Introduction
Poland syndrome consists of anatomic anomalies that include the absence of the sternocostal head of the pectoralis major muscle with other varied manifestations that include hypoplasia or absence of the pectoralis minor muscle as well as digital anomalies such as syndactyly.[1] Other anomalies include the absence or hypoplasia of the ipsilateral breast, excavatum deformities, and rib aplasia.[1] Defects are overwhelmingly unilateral and more commonly affect the right side.[2] Bilateral manifestations, although exceedingly rare, have also been described.[3] Many variations of the syndrome have been described, from mild hypoplasia of the pectoralis major musculature to severe hypoplasia of the thoracic wall.[4] Upper limb defects also vary from mild syndactyly to severe brachysyndactyly.[4][1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of Poland syndrome is not well understood and is thought to arise from abnormalities relating to the subclavian arteries and branch vessels during embryogenesis, reducing perfusion to the affected ipsilateral side of the chest wall.[5] Findings of vascular hypoplasia of the subclavian and branch vessels support this etiology, suggesting hypoperfusion of the developing limb bud during embryogenesis as the cause of Poland syndrome.[5] A teratogenic etiology has also been suggested because research shows an association with maternal smoking and cocaine use.[6][7] A history of misoprostol administration has been implicated.[8]
Epidemiology
Poland syndrome affects about 1 in 36,000 to 50,000 newborns, with males more likely to be symptomatic than females.[9] Furthermore, right-sided predominance occurs more frequently in men than women.[10] Cases are usually sporadic, with rare familial cases described in the literature.[11] Given the likelihood that Poland syndrome is often underdiagnosed and under-reported, the exact incidence is not definitively known, and incidence rates are usually estimated.[12]
History and Physical
Patients with Poland syndrome usually present for cosmetic and aesthetic complaints and are usually asymptomatic.[13] In pediatric patients and cases with more severe deformities, a more thorough history and physical examination are warranted. Patient history of cardiopulmonary complaints, although rare, can be important given the association of dextroposition and lung herniation with Poland syndrome.[10][14]
The physical evaluation for Poland syndrome includes an assessment of the anterior chest wall and associated anatomic limb abnormalities.[15][16] Evaluation of the anterior chest wall includes palpation to assess the asymmetry of the chest wall musculature and the osseous and cartilaginous deformities of the rib cage.[17] Evaluation for absence or hypoplasia of the costosternal pectoralis major muscle and the pectoralis minor muscle can usually be diagnosed with visual inspection and palpation.[18] Overlying soft tissues of the chest wall also tend to be thinner than normal.[1] Nipple absence or hypoplasia is frequently seen, and regional alopecia of the anterior chest wall and axilla can often be appreciated.[19] Breast asymmetry and hypoplasia, including a higher position of the breast of the affected side, can be seen in female patients.[20] Physical examination to evaluate the muscular caliber of the serratus, latissimus dorsi, and trapezius should be performed, as hypoplasia of these muscles can also be present.[21] Evaluation of the latissimus dorsi is important, especially in the setting of a planned surgical intervention.[21] A cardiopulmonary examination to evaluate for dextroposition, especially in the setting of left-sided Poland syndrome, should also be performed.[22]
Visual inspection and the physical examination of the ipsilateral limb are important because those limb anomalies are present in most cases, specifically syndactyly; hypoplastic metacarpals and phalangeal abnormalities of the index, middle, and ring fingers are most commonly affected.[23] In a pediatric patient, the association with Klippel-Feil and Mobius syndromes warrants a physical examination to evaluate for other manifestations, including abnormalities of the cervical spine and craniofacial abnormalities should be performed.[24][25]
