Introduction
Reticulocytes are immature red blood cells (RBCs) produced in the bone marrow and released into the peripheral blood, where they mature into RBCs within 1 to 2 days. An increase or decrease in reticulocyte count can be an indicator of erythropoiesis activity or failure, especially relative to anemias and bone marrow dysfunction.[1]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Flow cytometry is the most typical method of counting reticulocytes; this is an automated practice that provides a faster and more precise way to measure reticulocyte count.[2] The first step in the process is reticulocyte staining by mixing thiazole orange solution with whole blood. This solution is kept in the dark, incubated at room temperature, and then run through the laser-based machine. The stain adheres to ribosomal RNA (rRNA), which allows for the differentiation of reticulocyte staging. New cells have more RNA content compared to that more mature reticulocytes with low RNA content.[1] The reticulocyte count determined will be a percentage of the reticulocytes in the total amount of red blood cells in the field.[2]
Structure
The reticulocyte undergoes multiple structural changes as it transforms into a mature RBC. The process begins within the bone marrow, where an erythroblast undergoes chromatin and nuclear condensation. This process allows enucleation to take place by interacting with macrophages, forming a reticulocyte. Breakdown and expulsion of organelles begin while in the bone marrow and continue when the reticulocyte is in the bloodstream; it includes the endoplasm reticulum, Golgi apparatus, lysosomes, mitochondria, and ribosomes via both autophagic and non-autophagic pathways. Once in the bloodstream, RNA breakdown occurs, facilitated by ribonucleases.[3] Some rRNA will remain for RBC formation.[2] Changes in cell volume and membrane remodeling are thought to occur via exosomes. All these changes occur selectively, so the necessary proteins are available during the life of a reticulocyte but can be expelled when necessary to create a mature biconcave RBC.[2][3]
In comparison to a mature RBC, reticulocytes have greater volume, higher hemoglobin content, and lower hemoglobin concentration. Reticulocytes can only synthesize hemoglobin in the bone marrow. Thus, once they enter the peripheral blood, they have the maximum hemoglobin content they can have.[2]
Function
A reticulocyte functions as a step in the process of erythropoiesis. It forms from a differentiated hematopoietic stem cell.[4] Reticulocytes form in the bone marrow, where they continue to develop for 1 to 3 days. They are then released into the bloodstream with a life span of 1 to 2 days before they become mature RBCs.[5] During this time, the reticulocyte undergoes many changes to become a mature functioning RBC. An increase in erythropoietin (EPO) levels stimulates the bone marrow to increase reticulocyte production. EPO levels normally elevate for 3 to 4 days before an increase in the reticulocyte count presents.[1]
Microscopy, Light
In light microscopy, the sample must first be supravitally stained, usually using new methylene blue or brilliant cresyl blue, which binds to the RNA. The stain allows cells to be recognized by the blue intracytoplasmic precipitate, ranging from the appearance of granules to a network of reticular material.[2] It is mixed with equal parts whole blood and incubated at room temperature. Slides preparation is with a Wright counterstain, which helps illuminate the distinction of the reticulocytes with the background. The tester manually counts the reticulocytes under the electron microscope.[6][1]
Measuring reticulocyte count with light microscopy is not commonly used anymore. It has low reproducibility and can be unreliable, with a coefficient of variation ranging from 25 to 48%.[7]
Microscopy, Electron
Electron microscopy gives a more detailed view of individual reticulocytes and allows for organizational changes to be followed during their life span. Cell preparation is by fixing in a glutaraldehyde/tannic acid solution in sodium cacodylate, followed by resuspension in 2.0% agar. Agar slices are appropriately washed and then stained with 1.5% uranyl acetate in 50% methanol and lead citrate.[8]
In the beginning phase of reticulocytes, it is possible to visualize mitochondria (including heme synthesis), many ribosomes, endocytic vesicles, intracellular vesicles, and clathrin-coated pits. Microscopy also shows a much higher rate of iron incorporation in the early stages of reticulocytes. In more mature reticulocytes, one can see the degradation of the mitochondria, compaction of hemoglobin, and the presence of more intracellular vacuoles containing debris and exocytic vesicles.[8]
Clinical Significance
Reticulocytes are a useful clinical indicator of anemias and bone marrow response to anemia. Reticulocyte count in a healthy person should be between 0.5 to 2.5%.[9] When a patient is anemic and the bone marrow is unable to respond, the reticulocyte count will be low. When the bone marrow can respond appropriately, the reticulocyte count will increase.[1]
A decrease in reticulocyte count in patients can be caused by[1][3]:
- Hypochromic anemias: Iron deficiency anemia, sideroblastic anemia, and anemia of chronic disease are all causes of a decreased reticulocyte count because they result in decreased hemoglobin synthesis.
