
 Anatomy, Abdomen and Pelvis, Quadratus Lumborum
Anatomy, Abdomen and Pelvis, Quadratus Lumborum
Introduction
The quadratus lumborum is a muscle in the posterior inferior trunk lateral to the spine (see Image. Abdominopelvic Muscles). This muscle attaches to the iliac crest, the transverse processes of lumbar vertebrae 1 to 4, and the 12th rib. The quadratus lumborum's complex organization makes it difficult to precisely identify its actions through the contraction of its fibers. This muscle is an integral part of the thoracolumbar fascia.
Uncertainty persists about whether a quadratus lumborum abnormality is the primary source of back pain. This muscle potentially acts as a junction of the forces exerted by the neighboring muscles, influencing the vectors of the different tensions produced. The quadratus lumborum is a significant means of access for anesthesia during surgery on the back, lower limbs, or abdominal area, thanks to its strategic position and the entropic scheme of its fibers. Understanding the latest anatomical and clinical information on the quadratus lumborum is essential for treating various musculoskeletal conditions of the lower back.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Anatomy
The quadratus lumborum is an integral part of the thoracolumbar fascia, a myofascial system that covers the posterior trunk and involves parts of the lower and upper limbs. The quadratus lumborum is flat and quadrangular in shape. The muscle works with the multifidus and erector spinae to antagonize the abdominal muscles. The quadratus lumborum originates from the iliac crest's inner lip and the iliolumbar ligament and inserts on the 12th rib's internal surface and the transverse processes of the lumbar bodies of L1 to L4.[1]
The quadratus lumborum has 3 muscle fiber layers with different vectors. The thin anterior layer comprises iliocostal (iliac crest to ribs) and iliothoracic (iliac crest to the T12 vertebral body's lateral margin) muscle fibers, which terminate with a tendon or muscle. The middle layer comprises lumbocostal muscle fibers, which originate from the transverse processes of the lumbar vertebrae and insert on the 12th rib. These muscle fibers vary significantly in size, direction, and thickness.
The posterior layer consists of lateral iliocostal fibers and medial iliolumbar fibers, connecting the iliac crest to the lumbar vertebrae's transverse processes. The iliocostal muscle bundles may involve the thoracolumbar fascia, inserting with tendon endings. This layer is thicker in the caudal area and more tapered in the rostral portion.
The highly variable arrangement of the quadratus lumborum muscle fibers prevents the recognition of a precise orientation pattern. The muscle is generally located medial to the aponeurosis of the transverse abdominal muscle.
Function
Anatomy texts describe the quadratus lumborum as a lumbar spine extensor, stabilizer, and lateral tiltor, and an accessory muscle for inspiration. However, a cadaver study has raised doubts about the quadratus lumborum's actions.
During extension, the quadratus lumborum exerts only a force of 10 N, compared to the erector spinae's 100 N and the multifidus' 150 N. Extending the lumbar area in the sagittal plane with such a small force (10 N) seems unlikely. The quadratus lumborum is positioned laterally but exerts only a force of 10 N during a lateral trunk tilt. The quadratus lumborum participates with less than 10% of the force required for a coronal inclination.
The forces exerted by the erector spinae and multifidus in the lumbar vertebrae are about 1800 N and 2800 N, respectively. The quadratus lumborum exercises only 200 N. Thus, this muscle does not appear to be a significant lumbar stabilizer. As an accessory inspiratory muscle, the quadratus lumborum cannot transmit contractile forces to the diaphragm due to the mobility of the last rib.[2]
Thus, the quadratus lumborum likely serves as a junction for forces exerted by neighboring muscles, influencing the vectors of various tensions due to its strategic position and fiber arrangement. The lateral arcuate ligament of the diaphragm rests on the quadratus lumborum, potentially enhancing respiratory function by allowing the muscle to act as a pivot.
Embryology
The embryonic mesoderm leaflet gives rise to the skeletal musculature and is already visible from the 2nd week of gestation. The mesoderm divides into 4 areas in the mediolateral direction. The chordomesoderm makes up the notochord. The paraxial mesoderm is organized into 2 slings, located laterally to the notochord and following a longitudinal course. These slings are fragmented into metameric small masses due to the formation of transverse grooves. The intermediate mesoderm is adjacent to the somites in the cervical, thoracic, and caudal regions. The lateral mesoderm is furthest from the notochord and delaminated into 2 parallel sheets.