Evaluation
Prenatal sonographic evaluation can demonstrate unilateral limb defects and unilateral chest wall asymmetry and should prompt evaluation for other associated anatomic defects.[26] In an adult patient, although physical examination is usually sufficient in the diagnosis of Poland syndrome, further evaluation with CT can be performed, especially in the setting of surgical planning or further evaluation for associated cardiopulmonary abnormalities, including lung herniation.[27] On mammograms, hypoplasia of the unilateral breast and hypoplasia of the pectoralis major are often appreciated.[28] Chest radiograph findings of a unilateral hyperlucent thorax are classically seen. Ultrasound of the chest wall can also be used to evaluate for defects of the pectoralis major and minor musculature.[29]
Treatment / Management
Surgical intervention, although rarely necessary, can be indicated for reasons including paradoxical movement of the chest wall, hypoplasia or aplasia of the female breast, and cosmetic indication for men and women with chest wall asymmetry.[30] Chest wall reconstruction in the setting of severe rib hypoplasia and aplasia can also serve as an operative indication.[30] The operative course varies and depends on the degree of deformity as well as the patient’s age and gender.[31] Usual operative strategies include a muscle flap as well as breast augmentation in women.[23] Bone grafts can be used in the setting of sternal and rib defects.[30] Given that the ipsilateral latissimus dorsi muscle can potentially be hypoplastic in a patient with Poland syndrome, the contralateral latissimus dorsi muscle would serve as the next viable option for a muscle flap procedure.[32] Syndactyly release can usually be performed in a pediatric patient without significant complications and can be performed with or without a skin graft.[33] Physical therapy may be helpful in pediatric patients to assist them to crawl and adapt to their deformities. Physical and occupational therapy are appropriate after surgical intervention.(B2)
Differential Diagnosis
Differential diagnosis of Poland syndrome in female patients includes normal breast asymmetry.[34] Although not usually necessary, further evaluation with imaging to include CT can help differentiate breast asymmetry secondary to Poland syndrome by evaluating the anatomy of the pectoralis major muscle.
An incidentally noted absent pectoralis muscle on CT scan could also be secondary to a surgically absent pectoralis major muscle.[35] In the setting of an incidentally noted radiograph finding of a unilateral hyperlucent hemithorax, the differential diagnosis includes airway obstruction, Swyer-James syndrome, a mastectomy, a unilateral large bullae, and pneumothorax.[36]
Complications
The majority of patients with Poland syndrome are asymptomatic and have few functional manifestations.[37][38] Prognosis usually depends on the degree of surgical intervention performed and varies depending on the severity of the syndrome. Complications that have been described in the literature usually are not different from similar procedures done for other indications.[39]
Enhancing Healthcare Team Outcomes
In the setting of asymptomatic cases, a primary care physician and a radiologist are often the sole members of the healthcare team involved in diagnosing and educating the patient on this presenting complaint. In the setting of planned surgical intervention, a primary care physician, often in coordination with a surgeon, is involved in assessing the patient's health status before surgery.[40] A radiologist can potentially play a role in assisting a surgeon on the degree of hypoplasia and absence of the pectoralis muscles as well as the degree of hypoplasia of the latissimus dorsi; this often can help guide surgical approach based on the degree of severity.[41] In the setting of severe cases of aplasia of the chest wall, a coordinated approach between a pulmonologist, a radiologist, and a cardiothoracic surgeon is important in guiding reconstruction as well as post-surgical follow-up. Physical and occupational therapists are often involved.
