Introduction
Piriformis syndrome is an infrequent cause of entrapment neuropathy. A diagnosis of exclusion, piriformis syndrome occurs secondary compression or entrapment of the sciatic nerve by the piriformis muscle.
Historically, the exact definition of this syndrome has varied in the literature. In 1928, Yeoman was the first to describe pain in the sciatic nerve distribution secondary to piriformis syndrome. In 1947, Robinson coined the term piriformis syndrome and proposed six cardinal features which include:
- History of trauma to the sacroiliac and gluteal region
- Pain in the sacroiliac joint
- Greater sciatic notch and piriformis muscle extending down the leg and causing difficulty walking
- Acute exacerbations brought on by stooping or lifting and relieved by traction on the affected leg
- The presence of a palpable tender sausage-shaped mass over the piriformis muscle
- Positive Lasegue sign and gluteal atrophy.
Since this historical report, many of Robinson's proposed diagnostic criteria have since been disputed or refuted. Contemporary dogma is accepting of a much broader clinical definition accompanying a diagnosis of piriformis syndrome, defined as a syndrome consisting of isolated sciatic pain usually limited to the buttock with radiation down the thigh [1].
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Symptoms associated with piriformis syndrome occur from compression of the sciatic nerve by the piriformis muscle. The cause of compression and subsequent nerve irritation is variable. It can result from overuse or repetitive trauma where overtraining or sitting on hard surfaces can cause direct or indirect injury to the muscle or nerve.
Athletes and weightlifters are prone to intermittent symptom exacerbation secondary to increased training requirements and activities. In these cases, the piriformis muscle itself becomes hypertrophied and causes direct pressure on the nerve.
Acute trauma like blunt forces can also result in hematoma formation and subsequent scarring between the sciatic nerve and the short external rotators (piriformis, superior and inferior gemelli, quadratus femoris). Anomalous anatomic relationships of the sciatic nerve with the piriformis muscle have also been implicated where the nerve is more susceptible to compression because of the variant anatomy. Beaton and Anson originally described 6 different anatomic relationships between the sciatic nerve and piriformis muscle. In >80% of the population, the sciatic nerve passes deep and exits inferiorly to the inferior edge of the muscle belly/tendon [2]. Notable variations include early (proximal) divisions of the sciatic nerve into its tibial and common peroneal components, with these branches passing through and below the piriformis muscle or above and below the muscle. These anomalous sciatic nerve variants are all a potential cause of piriformis syndrome [3].
There have also been numerous case reports that show that other conditions have been associated with piriformis syndrome which includes pyomyositis, aberrant fibrous bands, myositis ossificans, and pseudoaneurysms.
Indications
Piriformis syndrome may be responsible for 0.3% to 6% of all cases of low back pain and/or sciatica. With an estimated amount of new cases of low back pain and sciatica at 40 million annually, the incidence of piriformis syndrome would be roughly 2.4 million per year. In the majority of cases, piriformis syndrome occurs in middle-aged patients with a reported ratio of male to female patients being affected 1:6.
Contraindications
Two components contribute to the clinical presentation of piriformis syndrome: somatic and neuropathic. The somatic component is a myofascial pain component of the syndrome secondary to any of the surrounding muscles/fascia (i.e. any of the short external rotators of the hip). The neuropathic component refers to the compression or irritation of the sciatic nerve as it courses through above, near, or through, the piriformis muscle itself.
Patients may present acutely in cases of post-traumatic piriformis syndrome or insidiously as in cases of overuse or myofascial pain. Patients will report having gluteal pain with possible associated paresthesias in the back, groin, perineum, buttocks, hip, back of the thigh, calf, foot, and rectum. There is also intense and worsened pain with sitting or squatting.
Preparation
The initial evaluation should start with a lumbar spine examination. The examination should take into account the patient's gait, posture, and alignment as well as any leg length discrepancies. Also, the practitioner should examine the patient's hips, pelvis, and sacroiliac joint, noting sensory, motor, and deep tendon reflexes.
In piriformis syndrome, sensory, motor, and deep tendon reflexes are normal. The piriformis should be palpated as well just posterior to the hip joint and in the area of the greater sciatic notch. Straight leg raise may also be positive although there is variable sensitivity and specificity for this provocative maneuver.
