Introduction
The shoulder is structurally and functionally complex as it is one of the most freely moveable areas in the human body due to the articulation at the glenohumeral joint. It contains the shoulder girdle, which connects the upper limb to the axial skeleton via the sternoclavicular joint. The high range of motion of the shoulder comes at the expense of decreased stability of the joint, and it is prone to dislocation and injury.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The shoulder girdle is composed of the clavicle and the scapula, which articulates with the proximal humerus of the upper limb. Four joints are present in the shoulder: the sternoclavicular (SC), acromioclavicular (AC), and scapulothoracic joints, and glenohumeral joint.
The sternoclavicular joint is a synovial saddle joint and is the only joint that connects the upper limb to the axial skeleton. It connects the clavicle to the manubrium of the sternum and gets stabilization from the costoclavicular ligament. The acromioclavicular joint is a plane synovial joint that connects the acromion of the scapula to the clavicle. It receives stabilization primarily from the coracoclavicular ligament, and secondary stabilizers are super and inferior acromioclavicular ligaments. The scapulothoracic joint is not a true joint, but rather the articulation of the scapula gliding over the posterior thoracic cage.
The glenohumeral joint is a highly moveable ball-and-socket synovial joint that is stabilized by the rotator cuff muscles that attach to the joint capsule, as well as the tendons of the biceps and triceps brachii. The humeral head articulates with the glenoid fossa of the scapula. It is a shallow articulation, as the fossa accommodates less than one-third of the humeral head. The labrum, a fibrocartilaginous ring, attaches to the outer rim of the glenoid fossa and provides additional depth and stability securing the humeral head. A small number of fluid-filled sacs known as bursae surround the capsule and aid in mobility. These are the subacromial, subdeltoid, subscapular, and subcoracoid bursae.
The major movements at the glenohumeral joint are:
- Abduction: upward lateral movement of humerus out to the side, away from the body, in the plane of the scapula
- Adduction: downward movement of humerus medially toward the body from abduction, in the plane of the scapula
- Flexion: the movement of humerus straight anteriorly
- Extension: the movement of humerus straight posteriorly
- External rotation: the movement of humerus laterally around its long axis away from the midline
- Internal rotation: the movement of humerus medially around its long axis toward the midline
- Horizontal adduction (transverse flexion): the movement of the humerus in a horizontal or transverse plane toward and across the chest
- Horizontal abduction (transverse extension): the movement of the humerus in a horizontal or transverse plane away from the chest
Embryology
All elements of the human body arise from the three primary germ layers in the young embryo: the ectoderm, endoderm, and mesoderm. Cartilage, bone (and marrow), muscles and ligaments, and connective tissue all arise from the mesoderm, which lies between the ectoderm and endoderm.
Blood Supply and Lymphatics
The axillary artery is the major blood vessel in the shoulder, with many of its branches supplying the area. These branches include the superior thoracic artery, thoracoacromial artery, lateral thoracic artery, subscapular artery, anterior humeral circumflex artery, and posterior humeral circumflex artery. Before becoming the axillary artery, after passing beyond the lateral edge of the first rib, the subclavian artery also includes branches that supply the area of the shoulder. The thyrocervical trunk off of the subclavian artery adds the suprascapular artery and the transverse cervical artery. The dorsal scapular artery most often branches off of the subclavian, but may sometimes branch off the transverse cervical artery.
Nerves
See the "Muscles" section for innervations.
Muscles
The intrinsic muscles of the shoulder connect the scapula and/or clavicle to the humerus. These include[1]
Deltoid
- Function:
- Anterior aspect is responsible for flexion and medial rotation of the arm
- Middle aspect is responsible for the abduction of the arm (up to 90 degrees)
- The posterior aspect is responsible for extension and lateral rotation of the arm
- Origin: Lateral clavicle, acromion and scapular spine
- Insertion: Deltoid tuberosity
- Innervation: Axillary nerve (C5, C6)
Teres major
- Function: Adduction and medial rotation of the arm
- Origin: Posterior surface of the scapula at its inferior angle
- Insertion: Intertubercular groove of the proximal humerus on its medial aspect
- Innervation: Lower scapular nerve (C5, C6)
Supraspinatus (Rotator Cuff)
- Function: Initiation of arm abduction (first 15 degrees), stabilize glenohumeral joint
- Origin: Posterior scapula, superior to the scapular spine/supraspinous fossa
- Insertion: Top of the greater tubercle of the humerus
- Innervation: Suprascapular nerve (C5, C6)
Infraspinatus (Rotator Cuff)
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Posterior scapula, inferior to the scapular spine/Infraspinous fossa
- Insertion: Greater tubercle of the humerus, between the supraspinatus and teres minor insertion
- Innervation: Suprascapular nerve (C5, C6)
Teres minor (Rotator Cuff)
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Inferior angle of the scapula
- Insertion: Inferior aspect of the greater tubercle
- Innervation: Axillary nerve (C5, C6)
Subscapularis (Rotator Cuff)
- Function: Adduction and medial rotation of the arm, stabilize glenohumeral joint
- Origin: Anterior aspect of the scapula
- Insertion: Lesser tubercle of the humerus
- Innervation: Subscapular nerves (C5, C6, C7)
Other muscles that affect movement at the shoulder joint include:
Trapezius
- Function:
- Upper fibers elevate the scapula and rotate it during abduction of the arm (90 to 180 degrees)
- Middle fibers retract the scapula
- Lower fibers pull the scapula inferiorly.