- Aplastic anemias: This is pancytopenia in response to bone marrow failure. While there are many causes of this, they all diminish erythropoiesis as reticulocytes form in the bone marrow. [1]
- Nutritional deficiency: Insufficient amounts of vitamin B12 and folate are causes of megaloblastic anemia. These nutrients are needed in the bone marrow to synthesize DNA, and without will cause a decrease in reticulocyte production.
- Aplastic crisis in hemolytic anemia: Aplastic crisis is a transient reduction in erythropoiesis due to a decline of precursors in the bone marrow. This is usually the result of an infection such as parvovirus B19, salmonella, and Streptococcus pneumoniae. Patients with hemolytic anemias have elevated reticulocyte counts, so when they present with a low count, it is possibly an aplastic crisis.
- Myelodysplastic syndromes: These syndromes characteristically demonstrate bone marrow damage from multiple causes. The erythropoietic cell line is usually affected, and the bone marrow is unable to produce reticulocytes.
Causes of increased reticulocyte count include[1]:
- Hemolytic anemias: These anemias are a result of red blood cell destruction. The bone marrow is still functional and has the required components to create reticulocytes. It responds to anemia by increasing the synthesis of reticulocytes.
- Blood loss: Acute or chronic blood loss will cause an increase in erythropoiesis.
Reticulocyte analysis, mainly immature reticulocyte fraction (IRF), has also been used in chemotherapy patients with leukemia to determine the regenerative activity of the bone marrow during and after treatment. This same idea applies to bone marrow transplant patients.[9]
Another clinical use of reticulocyte count is in patients taking hydroxyurea for sickle cell anemia. This medication impairs bone marrow production of reticulocytes, therefore, causing a decrease in the count. For this reason, frequent reticulocyte counts are necessary while on this medication.[10]
In end-stage renal disease patients receiving EPO therapy, the reticulocyte count has been used as a parameter to measure the response to therapy.[1]
Other values apart from reticulocyte count that can be calculated to assess function:
- Reticulocyte production index (RPI) = [%reticulocyte count x Patient Hct]/45(normal Hct)
- This is a corrected reticulocyte count used in anemias. In anemias, a falsely elevated reticulocyte count can occur. A decrease in RBCs automatically increases the reticulocyte count even if erythropoiesis has not taken place because the count represents a percentage in comparison to RBCs. It is possible the appropriate increase of erythropoiesis has not taken place in response to the anemia. This value, therefore, corrects for this issue.[2]
- Immature reticulocyte fraction (IRF): This is a value of the immature reticulocytes measured as a ratio of immature reticulocytes to the total amount of reticulocytes.[11]
- Reticulocyte hemoglobin content (Chr): This is a useful indirect measure of iron deficiency anemia. It measures the amount of iron available in the bone marrow that can be used by the reticulocyte for the production of hemoglobin. Multiple studies have shown a Chr of less than 28 pg is a good predictor for iron deficiency anemia.[12]
