Introduction
Retinoblastoma is an uncommon type of malignancy occurring in 1 per 18000 childbirths,[1] but it is the most commonly encountered primary intraocular malignancy of childhood and accounts for 3% cases of all childhood cancers.[2] It is also the second most prevalent intraocular malignant tumor after uveal melanoma. In specialized care centers, survival rates are up to 95% with retention of vision in most cases, but it is lower in developing countries. Retinoblastoma is composed of retinoblasts (basophilic cells with hyperchromatic nuclei and scanty cytoplasm). Mostly retinoblastomas are undifferentiated, but different degrees of differentiation are present owing to the formation of structures known as rosettes. The tumor can be endophytic (in vitreous) and seeding of tumor cells throughout the eye, or it can be exophytic (in subretinal space), or it can demonstrate a mixed presentation. Optic nerve invasion can occur with the spread of tumor in subarachnoid space and into the brain. Metastatic spread occurs in regional lymph nodes, liver, lungs, bones, and brain.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Retinoblastoma occurs as a result of a mutation in the RB1 tumor suppressor gene located at the long arm of chromosome 13 at locus 14 (13q14).[4] Formation of tumor occurs when both the copies of the RB1 gene are mutated. In the case of bilateral retinoblastoma, there are 98% chances that the mutation is germline. Only 5% of cases of retinoblastoma have a family history. 95% of retinoblastoma cases are sporadic, of which 60 % of patients have unilateral disease with no associated germline mutation. Remaining patients present with germline mutations along with the development of multiple tumors.
- Heritable
In this type of retinoblastoma, there is a mutation in one of the alleles of the RB1 gene in all body cells. When the second allele has a mutation as a result of some mutagenic event, it leads to the malignant transformation of cells. Due to the presence of the mutation in all cells, a large number of these children develop bilateral and multifocal retinoblastoma. Heritable disease patients are at significant risk of nonocular cancers such as pineoblastoma, osteosarcoma, soft tissue sarcomas, and melanomas: these malignancies usually occur in a particular age group.[5] The chances of second malignancy are 6%, but the risk increases five-fold when external beam radiation has been used to treat the primary tumor.
- Non-heritable
Non-heritable retinoblastomas are unilateral and are not transmitted. There is no risk of non-ocular cancers in these patients. In the case of unilateral retinoblastoma with no positive family history, it is non-heritable retinoblastoma, and the corresponding risk in each sibling and patient's offspring is 1%. Almost 90% of unilateral retinoblastomas cases are of the nonhereditary form.
Epidemiology
Retinoblastoma is the most commonly encountered primary intraocular tumor of childhood and accounts for 3% of all childhood tumors. It is also the second most common intraocular malignant tumor. The number of retinoblastoma cases ranges from 1 in 14000 to 1 in 20000 live births.[6] Three hundred new cases occur in the US per year. Retinoblastoma occurs equally in both sexes, and there is no sexual preference. Ninety percent of the cases present before the age of three years. Incidence of the disease is different in the various geographical regions.[7] Research shows six cases per million in Mexico and four cases per million in the US. India and Africa have the highest incidence.[2]
History and Physical
Presentation
Patients with retinoblastoma present mostly within the first year of age in the case of bilateral disease and within 3 years of age in case of unilateral disease. It is important to ask about family history of ocular malignancies. The most common presenting features are the following:
- Leucocoria: (whitish pupillary reflex): It is the most common presenting feature and accounts for 60% of cases.
- Strabismus: It is the second common presenting feature, and it is therefore important to perform fundus examination in all patients of childhood squint.
- Painful red eye: Painful red along with secondary glaucoma and associated buphthalmos can be present.
- Inflammation: Orbital inflammation resembling pre-septal or orbital cellulitis can also be a presenting feature.
- Visible extraocular growth
- Decreased vision
- Restriction of extraocular movements
- Metastatic disease: Metastatic disease involving lymph nodes, liver, lungs, brain, and bones is rare before ocular involvement.
