 Anatomy, Abdomen and Pelvis, Rectus Femoris Muscle
Anatomy, Abdomen and Pelvis, Rectus Femoris Muscle
Introduction
The rectus femoris is the anterior thigh compartment's most superficial and nearly vertically oriented muscle. This bipennate structure is a component of the quadriceps muscle complex, one of the knee's most important dynamic stabilizers.[1] The rectus femoris is also known as the "kicking muscle" for its involvement in activities involving forceful knee extension. As in other musculoskeletal structures, many rectus femoris injuries arise from sports activities, trauma, and occupations requiring repetitive movement of this muscle.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure of the Rectus Femoris
The rectus femoris is fusiform in shape with superficial bipenniform fibers and deep, vertically oriented fibers (see Image. Right Quadriceps Femoris, Anterior View). This muscle has two origins. The "direct head" originates from the anterior inferior iliac spine, while the superior acetabular ridge is the origin of the "indirect head." The muscle heads fuse distally at an acute angle to form a common tendon.[1][2]
Inferiorly, the rectus femoris inserts conjointly with the other quadriceps muscles on the patellar base via the quadriceps tendon. The connection between the quadriceps tendon, patella, and patellar ligament allows the quadriceps muscle complex to have another insertion point on the tibial tuberosity.
Thus, the rectus femoris can be easily distinguished from the other quadriceps muscles by its nearly vertical orientation, superficial location, and crossing of 2 lower limb joints, namely, the thigh and knee.[1]
Function of the Rectus Femoris
The rectus femoris flexes the hip along with the sartorius and iliopsoas and extends the knee as part of the quadriceps femoris. This superficial muscle antagonizes the hamstrings at the knee and hip.[1][3]
Active and passive insufficiency are functional limitations that multi-joint muscles can acquire. In the case of the rectus femoris, active insufficiency occurs when full extension of the knee limits its ability to flex the hip and vice-versa. The muscle is highly contracted in such a state. Thus, the rectus femoris becomes a weak knee extensor in the sitting position when the hip is flexed.
On the other hand, passive insufficiency of the rectus femoris occurs when full knee flexion limits its capacity to extend the hip and vice-versa. In this case, the muscle is at its longest.[1]
Embryology
The lower limb bud appears during the 5th week of development. The bud originates laterally from the L2 to S2 spinal segments and contains all the primary germ layers, the ectoderm, endoderm, and mesoderm. The muscle tissue of the rectus femoris arises from the myotomic portions of somites, which arise from the mesoderm. Meanwhile, the skeletal elements supporting the lower limb come from the lateral plate somatic mesoderm. During embryogenesis, the lower limb rotates 90 degrees medially about the longitudinal axis, bringing the knee to the anterior aspect of the fetus.[3]
Blood Supply and Lymphatics
The femoral artery supplies blood to the quadriceps muscle via the lateral femoral circumflex branch. The muscle's venous drainage is via the femoral vein and its branches.
Lymphatic vessels of the anterior thigh drain into the superficial inguinal nodes. From there, the vessels ascend to the external iliac and lateral aortic lymph nodes.[15]
Nerves
Cortical signals from the precentral gyrus apex descend via the corticospinal tract. About 90% of the fibers in this nerve tract decussate at the level of the lower medulla at a region called the "pyramidal tract decussation." These fibers continue to descend on the contralateral side as the lateral corticospinal tract until they reach the lower motor neurons below the upper thoracic spinal cord. The remaining 10% of the fibers that do not decussate continue as the ventral corticospinal tract, but they do not innervate structures below the upper thoracic spinal cord.
To reach the quadriceps femoris muscle, the lateral corticospinal tract's fibers synapse with the lower motor neurons at the L4 level. From there, the neuronal signal propagates toward the L4 anterior rami and the lumbar plexus.