Media
(Click Image to Enlarge)
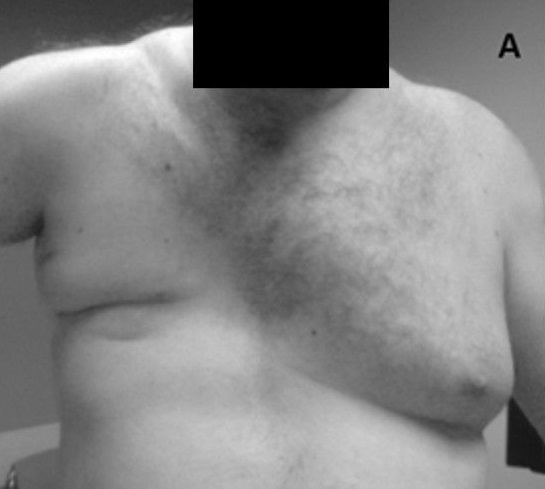
Poland Syndrome With Absence of Pectoralis Major Muscle
KJ Lizarraga and AAF De Salles, Public Domain, via Wikimedia Commons
References
Al Faleh K, Al Saadi M, Khalid-Bantuas S. Poland's Syndrome with Absent Limb Anomalies. Journal of clinical neonatology. 2014 Jan:3(1):44-6. doi: 10.4103/2249-4847.128735. Epub [PubMed PMID: 24741541]
Level 3 (low-level) evidenceIbrahim A, Ramatu A, Helen A. Poland syndrome a rare congenital anomaly. Indian journal of human genetics. 2013 Jul:19(3):349-51. doi: 10.4103/0971-6866.120824. Epub [PubMed PMID: 24339551]
Level 3 (low-level) evidenceShipkov CD, Anastassov YK. Bilateral Poland anomaly: does it exist? American journal of medical genetics. Part A. 2003 Apr 1:118A(1):101 [PubMed PMID: 12605453]
Level 3 (low-level) evidenceBlanco FC, Elliott ST, Sandler AD. Management of congenital chest wall deformities. Seminars in plastic surgery. 2011 Feb:25(1):107-16. doi: 10.1055/s-0031-1275177. Epub [PubMed PMID: 22294949]
Bavinck JN,Weaver DD, Subclavian artery supply disruption sequence: hypothesis of a vascular etiology for Poland, Klippel-Feil, and M�bius anomalies. American journal of medical genetics. 1986 Apr [PubMed PMID: 3008556]
Martínez-Frías ML, Czeizel AE, Rodríguez-Pinilla E, Bermejo E. Smoking during pregnancy and Poland sequence: results of a population-based registry and a case-control registry. Teratology. 1999 Jan:59(1):35-8 [PubMed PMID: 9988881]
Level 2 (mid-level) evidencePuvabanditsin S, Garrow E, Augustin G, Titapiwatanakul R, Kuniyoshi KM. Poland-Möbius syndrome and cocaine abuse: a relook at vascular etiology. Pediatric neurology. 2005 Apr:32(4):285-7 [PubMed PMID: 15797189]
Level 3 (low-level) evidenceRosa RF, Travi GM, Valiatti F, Zen PR, Pinto LL, Kiss A, Graziadio C, Paskulin GA. Poland syndrome associated with an aberrant subclavian artery and vascular abnormalities of the retina in a child exposed to misoprostol during pregnancy. Birth defects research. Part A, Clinical and molecular teratology. 2007 Jun:79(6):507-11 [PubMed PMID: 17393483]
Level 3 (low-level) evidenceSamuels TH,Haider MA,Kirkbride P, Poland's syndrome: a mammographic presentation. AJR. American journal of roentgenology. 1996 Feb [PubMed PMID: 8553944]
Level 3 (low-level) evidenceYiyit N, Işıtmangil T, Öksüz S. Clinical analysis of 113 patients with Poland syndrome. The Annals of thoracic surgery. 2015 Mar:99(3):999-1004. doi: 10.1016/j.athoracsur.2014.10.036. Epub 2015 Jan 27 [PubMed PMID: 25633462]
Level 2 (mid-level) evidenceDavid TJ. Familial Poland anomaly. Journal of medical genetics. 1982 Aug:19(4):293-6 [PubMed PMID: 6288948]
Level 3 (low-level) evidenceRam AN, Chung KC. Poland's syndrome: current thoughts in the setting of a controversy. Plastic and reconstructive surgery. 2009 Mar:123(3):949-953. doi: 10.1097/PRS.0b013e318199f508. Epub [PubMed PMID: 19319059]
Level 3 (low-level) evidenceGui L,Shen S,Mei W, Anaesthesia for chest wall reconstruction in a patient with Poland syndrome: CARE-compliant case report and literature review. BMC anesthesiology. 2018 May 24 [PubMed PMID: 29793431]