- Origin: Skull, nuchal ligament and the spinous processes of C7 to T12
- Insertion: clavicle, acromion and the scapular spine
- Innervation: Accessory nerve (C5, C6)
Latissmus dorsi
- Function: Extends, adducts and medially rotates the upper limb
- Origin: Spinous processes of T6 to T12, iliac crest, thoracolumbar fascia, and the inferior three ribs
- Insertion: Intertubercular sulcus of the humerus
- Innervation: Thoracodorsal nerve (C6, C7, C8)
Levator scapulae
- Function: Elevates the scapula
- Origin: Transverse processes of the C1 to C4 vertebrae
- Insertion: Medial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Rhomboid major
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of T2 to T5 vertebrae
- Insertion: Inferomedial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Rhomboid minor
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of C7 to T1 vertebrae
- Insertion: Medial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Serratus anterior
- Function: fixes the scapula into the thoracic wall, and aids in rotation and abduction of the arm (90 to 180 degrees)
- Origin: Surface of the upper eight ribs at the side of the chest
- Insertion: Along the entire anterior length of the medial border of the scapula
- Innervation: Long thoracic nerve (C5, C6, C7)
Pectoralis major
- Function:
- Clavicular head flexes and adducts arm
- Sternal head adducts and medially rotates the arm
- Accessory for inspiration
- Origin:
- Clavicular head: medial half clavicle
- Sternocostal head: Lateral manubrium and sternum, six upper costal cartilages and external oblique aponeurosis
- Insertion: Intertubercular groove of the proximal humerus on its lateral aspect
- Innervation: Medial and lateral pectoral nerves (C6, C7, C8)
Pectoralis minor
- Function: Depression of the shoulder, protraction of the scapula
- Origin: Third, fourth, fifth ribs close to their respective costal cartilages
- Insertion: Coracoid process
- Innervation: Medial pectoral nerve (C8, T1)
Subclavius
- Function: Depression and stabilization of the clavicle
- Origin: First rib medially
- Insertion: Middle of the clavicle, inferiorly
- Innervation: Nerve to subclavius (C5, C6)
Coracobrachialis
- Function: Flexion and adduction of the arm
- Origin: Coracoid process
- Insertion: Middle of the humerus, on its medial aspect
- Innervation: Musculocutaneous nerve (C5, C6, C7)
Biceps brachii
- Function: Resists dislocation of the shoulder, flexion of the forearm, supination of the forearm
- Origin:
- Short head: coracoid process
- Long head: supraglenoid tubercle of the scapula and superior labrum
- Insertion: Radial tuberosity of radius and forearm fascia (as bicipital aponeurosis)
- Innervation: Musculocutaneous nerve (C5, C6)
Triceps brachii
- Function: Resists dislocation of the shoulder, major extensor of the forearm
- Origin:
- Lateral head: above the radial groove of the humerus,
- Medial head: below the radial groove of the humerus
- Long head: infraglenoid tubercle of the scapula
- Insertion: Olecranon process of ulna and forearm fascia
- Innervation: Radial nerve (C6, C7, C8)
Physiologic Variants
The most common variants are related to the anterosuperior aspect of the shoulder joint, as well as variable development and shape of the bones within the shoulder girdle.[2]
Surgical Considerations
As it contains the most mobile joint in the body, the shoulder is very susceptible to injury. Surgical interventions may be required to repair or replace bones, joints, or tendons. Techniques used include arthroscopy, total arthroplasty, and shaving down bone in cases of impingement.
Clinical Significance
Rotator Cuff Injuries [3][4][5]
Shoulder pain affects approximately 18 million Americans a year, most of which are a result of rotator cuff tears. Tears can occur from a mix of trauma, overuse, or age-related degeneration and can be asymptomatic or cause severe pain and decreased mobility. Research has shown that smoking, hypercholesterolemia, and family history all predispose to tears. Even with small full-thickness tears, conservative, non-surgical treatment is the first line and may be effective. When it is not, or with larger full-thickness tears, surgical repair is a reliable fix. Rotator cuff tendonitis/impingement presents with pain during overhead activities and results from the tendon of the supraspinatus muscle being pinched down by the acromion in most cases, which can cause inflammation around the tendon and in the fluid-filled bursae surrounding it.
