Introduction
“Pilon,” the French word for pestle, was first used by Etienne Destot in 1911 as an analogy for the mechanical function of the distal tibia on the talus.[1] Fractures of the distal tibial plafond are also termed pilon fractures to describe the high energy axial compression force of the tibia as it acts as a pestle, driving vertically into the talus.[2][3][4] These fractures account for approximately 1% to 10% of the lower leg or tibial fractures and are often associated with severe bone comminution and soft tissue compromise.[5][6][7] Pilon fractures may also involve metaphyseal extension and can have associated fibular fractures.
The distal tibia has a quadrilateral cross-sectional shape and together with the fibula, ligaments, and capsule, forms the ankle mortise. This topography is designed to maximize the articular surface area with the dome of the talus and minimize the stress on the ankle joint.[5][6] The tibia and fibula are held together by the interosseous membrane, anterior inferior and posterior inferior tibiofibular ligaments. The vascular supply of the tibial plafond derives from branches of the anterior tibial, posterior tibial, and peroneal arteries.
The two most common classification systems used to describe pilon fractures are the Ruedi-Allgower classification and the AO/OTA classification. Type I Ruedi-Allgower fractures are defined as nondisplaced “cleavage fractures” of the tibial plafond.[4] Displacement is defined as greater than 2 mm of incongruity at the articular surface or mal-alignment greater than 10 degrees in any plane.[8] In Ruedi and Allgower’s initial publication, type-I fractures were associated with the highest rate of satisfactory reduction using closed methods.[4] Type-II fractures are defined as simple displacement without comminution of the articular surface, while type-III fractures are defined by substantial articular comminution often associated with metaphyseal impaction. Type-III fractures are the most frequent presentation, comprising approximately 25% to 71% of all pilon fractures.[4][7][8][9][10][11][12][13][14] In the AO/OTA classification for long bone fractures, pilon fractures are classified as extra-articular (43A), partial articular (43B), and intra-articular (43C), and further subclassified based on the degree of comminution. In addition to classifying the fracture type, consideration must be given to the extent of soft tissue damage using the Gustilo-Anderson classification for open fractures or the Tscherne classification for closed fractures.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Pilon fractures most often result from high-energy mechanisms, such as motor vehicle accidents and falls from a height that causes direct axial compression and articular impaction of the tibial plafond.[8][10][11][12][14][15] Low-energy mechanisms may also occur but are much less common. In Ruedi and Allgower’s original series,[3] the majority of their patients sustained pilon fractures from skiing injuries. These were felt to occur from rotational forces on the distal tibia, resulting in less comminution, fracture displacement, and soft tissue damage compared to higher energy mechanisms. Older females with osteoporotic bone are also at high risk of low-energy pilon fractures.[5]
Epidemiology
Pilon fractures occur more frequently in males (57% to 65%) compared to females.[5] The age distribution of pilon fractures follows a bimodal pattern with peak frequency at 25 and 50 years of age.[5]
Pathophysiology
The mechanism and degree of injury involved dictate the fracture pattern and the treatment approach to pilon fractures. The impact from an axial compression mechanism drives the articular surface proximally into the metaphysis, with associated metaphyseal comminution. Associated fibular fractures are commonly present.[5] Low-energy torsional injuries lead to less articular comminution and larger fracture fragments that remain in continuity with subchondral bone.[13][14] Several studies have also demonstrated the morphology of three major fragments (anterior, posterior, and medial) in a Y-shaped pattern on axial imaging.[6][13][14] Ligamentous attachments to the distal tibia contribute to this predictable fracture pattern. The anterior or Chaput fragment is attached to the anterior inferior tibiofibular ligament (AITFL); the posterior or Volkmann fragment is attached to the posterior inferior tibiofibular ligament (PITFL); the medial malleolar fragment is attached to the deltoid ligament. Fragments that maintain their normal alignment or fractures without this typical Y-shaped pattern may be indicative of ligament rupture.