During embryonic development, the median cellular cord forms the notochord, the embryo's first axial structure. Although short-lived, the notochord induces changes in the surrounding areas. From the cephalic end, the paraxial mesoderm on either side of the notochord fragments into 2 series of cylindrical thickenings with a spiral organization, known as somitomeres, due to transverse grooves.
Somitomere segmentation begins in the most cranial region of the mesoderm, with a more marked metamer in the cervical, thoracic, lumbar, sacral, and coccygeal regions. The first 7 pairs of somitomeres have a slightly accentuated segmentation and form the striated muscles of the face, jaw, and neck, all subsequent forms of segmental units called "somites." About 42 to 44 somites form, of which the 1st corresponds to the 8th somitomere.
The first 4 pairs of somites appear in the occipital region, contributing to the formation of the occipital and facial bones and the eye and tongue muscles. Eight pairs of cervical somites follow, with the 1st contributing to the formation of the occipital bone, while the remaining 7 form the cervical vertebrae, muscles, and associated dermal structures.
In succession, 12 pairs of thoracic somites form the vertebrae, musculature, and rib cage bones, contributing to upper limb development. Five pairs of lumbar somites form the lumbar vertebrae, muscles, and abdominal dermis. Five pairs of sacral somites form the sacrum along with its associated muscles and dermal elements. About 3 to 5 pairs of coccygeal somites form the coccyx.[3][4]
Blood Supply and Lymphatics
The quadratus lumborum gets its vascular supply via the lumbar arteries and a lumbar branch of the iliolumbar artery. The 4 lumbar arteries on each side arise from the posterior surface of the aorta at the level of the 1st 4 lumbar vertebrae. These blood vessels run posteriorly behind the sympathetic chain and under the tendinous arch of the iliopsoas muscle before perfusing the quadratus lumborum. The first 3 arteries pass posteriorly to the quadratus lumborum, while the 4th passes anteriorly.[5]
The iliolumbar artery is the 1st tributary of the internal iliac artery (or hypogastric artery). The iliolumbar artery rises behind the psoas and iliacus (in the iliac fossa), where the individual branches feed the iliac muscle. Branches from this artery extend to the psoas, quadratus lumborum, and transverse abdominal muscles. Another branch supplies the spinal canal between the 5th lumbar vertebra and the sacrum.[6]
The lumbar veins on each side connect through longitudinal anastomotic vessels that merge to form a small vertical trunk known as the "ascending lumbar vein." This vessel communicates with the iliolumbar vein at the inferior end and, sometimes, the common iliac vein. At the superior end, the ascending lumbar vein gives rise to the azygos vein on the right and the hemizygous vein on the left, creating an important anastomotic pathway between the inferior and superior vena cavae.[5]
The lumbar lymph nodes of the abdominal cavity, which drain the lymph from the quadratus lumborum, are associated with the inferior vena cava and the abdominal aorta.[7]
Nerves
The quadratus lumborum is innervated by the 12th thoracic intercostal, iliohypogastric, and ilioinguinal nerves.
Muscles
The subcostal muscle runs in front of the quadratus lumborum and contacts its terminal portion in about 2.9% of the population. The subcostal muscle is electrically activated during expiration, suggesting that the quadratus lumborum might influence forced expiration, though further study is warranted.[8]
The quadratus lumborum is a posterior continuation of the transverse abdominal muscle, which is part of the anterior fascial system of the body, extending from the deep anterior fascia of the neck to the transversalis fascia up to the pubis. The transversalis fascia penetrates the abdominal musculature. We can assume that abnormal tension on these muscles, eg, from a globular abdomen, can negatively influence the resting tension of the quadratus lumborum, altering the distribution of the lumbar area loads.
Physiologic Variants
No reports of hyperplasia or agenesis of the quadratus lumborum muscle exist in the literature.
