 Anatomy, Bony Pelvis and Lower Limb: Saphenous Nerve, Artery, and Vein
Anatomy, Bony Pelvis and Lower Limb: Saphenous Nerve, Artery, and Vein
Introduction
The saphenous nerve, artery, and vein are integral structures of a neurovascular bundle that courses through the thigh and leg of the lower limb. Firstly, the saphenous nerve is a strictly sensory nerve with no motor function.[1] It is responsible for innervation to the anteromedial aspect of the leg. The saphenous artery, a distant branch of the femoral artery arising from the descending genicular artery, is the predominant vascular supply to the surfaces of the knee. The saphenous vein (greater and lesser) returns blood from the superficial surfaces of the leg, emptying into the femoral vein proximally.[2][3]
Embryology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Embryology
During the gastrulation phase of the embryo, three germ layers are created—the ectoderm, endoderm, and mesoderm. The ectoderm itself is composed of two parts, the surface ectoderm, and the neuroectoderm. The neural crest, which derives from the neuroectoderm, gives rise to the peripheral nervous system which includes the saphenous nerve. On the other hand, the blood vessels that give rise to the saphenous artery and vein derive from the mesoderm. Although the blood vessels and nerves may originate from different germ layers, the vasculature corresponds with the consequent neuronal network. The Schwann cells that myelinate the peripheral nerves release vascular endothelial growth factor (VEGF) to stimulate the growth of the associated blood vessels of the neurovascular bundle.[4]
Blood Supply and Lymphatics
The saphenous artery typically branches from the descending genicular artery which originates from the medial wall of the femoral artery in the adductor canal. The saphenous artery, along with the saphenous nerve, travel under the sartorius muscle.[5] Once the saphenous artery is just proximal to the knee joint, there can be up to three cutaneous branches which supply the anterior and medial surfaces of the knee. Distal to the knee joint, there are more cutaneous branches to supply the anterior skin of the proximal third of the leg. The saphenous artery also has a muscular branch to supply to the sartorius muscle.[6]
The great saphenous vein is a subcutaneous vein that serves as the superficial vein of the leg. It initiates from the dorsal venous arch of the foot and runs anterior to the medial malleolus up to the medial aspect of the leg. It continues past the medial epicondyle of the femur to enter the saphenous opening where it drains into the femoral vein.[7][8][9]
Nerves
The saphenous nerve, the largest cutaneous branch of the femoral nerve, is derived from L3 and L4 of the lumbar plexus. This nerve has two major divisions known as the sartorial and infrapatellar nerves. These nerves together provide the sensory innervation to the medial, anteromedial, and posteromedial aspects of the distal thigh to the medial malleolus of the ankle joint. The saphenous nerve begins in the proximal thigh as a posterior division of the femoral nerve which lies laterally to the femoral artery. The saphenous nerve then tracks through the adductor canal where at this point, the saphenous nerve is now medial to the femoral artery. Upon exiting the adductor canal, the nerve divides into the sartorial and infrapatellar nerve branches at the level of the medial femoral condyle of the femur. The infrapatellar branch immediately travels anteriorly and innervates the anteroinferior and medial aspect of the knee.[10]
The sartorial branch continues to travel down the medial knee and behind the sartorius muscle. The sartorial branch then tracks more superficially as it penetrates through the fascia between the gracilis tendon and the sartorius tendon. At this point, the sartorial branch continues with the long saphenous vein to provide sensory innervation to the medial leg and ankle.[11][12][13]
Physiologic Variants
Ordinarily, the saphenous artery is a vascular branch of the descending geniculate artery that is supplied by the femoral artery. However, some anatomical studies have shown an absent descending genicular artery. In this case, the saphenous artery originates directly from the femoral artery. The saphenous vein also has a multitude of variants that typically subclassify into five different types. The types are dependent on the relationship on whether the vein splits and/or if their location is within the saphenous compartment at the level of the thigh.[14]
Surgical Considerations
The saphenous vein is of considerable surgical significance because of its ability to serve as a coronary artery bypass graft (CABG), especially when medical therapy or percutaneous intervention is ineffective or not performable. In terms of graft choices for CABG procedures, both arterial and venous grafts have been used, with the saphenous vein being the most commonly used venous graft for the bypass. However, in CABG procedures, arterial grafts are more widely used and preferred due to their prolonged patency. Studies have indicated that 10-year patency rates for saphenous vein grafts are at 61% compared to arterial bypass grafts such as the internal mammary artery at 85%.[15] Nevertheless, there have been cases where the saphenous vein has remained patent for over 30 years.[16]
The patency of the saphenous graft can be affected by a multitude of factors such as disruption of the vasa vasorum that supports the graft and tissue handling during the anastomoses of the graft. The mismatch between the compliance of the grafted vein at the site of the anastomosis to the coronary artery can cause a hemodynamic imbalance which promotes decreased patency of the venous graft.[17]
When harvesting the saphenous vein for CABG procedures, careful attention is necessary on delineating the saphenous vein from the saphenous nerve. Particularly in the inferior third of the leg, the saphenous nerve and vein are adhered together by a common fascia.[18] Due to its anatomical proximity in the lower third of the leg, there is a high incidence of saphenous neuralgia; this causes either hyperesthesia or diminished sensation in the distribution of the saphenous nerve.