Open fractures comprise approximately 20% of pilon fractures.[5] High-energy injuries are typically also associated with severe soft tissue destruction, which can present a major risk factor for wound complications and deep infections.[13][14] The extent of soft tissue injury, however, does not always correlate to the degree of fracture comminution.[16]
History and Physical
Patients who sustain high-energy pilon fractures may also present with multi-system trauma and other life-threatening injuries. Initial evaluation and resuscitation should follow the Advanced Trauma Life Support (ATLS) guidelines and begin with the ABCs of a primary survey. Once the patient is stabilized, a thorough history and secondary survey are necessary to identify the injury mechanism and other potential injuries. With pilon fractures, careful inspection of the patient’s lower extremities can further provide clues as to the extent of soft tissue insult. High-energy injuries may present with obvious deformities and open wounds; however, lower energy torsional injuries may be more difficult to detect. Inability to bear weight, considerable bruising, swelling, and skin blistering about the ankle should raise clinical suspicion of acute fracture with overlying soft tissue damage. Limb-threatening injuries often present as open fractures with severe soft tissue de-gloving or as crush injuries. The following are the grades as defined by the Tscherne classification for soft tissue injury in closed fractures:
- Grade 0 represents minimal tissue damage associated with simple fracture pattern
- Grade 1 involves superficial abrasion or contusion
- Grade 2 involves deep abrasion of skin or muscle contusion
- Grade 3 presents with extensive skin and muscle damage or crush injury, subcutaneous avulsion, and/or compartment syndrome[17]
The Gustillo-Anderson system is used to classify open pilon fractures.[18]
A detailed neurovascular examination, as well as evaluation of the lower leg compartments for compartment syndrome, is critical in the assessment of pilon fractures. Detailed neurovascular examination involves checking the posterior tibial and dorsalis pedis pulses, evaluating sensation in the tibial, superficial peroneal, deep peroneal, sural, and saphenous nerve distributions, and assessing motor function in active ankle dorsiflexion and plantarflexion as well as flexion and extension of the great toe. Motor function is expectedly limited due to pain.
Evaluation
Radiographic evaluation should begin with anteroposterior, lateral, and mortise x-rays views of the ankle. Full-length tibia x-rays should also be obtained to rule out associated fractures and assess the length, alignment, and rotation of the tibia. In patients who had a fall from a height, radiographs of the spine, pelvis, foot and contralateral lower limb may be indicated to evaluate for associated injuries, particularly to the vertebral column or calcaneus. Appropriate laboratory studies, such as metabolic panel, complete blood count, coagulation profile, urinalysis, and toxicology screen may be indicated in the poly-trauma patient.
Definitive surgical planning for pilon fractures often requires advanced imaging with computed tomography (CT). The original Ruedi-Allgower classification was based on plain radiographs.[4] Its simplicity and ease of use have made it the most well-known system for characterizing pilon fractures but has also made it problematic to differentiate more complex patterns and intra-articular fracture lines.[19] The advent of the CT and 3-dimensional reconstruction has improved the ability to discern complex fracture patterns. In a study by Tornetta et al.,[20] the authors reviewed 22 pilon fractures, in which CT scans provided additional information and altered the operative plan in 82% and 64% of cases, respectively. The timing of CT scan is recommended after the fracture has been adequately reduced and stabilized, most frequently with an external fixation device.
Treatment / Management
There are few relative contraindications to operative fixation of pilon fractures. Patients with non-displaced fractures without articular involvement may be treated with cast immobilization and weight-bearing restrictions. A major disadvantage to closed treatment in a cast is difficulty in assessing soft tissue healing. Patients who are non-ambulatory at baseline or not medically fit for surgery may also be treated conservatively. Other contraindications are decided on a case-by-case basis. Early descriptions of pilon fractures demonstrated difficulty in achieving fracture union and high complication rates, leaving patients with persistent pain, deficits in range of motion, and disability. Historically, many surgeons considered pilon fractures “not amenable to surgery.”[4] Nonoperative treatment, however, often resulted in secondary joint displacement and poor outcomes. Ruedi and Allgower first published their surgical technique and early results for the management of pilon fractures in 1968, providing a pivotal shift in the treatment paradigm.[21] They proposed a 4-stage surgical approach to optimize anatomic reduction and stabilization of pilon fractures.[3][4] The first step requires the restoration of fibular length to re-establish the lateral column, which aids in the reduction of the tibial plafond. The second step calls for anatomic restoration of the articular surface of the distal tibia, which often resembles a jigsaw puzzle given the severe comminution. Ruedi and Allgower recommended using the talus as a template to reconstruct the tibia. The third step involves the use of autologous bone graft to fill any metaphyseal bone defects. The purpose of this is to prevent collapse, or subsidence, of the distal articular surface. Lastly, a buttress plate is placed on the distal aspect of the tibia.
