trauma and from entrapment by soft and bony tissue. When the history and physical examination indicate injury to the CPN, plain radiography should be part of the initial workup. In addition to plain radiography, CT scans can be used to evaluate for additional osseous abnormalities. MRI or ultrasound can be used to assess soft-tissue sources or masses.[5][27]
Electrodiagnostic studies, including electromyography and nerve conduction velocity, can be helpful in assessing CPN palsy. These tests interrogate the motor and sensory axons of the CPN and its branches. They are also helpful in the localization of nerve injury. These tests are useful in patients presenting with a new onset of peroneal nerve symptoms, such as foot drop without a traumatic mechanism, in addition to evaluating patients in the postoperative setting of a known traumatic peroneal nerve injury to plan long-term management.
Treatment / Management
There are operative and nonoperative options for the treatment of CPN injuries. Nonoperative treatments include ankle-foot orthoses and physical therapy. An ankle-foot orthotic device provides toe dorsiflexion during the gait’s swing phase, medial or lateral stability at the ankle during stance, and, if necessary, some push-off stimulation during the late stance phase.[28] Recent advances in ankle-foot orthotics include using carbon fiber to increase the energy available for push-off during the stance phase; the lighter weight improves patient comfort. Physical therapy for CPN injury consists of a program of stretching, strengthening, mobilization, manipulation, and proprioceptive and balancing exercises. Physical therapy may also include icing, ankle bracing, and taping. A recent case report described the use of ultrasound-guided pulsed radiofrequency treatment to alleviate symptoms of SPN entrapment neuropathy in a handball player.[29](B3)
Indications for surgical approaches to CPN injuries include a rapidly deteriorating lesion, refractoriness without improvement for 3 months, and open injuries with suspected nerve laceration.[5] Open lacerations should undergo exploration and surgical repair within 72 hours.[5] More than that, though, any patient with a subjectively disturbing foot drop and a clinically suspected compressive neuropathy of the CPN should be informed that surgical decompression of the nerve at the fibular head can be performed with little risk. Some patients have benefitted from muscle-transfer surgery in cases of a permanent foot drop. For spastic foot drop, the option of botulinum toxin injections should be evaluated.[23] During surgical procedures, prevention of CPN injuries entails the padding of relevant bony prominences, including the fibular head and neck at the lateral aspect of the knee.
Differential Diagnosis
Foot drop can be caused by (lower) lumbar radiculopathy and lesions of the sciatic notch, in addition to the more classic cause of CPN neuropathy.[30] Cases of peroneal injury have been reported after total hip arthroplasty.
Peroneal neuropathy is found in patients with multiple system atrophy. In one study, decreased compound muscle action potentials in the peroneal nerve were found in 8.6% of patients with the Parkinsonian variant and 4.3% of patients with the cerebellar variant.[31]
Prognosis
The prognosis depends on etiology. While some transient CPN neuropathies improve or resolve over time with nonsurgical measures, CPN palsy following traumatic knee dislocations has a poor prognosis for the long-term recovery of nerve function.[32] Surgical intervention and tendon transfers are often necessary for refractory CPN palsy, dictated by results of follow-up physical examination and serial electromyographic testing with nerve conduction velocities.
The prognosis has been described extensively in patients who experience CPN injury following total knee arthroplasty. In one study, 62% of patients experienced maximal neurologic recovery, and 38% had complete recovery at 12 months.[33] In another large case series study of 318 operatively-managed peroneal nerve lesions associated with various mechanisms, 84% of patients who underwent end-to-end suture repair received good recovery by 24 months.[5] In patients who required grafts, graft lengths less than 6 cm recovered 75% function. Longer grafts were associated with poorer outcomes.[5]
Complications
In patients with foot drop, the clinician must ensure that the physical therapy and rehabilitation care teams engage in passive stretching exercises to mitigate the risks of a fixed equinovarus contracture. Orthotic devices are used to ensure the ankle can achieve at least passive dorsiflexion to a neutral position.[18]
Deterrence and Patient Education
The care team is responsible for educating patients on the treatment options available for CPN injuries, including the prognosis and complications that accompany each. Patients should follow their individualized treatment plans for the best results. Patients should maintain regular contact and follow up with their physician to ensure appropriate care. In almost all cases, patients benefit from constructive advice about the perils of nerve compression arising from crossing the legs for long periods.