Surgical Considerations
Quadratus Lumborum Anesthesia
Dr. Blanco Rafael was the first to use quadratus lumborum anesthesia in surgery in 2007. Both anterior and posterior approaches, whether lateral or intramuscular, are valid when assisted by ultrasound guidance.[9] Anesthesia administered in this manner covers dermatomes T4 to L2. The anesthetic passes through the paravertebral spaces, distributing via the blood and lymphatic vessels before reaching the nerves. This method is useful not only before surgery, including abdominal surgery, colostomy, cesarean section, laparoscopy, pyeloplasty, and gastrotomy, but also in the postoperative period to relieve pain.
Hip Fracture Surgery
Hip fractures are often complicated, usually occurring in patients of advanced age with various medical comorbidities. Thus, managing the condition in these patients requires innovative anesthetic techniques that effectively reduce the risks of anesthesia while ensuring adequate pain control. Whether used alone or in combination with other analgesic methods, the quadratus lumborum block shows clinical efficacy in controlling perioperative pain for this group.[10][11]
Clinical Significance
No consensus exists in the literature on whether altered quadratus lumborum tone may be the primary cause of back pain.[12] The quadratus lumborum is smaller in the dominant leg than on the opposite side. However, this muscle's size does not differ significantly between people with and without low back pain.[13][14]
Since the 12th thoracic, ilioinguinal, and iliohypogastric nerves pass through and branch to the quadratus lumborum, inflammation of the nervous tissue due to limited excursion (entrapment) may produce a syndrome that mimics low back pain.
Trigger points can involve the quadratus lumborum. This condition may also mimic lumbar area pain syndromes.[15]
Another cause of low back pain related to the anatomical presence of the quadratus lumborum is the development of heterotopic ossification or myositis ossificans, which may result from direct trauma and inadequate healing.[16] The etiopathogenesis of this condition may not always be clear in the absence of trauma.
One must consider that a single muscle rarely causes pain, except in cases of direct trauma. All muscles interconnect through the fascial system, and contractile areas with altered function can lead to issues in the surrounding muscular regions.
Other Issues
One of the best approaches to nonsurgical treatment of the quadratus lumborum is fascial osteopathic therapy, a gentle procedure that respects the patient’s pain while improving pain sensations.[17]
A recent study has shown that dry needling of the gluteus maximus and quadratus lumborum can relieve pain and enhance the performance of athletes suffering from patellofemoral pain syndrome.[18]
Media
(Click Image to Enlarge)