Level 3 (low-level) evidenceEroglu A, Yildiz D, Tunc H. Dextrocardia is a component of left-sided Poland syndrome. The Journal of thoracic and cardiovascular surgery. 2005 Nov:130(5):1471-2 [PubMed PMID: 16256811]
Level 3 (low-level) evidenceSeyfer AE, Fox JP, Hamilton CG. Poland syndrome: evaluation and treatment of the chest wall in 63 patients. Plastic and reconstructive surgery. 2010 Sep:126(3):902-911. doi: 10.1097/PRS.0b013e3181e60435. Epub [PubMed PMID: 20811224]
Catena N, Divizia MT, Calevo MG, Baban A, Torre M, Ravazzolo R, Lerone M, Sénès FM. Hand and upper limb anomalies in Poland syndrome: a new proposal of classification. Journal of pediatric orthopedics. 2012 Oct-Nov:32(7):727-31. doi: 10.1097/BPO.0b013e318269c898. Epub [PubMed PMID: 22955538]
Level 2 (mid-level) evidenceDelay E,La Marca S,Guerid S, [Correction of thoraco-mammary deformity of Poland syndrome]. Annales de chirurgie plastique et esthetique. 2016 Oct [PubMed PMID: 27567946]
Spear SL, Pelletiere CV, Lee ES, Grotting JC. Anterior thoracic hypoplasia: a separate entity from Poland syndrome. Plastic and reconstructive surgery. 2004 Jan:113(1):69-77; discussion 78-9 [PubMed PMID: 14707624]
Sharma CM, Kumar S, Meghwani MK, Agrawal RP. Poland syndrome. Indian journal of human genetics. 2014 Jan:20(1):82-4. doi: 10.4103/0971-6866.132764. Epub [PubMed PMID: 24959021]
Level 3 (low-level) evidenceCaouette-Laberge L, Borsuk D. Congenital anomalies of the breast. Seminars in plastic surgery. 2013 Feb:27(1):36-41. doi: 10.1055/s-0033-1343995. Epub [PubMed PMID: 24872738]
Cochran JH Jr,Pauly TJ,Edstrom LE,Dibbell DG, Hypoplasia of the latissimus dorsi muscle complicating breast reconstruction in Poland's syndrome. Annals of plastic surgery. 1981 May [PubMed PMID: 6264835]
Level 3 (low-level) evidenceLacorte D, Marsella M, Guerrini P. A case of Poland Syndrome associated with dextroposition. Italian journal of pediatrics. 2010 Feb 20:36():21. doi: 10.1186/1824-7288-36-21. Epub 2010 Feb 20 [PubMed PMID: 20170539]
Level 3 (low-level) evidenceShamberger RC, Welch KJ, Upton J 3rd. Surgical treatment of thoracic deformity in Poland's syndrome. Journal of pediatric surgery. 1989 Aug:24(8):760-5; discussion 766 [PubMed PMID: 2549232]
Chopan M, Sayadi L, Laub D. Mobius syndrome and poland syndrome presenting together in a single patient. Eplasty. 2015:15():ic12 [PubMed PMID: 25834693]
Erol M,Caksen H,Tan O,Atik B,Unal O,Odaba? D, Report of a girl with Klippel-feil syndrome and Poland anomaly. Genetic counseling (Geneva, Switzerland). 2004 [PubMed PMID: 15658624]
Level 3 (low-level) evidencePaladini D, D'Armiento MR, Martinelli P. Prenatal ultrasound diagnosis of poland syndrome. Obstetrics and gynecology. 2004 Nov:104(5 Pt 2):1156-9 [PubMed PMID: 15516435]
Level 3 (low-level) evidenceBainbridge LC, Wright AR, Kanthan R. Computed tomography in the preoperative assessment of Poland's syndrome. British journal of plastic surgery. 1991 Nov-Dec:44(8):604-7 [PubMed PMID: 1773224]