Pearls and Other Issues
Key facts to keep in mind regarding peroneal nerve injury include the following:
- The most common presentation in CPN injury or palsy is acute foot drop, although symptoms may be progressive and can include sensory loss or pain.
- Weakness in foot eversion may occur if the SPN is involved.
- Weakness in dorsiflexion of the foot and great toe extension suggests DPN involvement.
- Sensation in the webspace between the great and second toes is subserved by the DPN.
- The CPN has no motor function.
- The prognosis for common peroneal nerve injury is good following end-to-end suture repair as well as grafting.
Enhancing Healthcare Team Outcomes
Patients with CPN dysfunction experience a wide range of prognoses along a spectrum, depending on the underlying etiology. To offer adequate treatment to patients with CPN injuries, specialists, including neurologists and orthopedic surgeons, must coordinate and work closely with primary care physicians, nurse practitioners, physician assistants, and physical therapists to ensure appropriate management and outcomes. Orthotists contribute to care and recovery by making ankle-foot orthotics to help with coordinated rehabilitation efforts.
The key to managing injury to the CPN is early recognition and timely referral to the appropriate specialist. The patient requires monitoring for recovery, which, in many cases, may take weeks or months. The emergency department physician should be able to recognize CPN injuries and consult with the orthopedic surgeon. The ankle-foot orthotist can help with ambulation. The physical therapist should educate the patient on ambulation, ankle bracing, and the use of an assistive device. A wound care nurse should follow patients with open wounds until complete healing has occurred. Post-surgical pain control can benefit from pharmacist involvement, assisting with agent selection as well as minimizing opioid use. Communication among all involved disciplines is paramount, permitting everyone on the interprofessional team to understand the complete clinical picture and make decisions based on the patient’s current status.
Media
(Click Image to Enlarge)
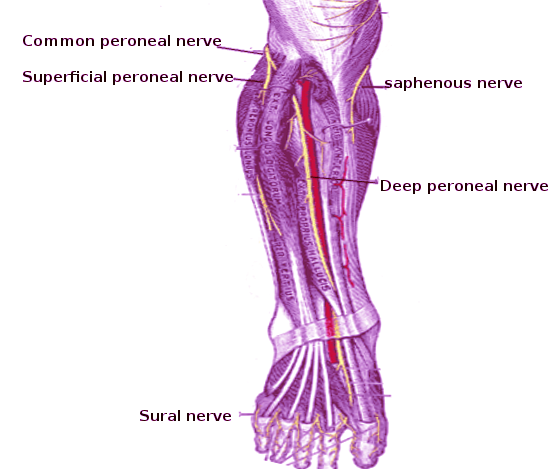
Peroneal Nerve
Image courtesy O Chaigasame
References
Capodici A, Hagert E, Darrach H, Curtin C. An overview of common peroneal nerve dysfunction and systematic assessment of its relation to falls. International orthopaedics. 2022 Dec:46(12):2757-2763. doi: 10.1007/s00264-022-05593-w. Epub 2022 Sep 28 [PubMed PMID: 36169699]
Level 1 (high-level) evidenceDrăghici NC, Văcăraș V, Bolchis R, Bashimov A, Domnița DM, Iluț S, Popa LL, Lupescu TD, Mureșanu DF. Diagnostic Approach to Lower Limb Entrapment Neuropathies: A Narrative Literature Review. Diagnostics (Basel, Switzerland). 2023 Nov 4:13(21):. doi: 10.3390/diagnostics13213385. Epub 2023 Nov 4 [PubMed PMID: 37958280]
Bowley MP, Doughty CT. Entrapment Neuropathies of the Lower Extremity. The Medical clinics of North America. 2019 Mar:103(2):371-382. doi: 10.1016/j.mcna.2018.10.013. Epub 2018 Dec 3 [PubMed PMID: 30704688]
Baima J, Krivickas L. Evaluation and treatment of peroneal neuropathy. Current reviews in musculoskeletal medicine. 2008 Jun:1(2):147-53. doi: 10.1007/s12178-008-9023-6. Epub [PubMed PMID: 19468889]
Poage C, Roth C, Scott B. Peroneal Nerve Palsy: Evaluation and Management. The Journal of the American Academy of Orthopaedic Surgeons. 2016 Jan:24(1):1-10. doi: 10.5435/JAAOS-D-14-00420. Epub [PubMed PMID: 26700629]