The price of being the most mobile joint in the body is that the glenohumeral joint lacks stability and is subject to dislocation. Anterior dislocations are the most common as they make up 97% of all dislocations. The typical cause by a blow to an abducted, externally rotated and extended extremity. Anterior dislocation may damage the axillary nerve, causing paralysis of the deltoid and decreased cutaneous sensation over the shoulder, as well as ligament tears and fractures. Patients usually recover functionality of the axillary nerve with a reduction of the humeral head back into the glenoid fossa. Posterior dislocations are less frequent but are associated with seizures. There is more risk of rotator cuff and ligament tears with posterior dislocations than anterior. Inferior dislocations are very rare and are the result of hyperabduction. They have the highest incidence of axillary nerve and artery damage.
Adhesive capsulitis [9]
Adhesive capsulitis also called frozen shoulder, occurs in 2 to 5% of the population, with most patients being females and over the age of 55. The thinking is that inflammation in the area of the shoulder capsule causes initial pain as well as capsular fibrosis and adhesions that lead to a decreased range of motion in all planes. There is a strong association of adhesive capsulitis with endocrine disorders like diabetes and hypothyroidism. Treatment is conservative, with most cases resolving spontaneously. Surgical intervention is reserved for refractory cases and involves releasing the fibrotic capsule.
Osteoarthritis [10]
Like other joints with extensive use, the shoulder joint is susceptible to wear and tear degeneration of the articular cartilage within the joint. Age, female gender, obesity, anatomical factors, muscle weakness, and joint injury are predisposing factors to the development of osteoarthritis. Bone-on-bone friction causes moderate to severe pain in patients. Treatment is usually conservative, with NSAIDs being the first-line choice. Refractory osteoarthritis may need intra-articular corticosteroid injections to decrease the inflammation. Surgical intervention in the form of arthroplasty is reserved for severe cases in which pharmacotherapy is not relieving symptoms.
Media
(Click Image to Enlarge)
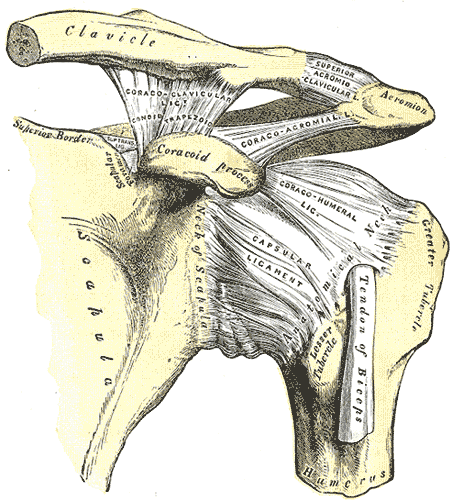
Left Shoulder Anatomy. This image shows the anatomic relationships between the clavicle, scapula, scapular neck, foramen, and superior border, coracoid process, acromion, greater and lesser humeral tubercles, humerus and anatomical neck, tendon of the biceps brachii long head, and the coracoclavicular (with the conoid and trapezoid), coracoacromial, superior acromioclavicular, coracohumeral, and capsular ligaments.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