Historically, the high rates of wound complications and infections were associated with early open fixation through compromised soft tissue, highlighting the importance of careful soft tissue evaluation and handling, especially in severe pilon fractures. Consequently, the treatment algorithm shifted to a staged procedure, beginning with ankle-spanning external fixation to restore length and alignment of the pilon fracture, followed by definitive internal fixation once the soft tissue swelling subsides.[22] Excessive traction across the ankle joint during external fixation placement should be avoided to prevent traction injury to the nerves. CT imaging should be obtained after external fixation to characterize the articular surface fracture patterns. Studies have demonstrated lower incidence of wound complications and deep infections with this staged protocol compared to early open reduction internal fixation (ORIF).[8][15](A1)
Advanced imaging can help guide the surgeon on the incisional approach and the selection and positioning of the implants. Various surgical approaches to the ankle may be utilized depending on the location of the fracture fragments (anteromedial, direct anterior, anterolateral, posterolateral, posteromedial and direct medial). Most pilon fractures are addressed through an anterior or anterolateral approach. Posteromedial and posterolateral approaches may be indicated if fixation of posterior fragments is warranted. If multiple incisions are needed, the width of the skin bridge should be maximized (typically greater than 7 cm) with continued vigilance in respecting the soft tissue envelope, although skin bridges less than 7 cm may be safe in certain patient.[23] Postoperatively, the patient is advised to elevate the operative extremity to alleviate swelling. They are restricted from weight-bearing typically until 6 to 12 weeks after surgery.[24]
Prognosis
Despite advances in radiographic imaging, surgical instrumentation, and our understanding of the importance of soft tissue handling, pilon fractures remain challenging to treat. Clinical outcomes correlate with severity of the fracture pattern and the quality of reduction.[11][12][25] Quality of life outcomes, including both the physical and mental component scores of the Short Form-36 Health Survey (SF36), are also significantly poorer compared to an age and gender-matched general population in a study based in Spain.[26] Multivariate analysis demonstrated lower physical component summary (PCS) scores in AO/OTA C-type fractures and patients with lower education level. Lower mental component summary (MCS) scores were found in patients older than 55 years. Divorced status, inadequate reduction (greater than 2 mm of joint incongruity), and asymmetric ankle range of motion were significant risk factors for decreased scores in both the PCS and MCS.[26] Complications after surgical fixation include wound slough or dehiscence, infection, varus malunion, nonunion, joint stiffness, and post-traumatic arthritis.[27] In one study, only 28% of patients treated for pilon fractures reported walking without pain at final follow-up.[5] Patients who develop symptomatic post-traumatic arthritis can be treated initially with activity modification and non-steroidal anti-inflammatory drugs (NSAIDs). Failed conservative management and persistent pain may require ankle arthrodesis as a salvage operation. Patients who sustain pilon fractures should be adequately counseled on outcomes and expectations after surgical fixation.
Enhancing Healthcare Team Outcomes