Signs
- Intraretinal tumor: Intraretinal retinoblastoma is homogenous, dome-shaped whitish lesion along with calcification.
- Endophytic tumor: The endophytic tumor is present in vitreous as whitish lesion and seeds in the gel.
- Exophytic tumor: Presents as whitish subretinal mass, and it causes retinal detachment.
- Hypopyon
- Strabismus
- Hyphema
- Ocular inflammation
- Iris heterochromia
- Globe perforation
- Proptosis
- Cataract
- Glaucoma
- Anisocoria
Evaluation
- Direct Ophthalmoscopy
Red reflex testing with a direct ophthalmoscope is the simplest test, and leukocoria is easily observable. This method serves as a simple screening test.[8]
- Examination Under Anesthesia
Examination under anesthesia is necessary for measuring the corneal diameter, for tonometry, anterior chamber examination with a hand-held slit lamp, fundoscopy, cycloplegic refraction, and documenting all findings.
- Ultrasound
To assess the size of the tumor, to observe calcifications, and it also helps to rule out similar conditions like coats disease.
- Wide-Field Photography
Wide-field photography is used for analysis, documentation, and helps in the management of retinoblastoma.
- CT SCAN
CT scans help in the detection of calcifications, but due to radiation risks, it is avoided upon making the primary diagnosis.
- MRI
MRI is useful in the evaluation of optic nerve, extraocular extension, pineoblastoma, and to exclude similar diseases.[9]
- Systemic Assessment
This includes physical examination, MRI orbit and brain, bone scan, bone marrow aspiration, and lumbar puncture.
- Genetic Studies
Genetic studies of blood samples and tumor tissue from patient and relatives.[3][8]
Treatment / Management
Treatment of retinoblastoma involves a multidisciplinary approach involving an ophthalmologist, pediatric oncologist, ocular pathologist, geneticist, allied health professional, and parents. Different treatment modalities employed in the treatment of retinoblastoma are;
CHEMOTHERAPY is the mainstay of treatment. It is also used in combination with local therapies. Intravenous carboplatin, etoposide, and vincristine are used in three to six cycles depending upon the grade of retinoblastoma. Single carboplatin or dual agent therapy can also be used and has shown favorable results in selective patients such as bridging therapy to avoid aggressive measures. Intravitreal melphalan is used in cases of vitreous seeding although it carries a small risk of extraocular dissemination. Chemoreduction is followed by cryotherapy or transpupillary thermal therapy to maximize tumor control.
TTT (Transpupillary thermal therapy)is used mostly for focal consolidation after chemotherapy; however, it can be used as an isolated treatment. TTT has a direct effect but also augments the effects of chemotherapy.
CRYOTHERAPY: the triple freeze-thaw technique is an option for pre equatorial tumors without deeper invasion or vitreous seedings.
BRACHYTHERAPY is used for an anterior tumor when there is no vitreous seeding and in cases of resistance to chemotherapy.
EXTERNAL BEAM RADIOTHERAPY is avoided when possible, especially in the case of heritable retinoblastoma because it can result in a second malignancy. Retinoblastomas are radiosensitive, but adverse effects include cataract, radiation neuropathy, radiation retinopathy, and hypoplasia of orbit.[10]
ENUCLEATION: enucleation is performed when there is infiltration of the anterior chamber, neovascular glaucoma, invasion of the optic nerve, and if the tumor comprises more than half of the vitreous volume. It is also useful when chemotherapy has failed and in cases of diffuse retinoblastoma due to poor visual prognosis and a high risk of recurrence. Minimal manipulation should take place when performing enucleation, and a portion of the optic nerve of about 10 mm requires excision.[11] Recent advances in enucleation techniques now allow the removal of a long segment of the optic nerve under direct vision.[12](B3)
EXTRAOCULAR EXTENSION Adjuvant chemotherapy for 6 months is given following enucleation when there is retrolaminar or massive choroidal spread. When the extension of the tumor is up to the cut end of the optic nerve at enucleation, or it is through the sclera, then external beam radiation is used.