The femoral nerve forms from the L4 anterior rami and has contributions from L2 and L3 fibers. The femoral nerve innervates all 4 components of the quadriceps femoris, including the rectus femoris.[1]
Physiologic Variants
Accessory muscles can arise from the rectus femoris. These variations include a muscle slip from the acetabulum that inserts directly into the vastus lateralis. The rectus femoris muscle's proximal origin may also have only 1 instead of 2 heads, with the lone tendon arising from the lower anterior iliac spine and the acetabular origin missing.[1][4]
Surgical Considerations
Acute rectus femoris muscle injuries present with a tearing sensation and abrupt-onset pain. By comparison, subacute injuries manifest gradually, usually with mild-to-moderate pain aggravated by running at the onset. Ultrasonography and MRI aid in the diagnosis and monitoring of injuries to this muscle.[5]
Proximal rectus femoris tears are uncommon but are associated with soccer and other sports activities requiring frequent kicking and sprinting. The direct head is more often involved than the indirect head. Total avulsions involve both. Acute single-head proximal rectus femoris tears may be managed conservatively, though they are prone to recurrence. Surgery is appropriate for total avulsion and recurrent single-head tears. Both conditions have a good prognosis, with patients being able to return to preinjury functional levels after surgery.[16]
A distal rectus femoris tear is more commonly associated with quadriceps tendon ruptures, which affect the quadriceps muscle as a whole. Isolated tears are uncommon. Quadriceps tendon tears are disabling and usually require surgical management.
Avulsed tendon repairs involve sewing the tendon into sutures anchored to the bony origin. The torn tendon may be sewn to the tendon stump if it has sufficient tissue for surgical sewing. Tendon allografts may be used for reconstruction if the tendon edges are unsuitable for repair or cannot be adequately mobilized.[6]
Clinical Significance
The rectus femoris muscle is the most frequently injured quadriceps muscle due to its superficial location. Contusion and rupture of this muscle are common in sports.[5][7][8][9] Trauma and intense exercise can tear the rectus muscle at the proximal or distal insertions.[10] A partial tear is usually treated conservatively with activity modification and positional restriction.[11] Physical therapy may also help rehabilitate torn muscles.
Acute rectus femoris strain typically presents with swelling and moderate to severe pain in the groin or anterior aspect of the hip. Knee extension is also impaired.[12] MRI detects rectus femoris strains.
Myositis ossificans involving the rectus femoris may arise from both traumatic and non-traumatic causes.[13] Most patients are managed conservatively with excellent outcomes. Typically, athletes progress to light activity in 2 or 3 months, full activity in 6 months, and return to their preinjury performance level in 1 year. Persistent cases may require surgical excision.[14]
Media
(Click Image to Enlarge)
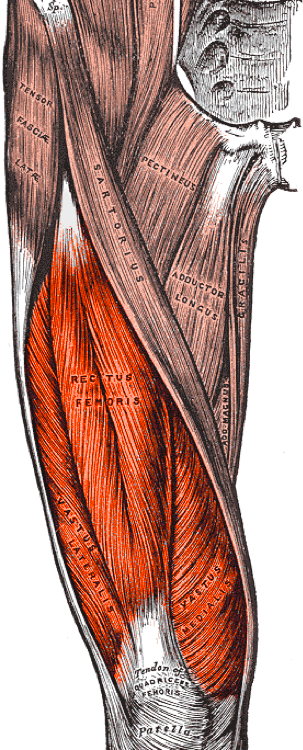
Right Quadriceps Femoris, Anterior View. This illustration shows the rectus femoris, vastus lateralis, and vastus medialis. Other structures are the tensor fascia lata, sartorius, pectineus, adductor longus, gracilis, adductor magnus, quadriceps femoris tendon, and patella.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Bordoni B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Quadriceps Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30020706]