There are individual tests that stretch the piriformis and can be used to help aid in the diagnosis of exclusion. One of these is the Freiberg sign, which is performed by putting the hip in extension and internal rotation and having the patient externally rotate against resistance. The positive exam will reproduce pain around the piriformis. This test will have positive results in up to 63% of patients. Another individual test called the Pace sign is performed by resisting abduction and external rotation of the hip while the patient is in a seated position. Pace sign occurs in 30% to 74% in piriformis syndrome. FAIR test or also known as the piriformis stretch may elicit pain. Beatty sign has also been described and is accomplished by elevating the flexed leg on the irritated side while the patient lies on the asymptomatic side. Pain and reproduction of the symptoms are positive test results.
Technique or Treatment
No definitive diagnostic criteria have been validated and established for piriformis syndrome. It remains a diagnosis of exclusion, but many of the following exam findings can aid the clinician in honing in on this diagnosis:
- Unilateral or bilateral buttock pain with fluctuating periods of pain throughout the day
- No lower back pain,
- No pain upon palpation of axial spine
- Negative results for straight leg raise
- Prolonged sitting triggering gluteal pain or sciatica
- Fluctuating sciatica through the course of the day
- Buttock pain near the projection of the piriformis reproduced by FAIR or Freiberg sign or Beatty sign, or palpitations
- The absence of perineal irradiation
- Sciatica reproduced by FAIR, Freiberg sign, or Beatty sign.
Standard radiographs of the pelvis and hip should be done to rule out underlying hip pathology. MRI of the lumbar spine is also recommended to evaluate for discogenic causes of lumbar radiculopathy and to rule out other sources of compression (e.g. soft tissue tumors or masses). MRI can also evaluate for spinal stenosis, herniated disks, facet arthrosis, SI joint pathology, occult pelvic fractures, and any surrounding tendinopathies or bursitides.
EMG is often normal in patients with acute piriformis syndrome presentations, however, chronically, EMG/NCS can be useful in identifying neuropathic changes and abnormal results in muscles innervated by the sciatic nerve [4].
Solution (injectable):
- Corticosteroids: 40-mg of Depo-Medrol or Kenalog
- Local anesthetics: 3-5-ml of local anesthetic such as lidocaine or bupivacaine
- It is also done with botulinum toxin for longer relief than steroids and local anesthetic.
Patient Position: Prone
Fluoroscopy starting position:
- An A-P view is adjusted so that the inferior part of the sacroiliac joint is in the middle of the screen.
Piriformis Muscle Injection with Fluoroscopic Guidance
- 18-gauge 1.5″ needle tip is placed on the cleaned skin over the inferior SI joint.
- Create a skin wheal and then anesthetize the deeper subcutaneous skin with 1% lidocaine and a 27-gauge 1.25-inch needle.
- A 22-gauge 3.5″ or 5″ Quincke needle is used to contact the very tip of the inferior sacroiliac joint. As the procedure is performed, note the approximate needle depth.
- After injection, the needle is withdrawn and redirected to a target site 1-cm inferior, 1-cm lateral, and 1-cm deeper than the SI joint.
Caution: Never inject if the patient feels a sharp pain shooting down their leg as the needle tip may be inside the sciatic nerve. The needle should be repositioned and then retry.
Complications
Nonoperative
Treatment for piriformis syndrome begins with nonoperative modalities including:
- Oral analgesics (e.g. NSAIDs, muscle relaxants, and gabapentin)
- Physical therapy:
- Regimens include nerve stretches, isometric exercises, gluteal muscle strengthening
- Injections
- Diagnostic and therapeutic modalities
- Agents used include cortisone, local anesthetic, or botulinum toxin
- A recent study reported positive outcomes in patients managed with physical therapy and Botulinum toxin injection
Surgical Treatment
- Surgery is considered in refractory cases after exhausting nonoperative modalities
- A 2005 study reported surgical outcomes in 64 patients managed with surgical intervention for refractory symptoms: [5]
- 82% reported initial improvement
- 76% had long-term positive outcomes
- 92% of those managed with surgery returned to work or presurgical baseline activity levels within 2 weeks of the surgery
Clinical Significance
Piriformis syndrome is an infrequent cause of entrapment neuropathy. Significant pain relief may be obtained by injection of the piriformis muscle.