Gloobe H, Chain D. Fibular fibrous arch. Anatomical considerations in fibular tunnel syndrome. Acta anatomica. 1973:85(1):84-7 [PubMed PMID: 4713100]
Fortier LM, Markel M, Thomas BG, Sherman WF, Thomas BH, Kaye AD. An Update on Peroneal Nerve Entrapment and Neuropathy. Orthopedic reviews. 2021:13(2):24937. doi: 10.52965/001c.24937. Epub 2021 Jun 19 [PubMed PMID: 34745471]
Rausch V, Hackl M, Oppermann J, Leschinger T, Scaal M, Müller LP, Wegmann K. Peroneal nerve location at the fibular head: an anatomic study using 3D imaging. Archives of orthopaedic and trauma surgery. 2019 Jul:139(7):921-926. doi: 10.1007/s00402-019-03141-7. Epub 2019 Feb 8 [PubMed PMID: 30737594]
Moonot P, Karwande N, Dakhode S, Thorat T. Anterior Tarsal Tunnel Syndrome: Entrapment of the Articular Branch of Deep Peroneal Nerve: A Case Report. JBJS case connector. 2023 Oct 1:13(4):. doi: e23.00253. Epub 2023 Dec 8 [PubMed PMID: 38064579]
Level 3 (low-level) evidenceLin JC, Tsai MH, Lin WP, Kuan TS, Lien WC. Entrapment neuropathy of common peroneal nerve by fabella: A case report. World journal of clinical cases. 2023 Oct 6:11(28):6857-6863. doi: 10.12998/wjcc.v11.i28.6857. Epub [PubMed PMID: 37901021]
Level 3 (low-level) evidenceDiaz CC, Agarwalla A, Forsythe B. Fabella Syndrome and Common Peroneal Neuropathy following Total Knee Arthroplasty. Case reports in orthopedics. 2021:2021():7621844. doi: 10.1155/2021/7621844. Epub 2021 Sep 2 [PubMed PMID: 34513102]
Level 3 (low-level) evidenceLaPrade RF, Terry GC. Injuries to the posterolateral aspect of the knee. Association of anatomic injury patterns with clinical instability. The American journal of sports medicine. 1997 Jul-Aug:25(4):433-8 [PubMed PMID: 9240974]
Moatshe G, Dornan GJ, Løken S, Ludvigsen TC, LaPrade RF, Engebretsen L. Demographics and Injuries Associated With Knee Dislocation: A Prospective Review of 303 Patients. Orthopaedic journal of sports medicine. 2017 May:5(5):2325967117706521. doi: 10.1177/2325967117706521. Epub 2017 May 22 [PubMed PMID: 28589159]
Yunga Tigre J, Maddy K, Errante EL, Costello MC, Steinlauf S, Burks SS. Recurrent Peroneal Intraneural Ganglion Cyst: Management and Review of the Literature. Cureus. 2023 May:15(5):e38449. doi: 10.7759/cureus.38449. Epub 2023 May 2 [PubMed PMID: 37273377]
Liu Z, Yushan M, Liu Y, Yusufu A. Prognostic factors in patients who underwent surgery for common peroneal nerve injury: a nest case-control study. BMC surgery. 2021 Jan 6:21(1):11. doi: 10.1186/s12893-020-01033-x. Epub 2021 Jan 6 [PubMed PMID: 33407374]
Level 2 (mid-level) evidenceBage T, Power DM. Iatrogenic peripheral nerve injury: a guide to management for the orthopaedic limb surgeon. EFORT open reviews. 2021 Aug:6(8):607-617. doi: 10.1302/2058-5241.6.200123. Epub 2021 Aug 10 [PubMed PMID: 34532069]
Hardin JM, Devendra S. Anatomy, Bony Pelvis and Lower Limb: Calf Common Peroneal Nerve (Common Fibular Nerve). StatPearls. 2024 Jan:(): [PubMed PMID: 30422563]
Marciniak C. Fibular (peroneal) neuropathy: electrodiagnostic features and clinical correlates. Physical medicine and rehabilitation clinics of North America. 2013 Feb:24(1):121-37. doi: 10.1016/j.pmr.2012.08.016. Epub 2012 Oct 26 [PubMed PMID: 23177035]
Jaeger JA, Gohil A, Nebesio TD. Acute Peroneal Neuropathy and Foot Drop in Two Adolescent Female Athletes with New-Onset Diabetes. Current sports medicine reports. 2022 Feb 1:21(2):39-41. doi: 10.1249/JSR.0000000000000931. Epub [PubMed PMID: 35120048]