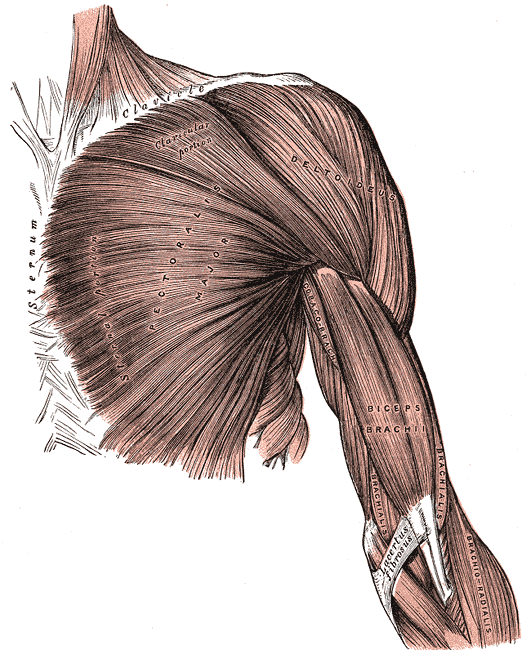
Superficial Muscles of the Chest and Shoulder. This illustration shows the pectoralis major, deltoid, coracobrachialis biceps brachii, brachialis, and brachioradialis. Other structures included in this image are the clavicle, sternum, and lacertus fibrosus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
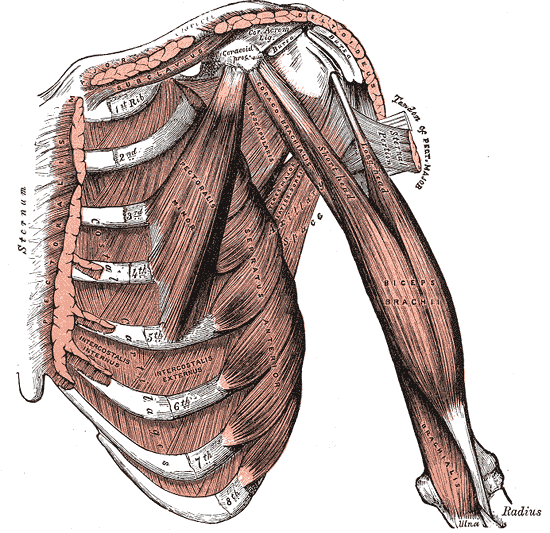
Internal Muscles of the Chest and Shoulder. The internal muscles of the chest and shoulder include the pectoralis, deltoid, subclavius, costal cartilages, ribs, pectoralis minor, serratus anterior, biceps brachii, coracobrachialis, and brachialis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
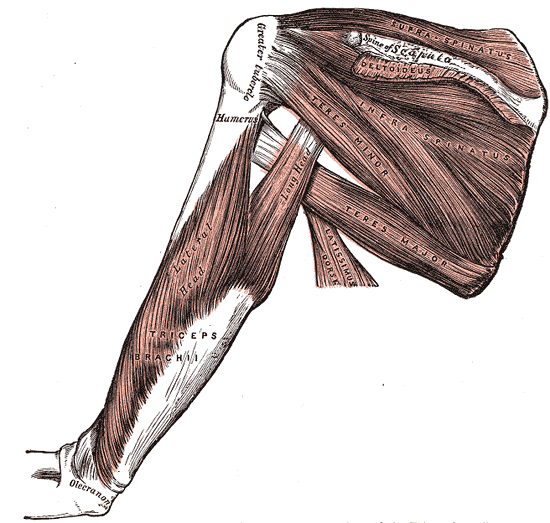
Muscles and Fascia of the Shoulder, Supraspinatus, Scapula, Humerus, Deltoid, Infraspinatus, Teres minor and major, Latissimus Dorsi, Triceps brachii,
Henry Vandyke Carter, Public domain, via Wikimedia Commons
References
Javed O, Maldonado KA, Ashmyan R. Anatomy, Shoulder and Upper Limb, Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 29494017]
Kadi R, Milants A, Shahabpour M. Shoulder Anatomy and Normal Variants. Journal of the Belgian Society of Radiology. 2017 Dec 16:101(Suppl 2):3. doi: 10.5334/jbr-btr.1467. Epub 2017 Dec 16 [PubMed PMID: 30498801]
Tashjian RZ. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clinics in sports medicine. 2012 Oct:31(4):589-604. doi: 10.1016/j.csm.2012.07.001. Epub 2012 Aug 30 [PubMed PMID: 23040548]
Schmidt CC, Jarrett CD, Brown BT. Management of rotator cuff tears. The Journal of hand surgery. 2015 Feb:40(2):399-408. doi: 10.1016/j.jhsa.2014.06.122. Epub 2015 Jan 1 [PubMed PMID: 25557775]
Maruvada S, Madrazo-Ibarra A, Varacallo M. Anatomy, Rotator Cuff. StatPearls. 2023 Jan:(): [PubMed PMID: 28722874]
Abrams R, Akbarnia H. Shoulder Dislocations Overview. StatPearls. 2023 Jan:(): [PubMed PMID: 29083735]
Avis D, Power D. Axillary nerve injury associated with glenohumeral dislocation: A review and algorithm for management. EFORT open reviews. 2018 Mar:3(3):70-77. doi: 10.1302/2058-5241.3.170003. Epub 2018 Mar 26 [PubMed PMID: 29657847]
Kammel KR, El Bitar Y, Leber EH. Posterior Shoulder Dislocations. StatPearls. 2023 Jan:(): [PubMed PMID: 28722948]
St Angelo JM, Fabiano SE. Adhesive Capsulitis. StatPearls. 2023 Jan:(): [PubMed PMID: 30422550]
Sen R, Hurley JA. Osteoarthritis. StatPearls. 2023 Jan:(): [PubMed PMID: 29493951]