Enhancing Healthcare Team Outcomes
An interprofessional team involving a doctor and nurse will result in the best possible outcomes.
Media
(Click Image to Enlarge)
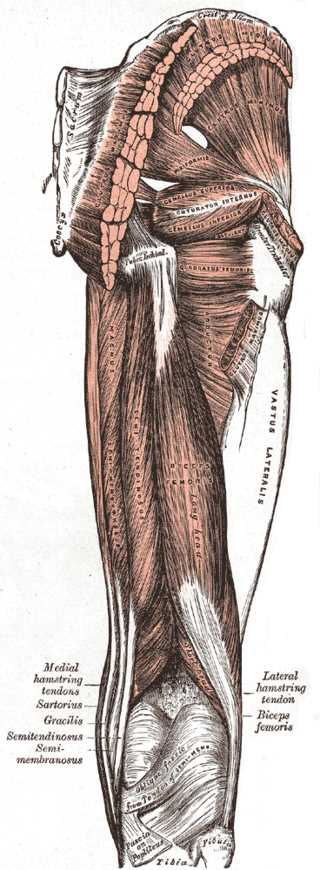
Muscles of the Hip and Thigh. The gluteal muscles include the gluteus maximus, gluteus medius, and gluteus minimus. Hip muscles include the piriformis, gemellus superior, gemellus inferior, and obturator internus. Thigh muscles include the adductor magnus, vastus lateralis, biceps femoris, semitendinosus, hamstring tendons, and gracilis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
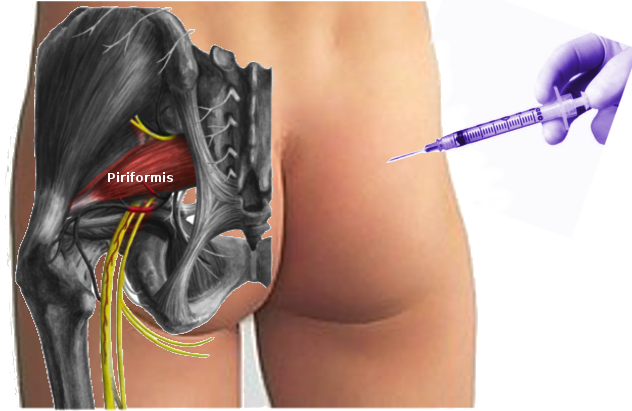
Piriformis injection Image courtesy S Bhimji MD
References
McCrory P, Bell S. Nerve entrapment syndromes as a cause of pain in the hip, groin and buttock. Sports medicine (Auckland, N.Z.). 1999 Apr:27(4):261-74 [PubMed PMID: 10367335]
Cassidy L, Walters A, Bubb K, Shoja MM, Tubbs RS, Loukas M. Piriformis syndrome: implications of anatomical variations, diagnostic techniques, and treatment options. Surgical and radiologic anatomy : SRA. 2012 Aug:34(6):479-86. doi: 10.1007/s00276-012-0940-0. Epub 2012 Feb 12 [PubMed PMID: 22327640]
Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequence: a review. Clinical anatomy (New York, N.Y.). 2010 Jan:23(1):8-17. doi: 10.1002/ca.20893. Epub [PubMed PMID: 19998490]
Level 1 (high-level) evidenceKraus E,Tenforde AS,Beaulieu CF,Ratliff J,Fredericson M, Piriformis Syndrome With Variant Sciatic Nerve Anatomy: A Case Report. PM [PubMed PMID: 26377629]
Level 3 (low-level) evidenceFiller AG, Haynes J, Jordan SE, Prager J, Villablanca JP, Farahani K, McBride DQ, Tsuruda JS, Morisoli B, Batzdorf U, Johnson JP. Sciatica of nondisc origin and piriformis syndrome: diagnosis by magnetic resonance neurography and interventional magnetic resonance imaging with outcome study of resulting treatment. Journal of neurosurgery. Spine. 2005 Feb:2(2):99-115 [PubMed PMID: 15739520]