REVIEW careful follow-up at repeated intervals is required after treatment for early diagnosis of recurrence or development of new tumor, especially in patients with inherited disease.
Differential Diagnosis
The differential diagnosis of retinoblastoma includes diseases such as:
- Persistent anterior fetal vasculature
- Persistent posterior fetal vasculature
- Coats disease
- Retinopathy of prematurity
- Toxocariasis
- Uveitis
- Vitreoretinal dysplasia
- Coloboma of the choroid and optic disk
- Posterior cataract
Prognosis
Patients with intraocular retinoblastoma, particularly those who have access to modern health care facilities, have an excellent prognosis and an overall survival rate of more than 95% in developed countries. The most critical risk factor associated with poor prognosis is extraocular extension either through the sclera or through the invasion of the optic nerve. Patients who survive bilateral retinoblastoma are at an increased risk of developing non-ocular malignancies later in life the latent period for the development of the second tumor is usually 9 months. External beam radiotherapy decreases the latent period and increases the risk of the second malignancy in the first 30 years of life. The most prevalent type of second malignancy is a sarcoma. The survival of patients who have developed sarcoma is less than 50%.
Complications
If retinoblastoma is left untreated patient is likely to develop the following complications:
- Retinal detachment
- Retinal necrosis
- Orbital invasion
- Optic nerve invasion
- Blindness
- Intracranial extension
- Secondary neoplasms
- Metastasis
- Tumor recurrence
- Temporal bone hypoplasia
- Cataract
- Radiation neuropathy
- Radiation retinopathy
Enhancing Healthcare Team Outcomes
Retinoblastoma management is complex and requires an interprofessional team approach that includes an ophthalmologist, pediatric oncologist, ocular pathologist, geneticist, allied health professionals, and parents. In almost every case, the patient first presents to the nurse practitioner or primary care provider. Since this is a rare disorder that needs urgent attention, the patient should immediately obtain a referral to an ophthalmologist.
The cornerstone of long term retinoblastoma management is strict adherence to the treatment plan, and a careful follow up at repeated intervals is required after treatment for early diagnosis of recurrence or development of new tumor especially in patients with inherited disease.
Patients require education about the type of treatment, including chemotherapy, surgery, and radiation. The primary care providers should be familiar with the postoperative follow up of these patients and when to refer the patient back to the ophthalmologist.
Since chemotherapy is the mainstay of treatment, the involvement of a pharmacist with experience in oncologic treatment is essential. The pharmacist can verify agent selection, dosing, and perform medication reconciliation, reporting any concerns back to the healthcare team. Since nursing is most likely to be in charge of administering the chemo, a close rapport and open communication between pharmacy and nursing staff are crucial.
All patient management is best in consultation with an experienced ophthalmologist who will be able to provide appropriate support. For patients who adhere and to treatment plan and proper follow up, the prognosis is good.