Media
(Click Image to Enlarge)
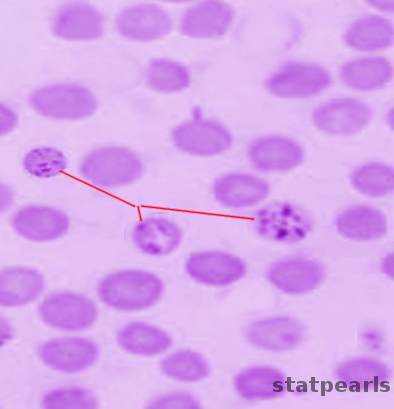
Reticulocytes Image courtesy Dr Chaigasame
References
Riley RS, Ben-Ezra JM, Goel R, Tidwell A. Reticulocytes and reticulocyte enumeration. Journal of clinical laboratory analysis. 2001:15(5):267-94 [PubMed PMID: 11574956]
Piva E, Brugnara C, Spolaore F, Plebani M. Clinical utility of reticulocyte parameters. Clinics in laboratory medicine. 2015 Mar:35(1):133-63. doi: 10.1016/j.cll.2014.10.004. Epub 2014 Nov 26 [PubMed PMID: 25676377]
Moras M, Lefevre SD, Ostuni MA. From Erythroblasts to Mature Red Blood Cells: Organelle Clearance in Mammals. Frontiers in physiology. 2017:8():1076. doi: 10.3389/fphys.2017.01076. Epub 2017 Dec 19 [PubMed PMID: 29311991]
Noulin F, Borlon C, van den Eede P, Boel L, Verfaillie CM, D'Alessandro U, Erhart A. Cryopreserved reticulocytes derived from hematopoietic stem cells can be invaded by cryopreserved Plasmodium vivax isolates. PloS one. 2012:7(7):e40798. doi: 10.1371/journal.pone.0040798. Epub 2012 Jul 23 [PubMed PMID: 22844411]
Mast AE, Blinder MA, Dietzen DJ. Reticulocyte hemoglobin content. American journal of hematology. 2008 Apr:83(4):307-10 [PubMed PMID: 18027835]
Riley RS, Ben-Ezra JM, Tidwell A, Romagnoli G. Reticulocyte analysis by flow cytometry and other techniques. Hematology/oncology clinics of North America. 2002 Apr:16(2):373-420, vii [PubMed PMID: 12094477]
Preloznik-Zupan I, Cernelc P, Zontar D. Reticulocyte analysis using light microscopy and two different flow cytometric procedures. Pflugers Archiv : European journal of physiology. 2000:440(5 Suppl):R185-7 [PubMed PMID: 11005665]
Koury MJ, Koury ST, Kopsombut P, Bondurant MC. In vitro maturation of nascent reticulocytes to erythrocytes. Blood. 2005 Mar 1:105(5):2168-74 [PubMed PMID: 15528310]
Level 3 (low-level) evidenceRaja-Sabudin RZ, Othman A, Ahmed-Mohamed KA, Ithnin A, Alauddin H, Alias H, Abdul-Latif Z, Das S, Abdul-Wahid FS, Hussin NH. Immature reticulocyte fraction is an early predictor of bone marrow recovery post chemotherapy in patients with acute leukemia. Saudi medical journal. 2014 Apr:35(4):346-9 [PubMed PMID: 24749130]
Level 2 (mid-level) evidenceAgrawal RK, Patel RK, Shah V, Nainiwal L, Trivedi B. Hydroxyurea in sickle cell disease: drug review. Indian journal of hematology & blood transfusion : an official journal of Indian Society of Hematology and Blood Transfusion. 2014 Jun:30(2):91-6. doi: 10.1007/s12288-013-0261-4. Epub 2013 May 24 [PubMed PMID: 24839362]
Chang CC, Kass L. Clinical significance of immature reticulocyte fraction determined by automated reticulocyte counting. American journal of clinical pathology. 1997 Jul:108(1):69-73 [PubMed PMID: 9208980]
Karagülle M, Gündüz E, Sahin Mutlu F, Olga Akay M. Clinical significance of reticulocyte hemoglobin content in the diagnosis of iron deficiency anemia. Turkish journal of haematology : official journal of Turkish Society of Haematology. 2013 Jun:30(2):153-6. doi: 10.4274/Tjh.2012.0107. Epub 2013 Jun 5 [PubMed PMID: 24385778]