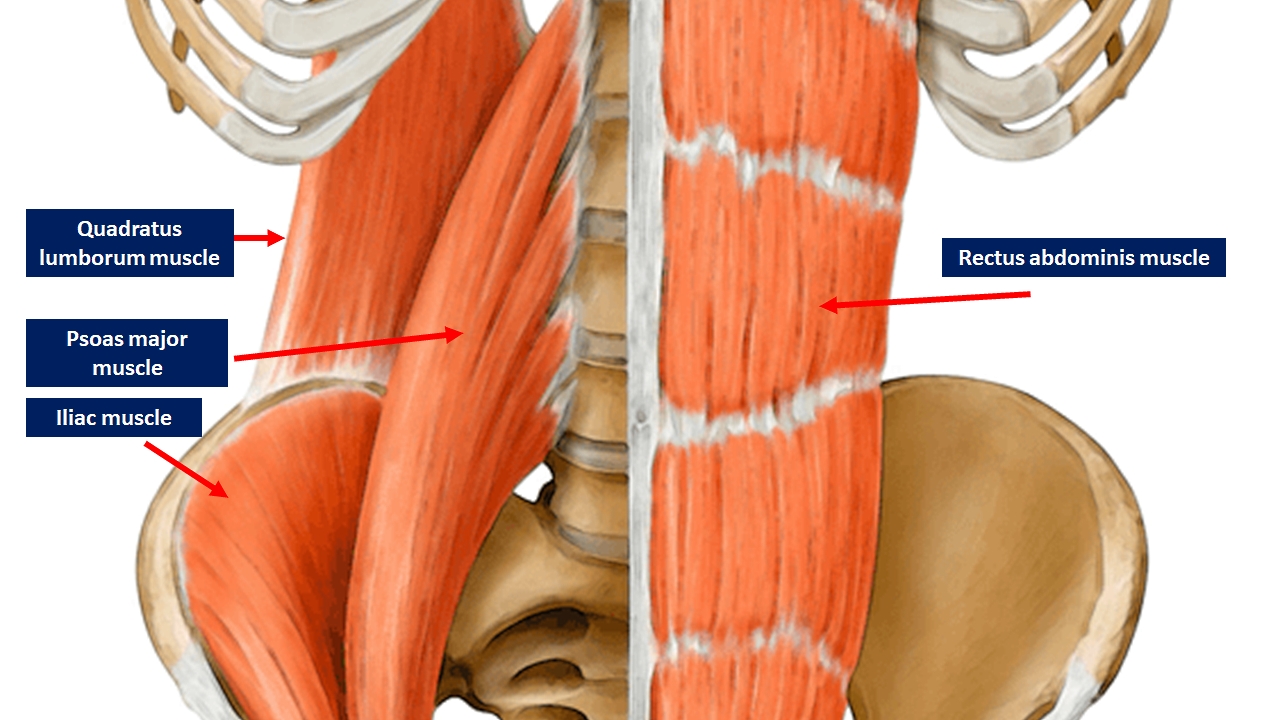
Abdominopelvic Muscles. This image shows the anatomic relationships between the quadratus lumborum, rectus abdominis, iliac, and psoas major. The unlabeled bony structures include the ribs, vertebrae, sacrum, and hip bone.
Contributed by Bruno Bordoni, PhD
References
Grzonkowska M, Baumgart M, Badura M, Dombek M, Wiśniewski M, Paruszewska-Achtel M, Szpinda M. Quantitative anatomy of the growing quadratus lumborum in the human foetus. Surgical and radiologic anatomy : SRA. 2018 Jan:40(1):91-98. doi: 10.1007/s00276-017-1901-4. Epub 2017 Jul 29 [PubMed PMID: 28756538]
Phillips S, Mercer S, Bogduk N. Anatomy and biomechanics of quadratus lumborum. Proceedings of the Institution of Mechanical Engineers. Part H, Journal of engineering in medicine. 2008 Feb:222(2):151-9 [PubMed PMID: 18441751]
Chal J, Pourquié O. Making muscle: skeletal myogenesis in vivo and in vitro. Development (Cambridge, England). 2017 Jun 15:144(12):2104-2122. doi: 10.1242/dev.151035. Epub [PubMed PMID: 28634270]
Hernández-Hernández JM, García-González EG, Brun CE, Rudnicki MA. The myogenic regulatory factors, determinants of muscle development, cell identity and regeneration. Seminars in cell & developmental biology. 2017 Dec:72():10-18. doi: 10.1016/j.semcdb.2017.11.010. Epub 2017 Nov 15 [PubMed PMID: 29127045]
Beveridge TS, Power A, Johnson M, Power NE, Allman BL. The lumbar arteries and veins: Quantification of variable anatomical positioning with application to retroperitoneal surgery. Clinical anatomy (New York, N.Y.). 2015 Jul:28(5):649-60. doi: 10.1002/ca.22504. Epub 2015 Feb 2 [PubMed PMID: 25644404]
Level 3 (low-level) evidenceSingh T, Andi K. Iliolumbar artery: a useful pedicle for the iliac crest free flap in maxillofacial reconstruction. The British journal of oral & maxillofacial surgery. 2017 Apr:55(3):270-273. doi: 10.1016/j.bjoms.2016.12.012. Epub 2017 Jan 11 [PubMed PMID: 28089170]
Beveridge TS, Allman BL, Johnson M, Power A, Sheinfeld J, Power NE. Retroperitoneal Lymph Node Dissection: Anatomical and Technical Considerations from a Cadaveric Study. The Journal of urology. 2016 Dec:196(6):1764-1771. doi: 10.1016/j.juro.2016.06.091. Epub 2016 Jul 5 [PubMed PMID: 27389330]
Kim JH, Won HS, Chung IH, Kim IB. The enigmatic subcostal muscle: Anatomical study with application to spine and chest pain syndromes and avoidance of confusion on imaging. Clinical anatomy (New York, N.Y.). 2015 Nov:28(8):1017-21. doi: 10.1002/ca.22631. Epub 2015 Oct 5 [PubMed PMID: 26384842]
Ueshima H, Otake H, Lin JA. Ultrasound-Guided Quadratus Lumborum Block: An Updated Review of Anatomy and Techniques. BioMed research international. 2017:2017():2752876. doi: 10.1155/2017/2752876. Epub 2017 Jan 3 [PubMed PMID: 28154824]