Level 3 (low-level) evidencePerez Aznar JM, Urbano J, Garcia Laborda E, Quevedo Moreno P, Ferrer Vergara L. Breast and pectoralis muscle hypoplasia. A mild degree of Poland's syndrome. Acta radiologica (Stockholm, Sweden : 1987). 1996 Sep:37(5):759-62 [PubMed PMID: 8915289]
Smereczy?ski A,Ko?aczyk K,Bernatowicz E, Chest wall - underappreciated structure in sonography. Part II: Non-cancerous lesions. Journal of ultrasonography. 2017 Dec [PubMed PMID: 29375903]
Fokin AA,Robicsek F, Poland's syndrome revisited. The Annals of thoracic surgery. 2002 Dec [PubMed PMID: 12643435]
Fija?kowska M,Antoszewski B, Surgical treatment of patients with Poland's syndrome--own experience. Polski przeglad chirurgiczny. 2011 Dec [PubMed PMID: 22343203]
Level 2 (mid-level) evidenceFreitas Rda S, o Tolazzi AR, Martins VD, Knop BA, Graf RM, Cruz GA. Poland's syndrome: different clinical presentations and surgical reconstructions in 18 cases. Aesthetic plastic surgery. 2007 Mar-Apr:31(2):140-6 [PubMed PMID: 17093886]
Level 3 (low-level) evidenceBraun TL, Trost JG, Pederson WC. Syndactyly Release. Seminars in plastic surgery. 2016 Nov:30(4):162-170 [PubMed PMID: 27895538]
Losken A, Fishman I, Denson DD, Moyer HR, Carlson GW. An objective evaluation of breast symmetry and shape differences using 3-dimensional images. Annals of plastic surgery. 2005 Dec:55(6):571-5 [PubMed PMID: 16327452]
Plesca M, Bordea C, El Houcheimi B, Ichim E, Blidaru A. Evolution of radical mastectomy for breast cancer. Journal of medicine and life. 2016 Apr-Jun:9(2):183-6 [PubMed PMID: 27453752]
Jansari M, Karkhanis V, Joshi JM. Unilateral hyperlucent lung: Always think ACROSS. Lung India : official organ of Indian Chest Society. 2013 Oct:30(4):368-9. doi: 10.4103/0970-2113.120629. Epub [PubMed PMID: 24339504]
Sunitha VC, Narayanan S, Nair PP, Prakash ML. Left-sided Poland's syndrome in a girl with rare associations like spina bifida and diaphragmatic hernia. BMJ case reports. 2013 Sep 20:2013():. doi: 10.1136/bcr-2013-200930. Epub 2013 Sep 20 [PubMed PMID: 24057335]
Level 3 (low-level) evidenceGarg R,Saheer S,Gupta V,Mehra S, Poland sequence: Series of two cases and brief review of the literature. Annals of thoracic medicine. 2012 Apr [PubMed PMID: 22558018]
Level 3 (low-level) evidenceLantzsch T, Lampe D, Kantelhardt EJ. Correction of Poland's Syndrome: Case Report and Review of the Current Literature. Breast care (Basel, Switzerland). 2013 May:8(2):139-42. doi: 10.1159/000350778. Epub [PubMed PMID: 24419214]
Level 3 (low-level) evidenceBaldelli I, Santi P, Dova L, Cardoni G, Ciliberti R, Franchelli S, Merlo DF, Romanini MV. Body Image Disorders and Surgical Timing in Patients Affected by Poland Syndrome: Data Analysis of 58 Case Studies. Plastic and reconstructive surgery. 2016 Apr:137(4):1273-1282. doi: 10.1097/PRS.0000000000002018. Epub [PubMed PMID: 27018681]
Level 3 (low-level) evidenceRibeiro RC, Saltz R, Mangles MG, Koch H. Clinical and radiographic poland syndrome classification: a proposal. Aesthetic surgery journal. 2009 Nov-Dec:29(6):494-504. doi: 10.1016/j.asj.2009.09.015. Epub [PubMed PMID: 19944994]
Level 2 (mid-level) evidence