Kumaravel M, Bawa P, Murai N. Magnetic resonance imaging of muscle injury in elite American football players: Predictors for return to play and performance. European journal of radiology. 2018 Nov:108():155-164. doi: 10.1016/j.ejrad.2018.09.028. Epub 2018 Sep 27 [PubMed PMID: 30396649]
Mahabadi N, Lew V, Kang M. Anatomy, Abdomen and Pelvis: Femoral Sheath. StatPearls. 2023 Jan:(): [PubMed PMID: 29494010]
Biondi NL, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Vastus Lateralis Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30335342]
Mendiguchia J, Alentorn-Geli E, Idoate F, Myer GD. Rectus femoris muscle injuries in football: a clinically relevant review of mechanisms of injury, risk factors and preventive strategies. British journal of sports medicine. 2013 Apr:47(6):359-66. doi: 10.1136/bjsports-2012-091250. Epub 2012 Aug 3 [PubMed PMID: 22864009]
Volk WR, Yagnik GP, Uribe JW. Complications in brief: Quadriceps and patellar tendon tears. Clinical orthopaedics and related research. 2014 Mar:472(3):1050-7. doi: 10.1007/s11999-013-3396-6. Epub 2013 Dec 12 [PubMed PMID: 24338040]
Cross TM, Gibbs N, Houang MT, Cameron M. Acute quadriceps muscle strains: magnetic resonance imaging features and prognosis. The American journal of sports medicine. 2004 Apr-May:32(3):710-9 [PubMed PMID: 15090389]
Gyftopoulos S, Rosenberg ZS, Schweitzer ME, Bordalo-Rodrigues M. Normal anatomy and strains of the deep musculotendinous junction of the proximal rectus femoris: MRI features. AJR. American journal of roentgenology. 2008 Mar:190(3):W182-6. doi: 10.2214/AJR.07.2947. Epub [PubMed PMID: 18287410]
Level 2 (mid-level) evidencePesquer L, Poussange N, Sonnery-Cottet B, Graveleau N, Meyer P, Dallaudiere B, Feldis M. Imaging of rectus femoris proximal tendinopathies. Skeletal radiology. 2016 Jul:45(7):889-97. doi: 10.1007/s00256-016-2345-3. Epub 2016 Mar 8 [PubMed PMID: 26956398]
Esser S, Jantz D, Hurdle MF, Taylor W. Proximal Rectus Femoris Avulsion: Ultrasonic Diagnosis and Nonoperative Management. Journal of athletic training. 2015 Jul:50(7):778-80. doi: 10.4085/1052-6050-50.2.13. Epub 2015 May 15 [PubMed PMID: 25978099]
Colombelli A, Polidoro F, Guerra G, Belluati A. Patellar and quadriceps tendons acute repair with suture anchors. Acta bio-medica : Atenei Parmensis. 2019 Jan 14:90(1-S):209-213. doi: 10.23750/abm.v90i1-S.8108. Epub 2019 Jan 14 [PubMed PMID: 30715027]
Lempainen L, Mechó S, Valle X, Mazzoni S, Villalon J, Freschi M, Stefanini L, García-Romero-Pérez A, Burova M, Pleshkov P, Pruna R, Pasta G, Kosola J. Management of anterior thigh injuries in soccer players: practical guide. BMC sports science, medicine & rehabilitation. 2022 Mar 18:14(1):41. doi: 10.1186/s13102-022-00428-y. Epub 2022 Mar 18 [PubMed PMID: 35303927]
Marques JP, Pinheiro JP, Santos Costa J, Moura D. Myositis ossificans of the quadriceps femoris in a soccer player. BMJ case reports. 2015 Aug 11:2015():. doi: 10.1136/bcr-2015-210545. Epub 2015 Aug 11 [PubMed PMID: 26264943]
Level 3 (low-level) evidenceDevilbiss Z, Hess M, Ho GWK. Myositis Ossificans in Sport: A Review. Current sports medicine reports. 2018 Sep:17(9):290-295. doi: 10.1249/JSR.0000000000000515. Epub [PubMed PMID: 30204632]