Weerasinghe D, Veerapandiyan A, Stanton M, Herrmann DN, Akmyradov C, Logigian E. Recovery of foot drop in chronic inflammatory demyelinating polyneuropathy (CIDP). Muscle & nerve. 2021 Jul:64(1):59-63. doi: 10.1002/mus.27253. Epub 2021 Apr 30 [PubMed PMID: 33876440]
Smith PJ, Azar FM. Knee Dislocations in the Morbidly Obese Patient. Sports medicine and arthroscopy review. 2020 Sep:28(3):110-115. doi: 10.1097/JSA.0000000000000273. Epub [PubMed PMID: 32740463]
Noble J, Munro CA, Prasad VS, Midha R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. The Journal of trauma. 1998 Jul:45(1):116-22 [PubMed PMID: 9680023]
Carolus AE, Becker M, Cuny J, Smektala R, Schmieder K, Brenke C. The Interdisciplinary Management of Foot Drop. Deutsches Arzteblatt international. 2019 May 17:116(20):347-354. doi: 10.3238/arztebl.2019.0347. Epub [PubMed PMID: 31288916]
Varacallo M, Shirey L, Kavuri V, Harding S. Acute compartment syndrome of the hand secondary to propofol extravasation. Journal of clinical anesthesia. 2018 Jun:47():1-2. doi: 10.1016/j.jclinane.2018.01.020. Epub 2018 Feb 21 [PubMed PMID: 29476968]
Chandwani D, Varacallo M. Exertional Compartment Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 31335004]
Heinrich K, Pumberger P, Schwaiger K, Schaffler G, Hladik M, Wechselberger G. [Surgical decompression of the peroneal nerve at the level of the fibular head]. Operative Orthopadie und Traumatologie. 2020 Oct:32(5):467-474. doi: 10.1007/s00064-020-00648-w. Epub 2020 Feb 25 [PubMed PMID: 32100068]
Schwabl C, Schmidle G, Kaiser P, Drakonaki E, Taljanovic MS, Klauser AS. Nerve entrapment syndromes: detection by ultrasound. Ultrasonography (Seoul, Korea). 2023 Jul:42(3):376-387. doi: 10.14366/usg.22186. Epub 2023 Feb 2 [PubMed PMID: 37343936]
Choo YJ, Chang MC. Commonly Used Types and Recent Development of Ankle-Foot Orthosis: A Narrative Review. Healthcare (Basel, Switzerland). 2021 Aug 13:9(8):. doi: 10.3390/healthcare9081046. Epub 2021 Aug 13 [PubMed PMID: 34442183]
Level 3 (low-level) evidenceMartins da Silva R, Pereira A, Branco R, Carvalho JL. Ultrasound-Guided Pulsed Radiofrequency Treatment for Superficial Peroneal Nerve Entrapment in a Professional Handball Player. Cureus. 2023 Jul:15(7):e42043. doi: 10.7759/cureus.42043. Epub 2023 Jul 17 [PubMed PMID: 37593284]
Seruya M. Differential Diagnosis of "Foot Drop": Implications for Peripheral Nerve Surgery. Journal of reconstructive microsurgery. 2024 Jan 24:():. doi: 10.1055/a-2253-6360. Epub 2024 Jan 24 [PubMed PMID: 38267007]
Gawel M, Jamrozik Z, Szmidt-Salkowska E, Slawek J, Rowinska-Marcinska K. Is peripheral neuron degeneration involved in multiple system atrophy? A clinical and electrophysiological study. Journal of the neurological sciences. 2012 Aug 15:319(1-2):81-5. doi: 10.1016/j.jns.2012.05.011. Epub 2012 May 28 [PubMed PMID: 22647584]
O'Malley MP, Pareek A, Reardon P, Krych A, Stuart MJ, Levy BA. Treatment of Peroneal Nerve Injuries in the Multiligament Injured/Dislocated Knee. The journal of knee surgery. 2016 May:29(4):287-92. doi: 10.1055/s-0035-1570019. Epub 2015 Dec 18 [PubMed PMID: 26683981]
Park JH, Restrepo C, Norton R, Mandel S, Sharkey PF, Parvizi J. Common peroneal nerve palsy following total knee arthroplasty: prognostic factors and course of recovery. The Journal of arthroplasty. 2013 Oct:28(9):1538-42. doi: 10.1016/j.arth.2013.02.025. Epub 2013 Apr 4 [PubMed PMID: 23562462]