Retinoblastoma is a challenging diagnosis to manage, and as such, requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and pharmacists, all collaborating across disciplines to achieve optimal patient results. [Level 5]
Media
(Click Image to Enlarge)
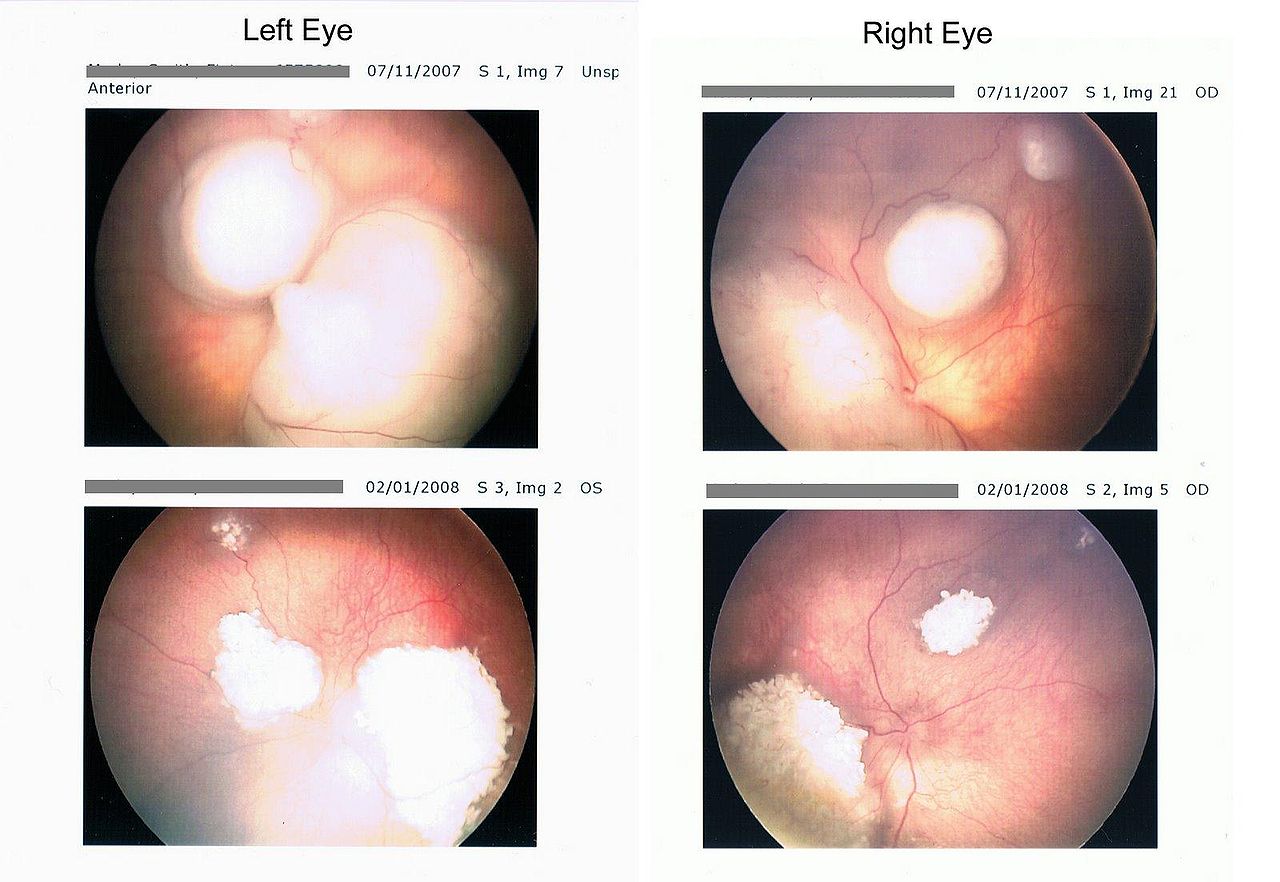
Retinoblastoma retina scan before and after chemotherapy Contributed by Wikimedia Commons
(Click Image to Enlarge)

Shows close-up of human face, straight on, showing both eyes, an example of a patient with retinoblastoma. Contributed by Wikimedia Commons (Public Domain)
(Click Image to Enlarge)
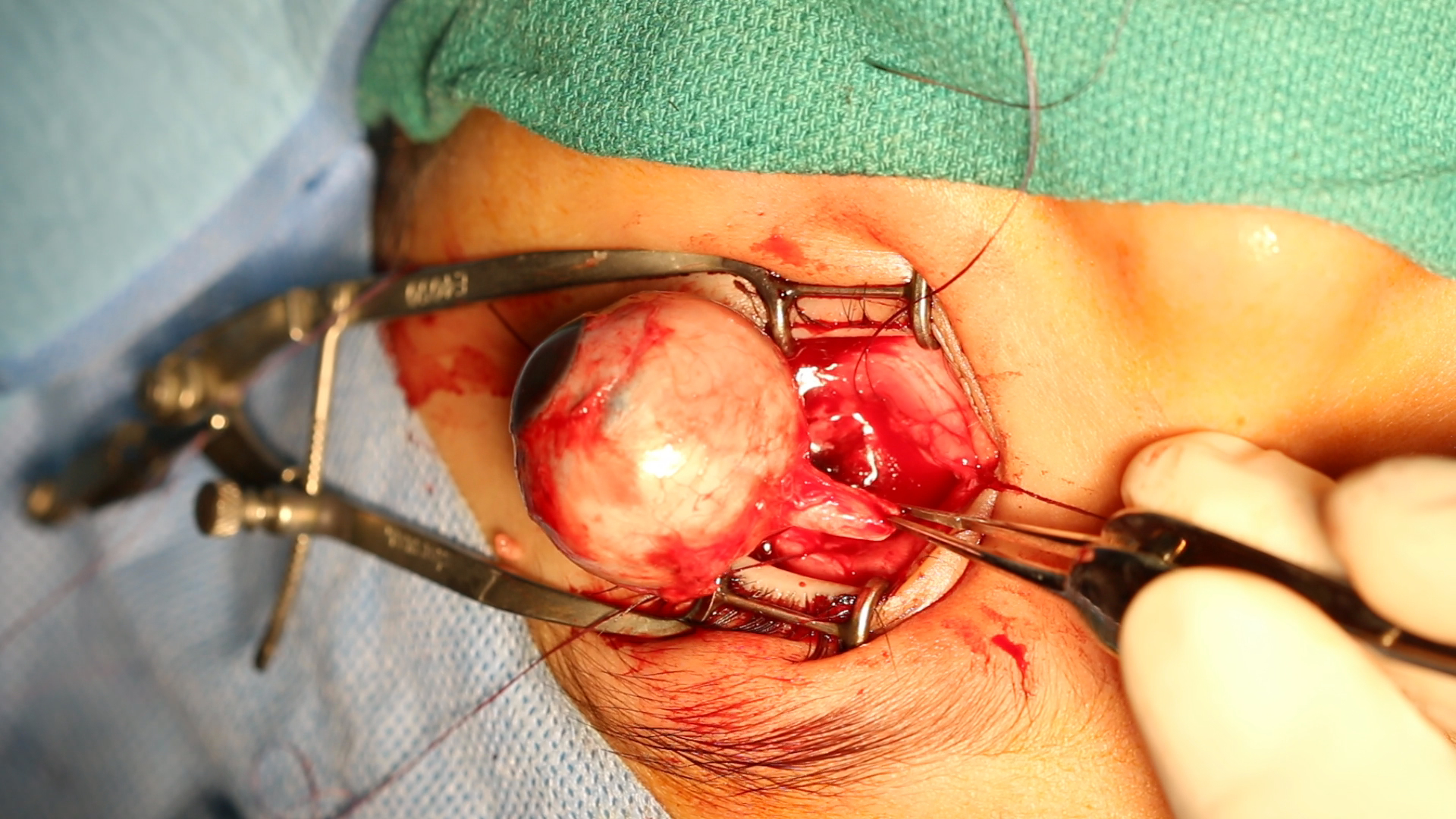
Enucleation: by using the separate supers-medial approach to the optic nerve, a good length of the optic nerve can be obtained as seen here. This is important with intraocular malignancies, especially large retinoblastomas Contributed by Professor Bhupendra C. K. Patel MD, FRCS
References
Mattosinho CCS, Moura ATMS, Oigman G, Ferman SE, Grigorovski N. Time to diagnosis of retinoblastoma in Latin America: A systematic review. Pediatric hematology and oncology. 2019 Mar:36(2):55-72. doi: 10.1080/08880018.2019.1605432. Epub 2019 Apr 24 [PubMed PMID: 31014139]
Level 1 (high-level) evidenceAlkatan HM, Al Marek F, Elkhamary S. Demographics of Pediatric Orbital Lesions: A Tertiary Eye Center Experience in Saudi Arabia. Journal of epidemiology and global health. 2019 Mar:9(1):3-10. doi: 10.2991/jegh.k.181224.001. Epub [PubMed PMID: 30932383]