Tulgar S, Ermis MN, Ozer Z. Combination of lumbar erector spinae plane block and transmuscular quadratus lumborum block for surgical anaesthesia in hemiarthroplasty for femoral neck fracture. Indian journal of anaesthesia. 2018 Oct:62(10):802-805. doi: 10.4103/ija.IJA_230_18. Epub [PubMed PMID: 30443064]
Adhikary SD, Short AJ, El-Boghdadly K, Abdelmalak MJ, Chin KJ. Transmuscular quadratus lumborum versus lumbar plexus block for total hip arthroplasty: A retrospective propensity score matched cohort study. Journal of anaesthesiology, clinical pharmacology. 2018 Jul-Sep:34(3):372-378. doi: 10.4103/joacp.JOACP_335_17. Epub [PubMed PMID: 30386022]
Level 2 (mid-level) evidenceSions JM, Elliott JM, Pohlig RT, Hicks GE. Trunk Muscle Characteristics of the Multifidi, Erector Spinae, Psoas, and Quadratus Lumborum in Older Adults With and Without Chronic Low Back Pain. The Journal of orthopaedic and sports physical therapy. 2017 Mar:47(3):173-179. doi: 10.2519/jospt.2017.7002. Epub 2017 Feb 3 [PubMed PMID: 28158957]
Aboufazeli M, Akbari M, Jamshidi AA, Jafarpisheh MS. Comparison of Selective Local and Global Muscle Thicknesses in Females with and without Chronic Low Back Pain. Ortopedia, traumatologia, rehabilitacja. 2018 Jun 27:20(3):197-204. doi: 10.5604/01.3001.0012.1473. Epub [PubMed PMID: 30152768]
Ranger TA, Cicuttini FM, Jensen TS, Peiris WL, Hussain SM, Fairley J, Urquhart DM. Are the size and composition of the paraspinal muscles associated with low back pain? A systematic review. The spine journal : official journal of the North American Spine Society. 2017 Nov:17(11):1729-1748. doi: 10.1016/j.spinee.2017.07.002. Epub 2017 Jul 26 [PubMed PMID: 28756299]
Level 1 (high-level) evidenceHong JO, Park JS, Jeon DG, Yoon WH, Park JH. Extracorporeal Shock Wave Therapy Versus Trigger Point Injection in the Treatment of Myofascial Pain Syndrome in the Quadratus Lumborum. Annals of rehabilitation medicine. 2017 Aug:41(4):582-588. doi: 10.5535/arm.2017.41.4.582. Epub 2017 Aug 31 [PubMed PMID: 28971042]
Alport B, Horne D, Burbridge B. Heterotopic ossification of the quadratus lumborum muscle. Journal of radiology case reports. 2014 Jan:8(1):41-6. doi: 10.3941/jrcr.v8i1.1348. Epub 2014 Jan 1 [PubMed PMID: 24967013]
Level 3 (low-level) evidenceTozzi P, Bongiorno D, Vitturini C. Fascial release effects on patients with non-specific cervical or lumbar pain. Journal of bodywork and movement therapies. 2011 Oct:15(4):405-16. doi: 10.1016/j.jbmt.2010.11.003. Epub 2011 Jan 8 [PubMed PMID: 21943614]
Zarei H, Bervis S, Piroozi S, Motealleh A. Added Value of Gluteus Medius and Quadratus Lumborum Dry Needling in Improving Knee Pain and Function in Female Athletes With Patellofemoral Pain Syndrome: A Randomized Clinical Trial. Archives of physical medicine and rehabilitation. 2020 Feb:101(2):265-274. doi: 10.1016/j.apmr.2019.07.009. Epub 2019 Aug 26 [PubMed PMID: 31465756]
Level 1 (high-level) evidence