A team approach involving the emergency nurse, orthopedic nurse, emergency clinician, and the specialist will result in the best care and positive results for the patient. [Level V]
Media
(Click Image to Enlarge)

Pilon Fracture 3D CT scan of a pilon fracture. Note articular impaction and comminution of the tibial plafond. Contributed by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Distal Tibia Pilon fracture Contributed by Andrew Hadeed, DO
(Click Image to Enlarge)

Transverse CT of a pilon fracture demonstrating a comminuted anterolateral fragment (Chaput). Contributed by T. David Luo, MD
(Click Image to Enlarge)
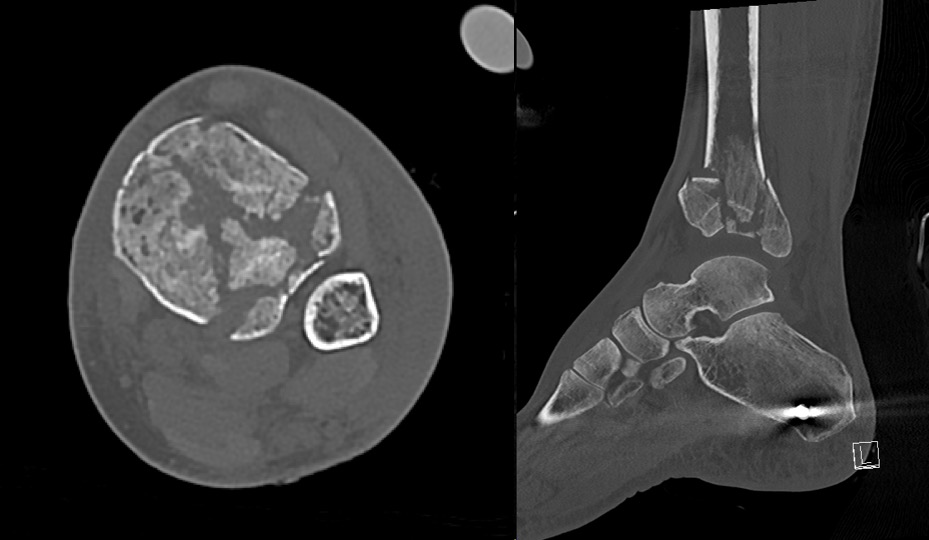
Axial and sagittal CT slices of a pilon fracture after external fixation placement Contributed by T. David Luo, MD
(Click Image to Enlarge)

AP and lateral XR of left pilon fracture Contributed by T. David Luo, MD
References
Michelson J, Moskovitz P, Labropoulos P. The nomenclature for intra-articular vertical impact fractures of the tibial plafond: pilon versus pylon. Foot & ankle international. 2004 Mar:25(3):149-50 [PubMed PMID: 15006336]
Jacob N, Amin A, Giotakis N, Narayan B, Nayagam S, Trompeter AJ. Management of high-energy tibial pilon fractures. Strategies in trauma and limb reconstruction. 2015 Nov:10(3):137-47. doi: 10.1007/s11751-015-0231-5. Epub 2015 Sep 25 [PubMed PMID: 26407690]
Rüedi T. Fractures of the lower end of the tibia into the ankle joint: results 9 years after open reduction and internal fixation. Injury. 1973 Nov:5(2):130-4 [PubMed PMID: 4774764]
Rüedi TP, Allgöwer M. The operative treatment of intra-articular fractures of the lower end of the tibia. Clinical orthopaedics and related research. 1979 Jan-Feb:(138):105-10 [PubMed PMID: 376196]
Mauffrey C, Vasario G, Battiston B, Lewis C, Beazley J, Seligson D. Tibial pilon fractures: a review of incidence, diagnosis, treatment, and complications. Acta orthopaedica Belgica. 2011 Aug:77(4):432-40 [PubMed PMID: 21954749]
Cole PA, Mehrle RK, Bhandari M, Zlowodzki M. The pilon map: fracture lines and comminution zones in OTA/AO type 43C3 pilon fractures. Journal of orthopaedic trauma. 2013 Jul:27(7):e152-6. doi: 10.1097/BOT.0b013e318288a7e9. Epub [PubMed PMID: 23360909]
Ballal A, Rai HR, Shetty SM, Mathias LJ, Shetty V, Shetty A. A Prospective Study on Functional Outcome of Internal Fixation of Tibial Pilon Fractures with Locking Plate using Minimally Invasive Plate Osteosynthesis Technique. Journal of clinical and diagnostic research : JCDR. 2016 Jan:10(1):RC01-4. doi: 10.7860/JCDR/2016/15284.7013. Epub 2016 Jan 1 [PubMed PMID: 26894132]
Wyrsch B, McFerran MA, McAndrew M, Limbird TJ, Harper MC, Johnson KD, Schwartz HS. Operative treatment of fractures of the tibial plafond. A randomized, prospective study. The Journal of bone and joint surgery. American volume. 1996 Nov:78(11):1646-57 [PubMed PMID: 8934478]
Level 1 (high-level) evidenceAnglen JO. Early outcome of hybrid external fixation for fracture of the distal tibia. Journal of orthopaedic trauma. 1999 Feb:13(2):92-7 [PubMed PMID: 10052782]
Level 2 (mid-level) evidenceChen SH, Wu PH, Lee YS. Long-term results of pilon fractures. Archives of orthopaedic and trauma surgery. 2007 Jan:127(1):55-60 [PubMed PMID: 17004076]
Korkmaz A, Ciftdemir M, Ozcan M, Copuroğlu C, Sarıdoğan K. The analysis of the variables, affecting outcome in surgically treated tibia pilon fractured patients. Injury. 2013 Oct:44(10):1270-4. doi: 10.1016/j.injury.2013.06.016. Epub 2013 Jul 18 [PubMed PMID: 23871428]
Level 2 (mid-level) evidenceTeeny SM, Wiss DA. Open reduction and internal fixation of tibial plafond fractures. Variables contributing to poor results and complications. Clinical orthopaedics and related research. 1993 Jul:(292):108-17 [PubMed PMID: 8519097]