Kletke SN, Feng ZX, Hazrati LN, Gallie BL, Soliman SE. Clinical Predictors at Diagnosis of Low-Risk Histopathology in Unilateral Advanced Retinoblastoma. Ophthalmology. 2019 Sep:126(9):1306-1314. doi: 10.1016/j.ophtha.2019.04.003. Epub 2019 Apr 12 [PubMed PMID: 30986443]
Zahn J, Chan MP, Wang G, Patel RM, Andea AA, Bresler SC, Harms PW. Altered Rb, p16, and p53 expression is specific for porocarcinoma relative to poroma. Journal of cutaneous pathology. 2019 Sep:46(9):659-664. doi: 10.1111/cup.13480. Epub 2019 May 3 [PubMed PMID: 31012122]
House RJ, Hsu ST, Thomas AS, Finn AP, Toth CA, Materin MA, Vajzovic L. Vascular Findings in a Small Retinoblastoma Tumor Using OCT Angiography. Ophthalmology. Retina. 2019 Feb:3(2):194-195. doi: 10.1016/j.oret.2018.09.018. Epub 2018 Sep 29 [PubMed PMID: 31014771]
Darwich R, Ghazawi FM, Rahme E, Alghazawi N, Burnier JV, Sasseville D, Burnier MN, Litvinov IV. Retinoblastoma Incidence Trends in Canada: A National Comprehensive Population-Based Study. Journal of pediatric ophthalmology and strabismus. 2019 Mar 19:56(2):124-130. doi: 10.3928/01913913-20190128-02. Epub [PubMed PMID: 30889267]
Liu Z, Yang Q, Cai N, Jin L, Zhang T, Chen X. Enigmatic Differences by Sex in Cancer Incidence: Evidence From Childhood Cancers. American journal of epidemiology. 2019 Jun 1:188(6):1130-1135. doi: 10.1093/aje/kwz058. Epub [PubMed PMID: 30834440]