Level 2 (mid-level) evidenceTopliss CJ, Jackson M, Atkins RM. Anatomy of pilon fractures of the distal tibia. The Journal of bone and joint surgery. British volume. 2005 May:87(5):692-7 [PubMed PMID: 15855374]
Schulz AP, Fuchs S, Simon L, Seide K, Paech A, Queitsch C. Severe Fracture of the Tibial Pilon: Results with a Multidirectional Self-locking Osteosynthesis Plate Utilizing a Two-stage Procedure. European journal of trauma and emergency surgery : official publication of the European Trauma Society. 2008 Aug:34(4):391-6. doi: 10.1007/s00068-007-2209-6. Epub 2007 Nov 14 [PubMed PMID: 26815817]
Sirkin M, Sanders R, DiPasquale T, Herscovici D Jr. A staged protocol for soft tissue management in the treatment of complex pilon fractures. Journal of orthopaedic trauma. 1999 Feb:13(2):78-84 [PubMed PMID: 10052780]
Level 2 (mid-level) evidenceAnderson DD, Mosqueda T, Thomas T, Hermanson EL, Brown TD, Marsh JL. Quantifying tibial plafond fracture severity: absorbed energy and fragment displacement agree with clinical rank ordering. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2008 Aug:26(8):1046-52. doi: 10.1002/jor.20550. Epub [PubMed PMID: 18327811]
Ibrahim DA, Swenson A, Sassoon A, Fernando ND. Classifications In Brief: The Tscherne Classification of Soft Tissue Injury. Clinical orthopaedics and related research. 2017 Feb:475(2):560-564. doi: 10.1007/s11999-016-4980-3. Epub 2016 Jul 14 [PubMed PMID: 27417853]
Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. The Journal of trauma. 1984 Aug:24(8):742-6 [PubMed PMID: 6471139]
Luo TD, Eady JM, Aneja A, Miller AN. Classifications in Brief: Rüedi-Allgöwer Classification of Tibial Plafond Fractures. Clinical orthopaedics and related research. 2017 Jul:475(7):1923-1928. doi: 10.1007/s11999-016-5219-z. Epub 2017 Jan 4 [PubMed PMID: 28054323]
Tornetta P 3rd, Gorup J. Axial computed tomography of pilon fractures. Clinical orthopaedics and related research. 1996 Feb:(323):273-6 [PubMed PMID: 8625591]
Rüedi T, Matter P, Allgöwer M. [Intra-articular fractures of the distal tibial end]. Helvetica chirurgica acta. 1968 Nov:35(5):556-82 [PubMed PMID: 4974693]
Helfet DL, Koval K, Pappas J, Sanders RW, DiPasquale T. Intraarticular "pilon" fracture of the tibia. Clinical orthopaedics and related research. 1994 Jan:(298):221-8 [PubMed PMID: 8118979]
Howard JL, Agel J, Barei DP, Benirschke SK, Nork SE. A prospective study evaluating incision placement and wound healing for tibial plafond fractures. Journal of orthopaedic trauma. 2008 May-Jun:22(5):299-305; discussion 305-6. doi: 10.1097/BOT.0b013e318172c811. Epub [PubMed PMID: 18448981]
Kubiak EN, Beebe MJ, North K, Hitchcock R, Potter MQ. Early weight bearing after lower extremity fractures in adults. The Journal of the American Academy of Orthopaedic Surgeons. 2013 Dec:21(12):727-38. doi: 10.5435/JAAOS-21-12-727. Epub [PubMed PMID: 24292929]
Ovadia DN, Beals RK. Fractures of the tibial plafond. The Journal of bone and joint surgery. American volume. 1986 Apr:68(4):543-51 [PubMed PMID: 3957978]
Level 2 (mid-level) evidenceCutillas-Ybarra MB, Lizaur-Utrilla A, Lopez-Prats FA. Prognostic factors of health-related quality of life in patients after tibial plafond fracture. A pilot study. Injury. 2015 Nov:46(11):2253-7. doi: 10.1016/j.injury.2015.06.025. Epub 2015 Jun 18 [PubMed PMID: 26115581]
Level 2 (mid-level) evidenceThordarson DB. Complications after treatment of tibial pilon fractures: prevention and management strategies. The Journal of the American Academy of Orthopaedic Surgeons. 2000 Jul-Aug:8(4):253-65 [PubMed PMID: 10951114]