Shafiq A. Seeing red in young children: the importance of the red reflex. The British journal of general practice : the journal of the Royal College of General Practitioners. 2015 Apr:65(633):209-10. doi: 10.3399/bjgp15X684625. Epub [PubMed PMID: 25824175]
Jenkinson H. Retinoblastoma: diagnosis and management--the UK perspective. Archives of disease in childhood. 2015 Nov:100(11):1070-5. doi: 10.1136/archdischild-2014-306208. Epub 2015 May 4 [PubMed PMID: 25940424]
Level 3 (low-level) evidenceElaraoud I, Ch'ng S, Karl D, Kalogeropoulos D, Chavan R, Sharma A. Management of retinal detachment in retinoblastoma with globe conserving treatment. Journal of current ophthalmology. 2019 Mar:31(1):43-48. doi: 10.1016/j.joco.2018.09.002. Epub 2018 Sep 22 [PubMed PMID: 30899845]
Schefler AC, Kim RS. Recent advancements in the management of retinoblastoma and uveal melanoma. F1000Research. 2018:7():. pii: F1000 Faculty Rev-476. doi: 10.12688/f1000research.11941.1. Epub 2018 Apr 18 [PubMed PMID: 29755733]
Pelton RW, Patel BC. Superomedial lid crease approach to the medial intraconal space: a new technique for access to the optic nerve and central space. Ophthalmic plastic and reconstructive surgery. 2001 Jul:17(4):241-53 [PubMed PMID: 11476174]
Level 3 (low-level) evidence