Iatrogenic saphenous nerve injury
While saphenous neuropathy following trauma accounts for less than 1% of adult patients presenting with lower extremity pain[19], the literature notes variable rates of saphenous nerve injury following various orthopedic procedures. For example, a 2017 study reported varying degrees of sensory disturbances persisting up to and beyond 6-month follow-up in the majority of patients undergoing autograft hamstring (HS) harvesting during an anterior cruciate ligament (ACL) reconstruction procedure. The cohort consisted of oblique (n = 42) versus vertical (n = 36) incisional harvesting techniques, with 28 of 36 patients (77%) with the vertical incision experiencing sensory deficits at 6-months compared to 19 of 42 (45%) in the oblique incision cohort[20].
Depending on the technique used, the incidence of sensory disturbances in patients undergoing arthroscopic knee surgery has been reported as low as 0.06% up to as high as 77%.[21][22] With regards to meniscal repairs specifically, the reported range of saphenous nerve injury ranges from 1 to 20% of cases.[23][24]
The original belief was that the sartorial branch of saphenous nerve only becomes superficial at the medial joint line of the knee. So that during medical dissection of the knee, retraction of subcutaneous tissues would be protective of the sartorial branch of the saphenous nerve. However, there is anatomical variation where the saphenous nerve can become superficial above or below the joint line which can make it susceptible to injury during medial meniscus repairs.[25]
The saphenous artery also has significant surgical implications since a fasciocutaneous flap containing the saphenous artery can be elevated from the upper medial third of the leg and knee. These flaps can be utilized by reconstructive surgeons to cover defects of the upper extremities and exposed tibia after burns.[26]
Clinical Significance
Due to the saphenous nerve’s purely sensory function, a regional blockade of the nerve can be of sizeable clinical significance for procedures terminal to the knee. Nerve blocks for ankle manipulation, particularly around the medial malleolus would be an effective method of pain management during such procedures. Blocks would also be of benefit for meniscectomies due to the saphenous nerve’s course and location of innervation in the medial knee.[27]
The saphenous vein is also a commonly implicated vein in varicose veins that can lead to chronic venous disease. Structural changes can occur to the vein such as intimal wall thickening and increased connective tissue within the venous wall. The structural changes to the wall result in overall weakness and dilation of the vein which promotes reflux of flow. The reversal of flow can contribute to increased venous hypertension which promotes a continuous cycle of structural damage to the vein. Since the saphenous vein is a relatively superficial vein, it is often the vein that is visibly distended and problematic for the patient.[28]
Media
(Click Image to Enlarge)
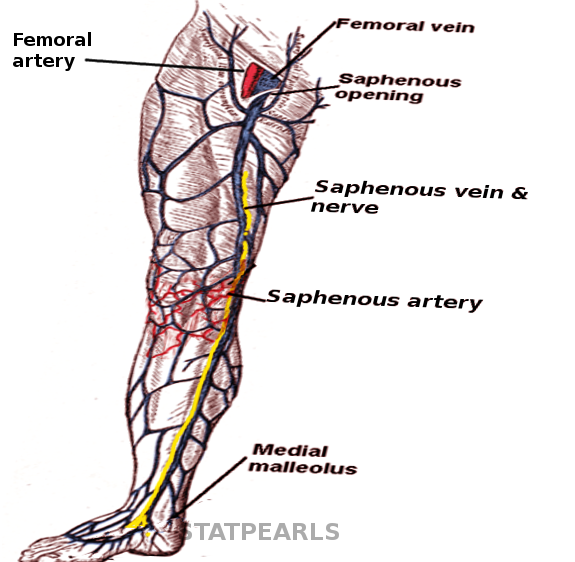
Saphenous neurovasculature Image courtesy S Bhimji MD
References
Ramage JL, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Medial Thigh Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30521196]
Bourne M, Talkad A, Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Foot Fascia. StatPearls. 2023 Jan:(): [PubMed PMID: 30252299]
Attum B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 29494052]
Uhl JF, Gillot C. Anatomy and embryology of the small saphenous vein: nerve relationships and implications for treatment. Phlebology. 2013 Feb:28(1):4-15 [PubMed PMID: 23256200]
Level 3 (low-level) evidenceWalters BB, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Sartorius Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30422484]
Xu Q, Zheng X, Li Y, Zhu L, Ding Z. Anatomical Study of the Descending Genicular Artery Chimeric Flaps. Journal of investigative surgery : the official journal of the Academy of Surgical Research. 2020 Jun:33(5):422-427. doi: 10.1080/08941939.2018.1532541. Epub 2019 Mar 19 [PubMed PMID: 30884993]
Caggiati A, Bergan JJ. The saphenous vein: derivation of its name and its relevant anatomy. Journal of vascular surgery. 2002 Jan:35(1):172-5 [PubMed PMID: 11802151]
Shah DM, Chang BB, Leopold PW, Corson JD, Leather RP, Karmody AM. The anatomy of the greater saphenous venous system. Journal of vascular surgery. 1986 Feb:3(2):273-83 [PubMed PMID: 3944931]
Cantrell AJ, Imonugo O, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Leg Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 30725709]
Hosahalli G, Sierakowski A, Venkatramani H, Sabapathy SR. Entrapment Neuropathy of the Infrapatellar Branch of the Saphenous Nerve: Treated by Partial Division of Sartorius. Indian journal of orthopaedics. 2017 Jul-Aug:51(4):474-476. doi: 10.4103/0019-5413.209954. Epub [PubMed PMID: 28790478]
Marsland D, Dray A, Little NJ, Solan MC. The saphenous nerve in foot and ankle surgery: its variable anatomy and relevance. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons. 2013 Jun:19(2):76-9. doi: 10.1016/j.fas.2012.10.007. Epub 2012 Dec 27 [PubMed PMID: 23548446]
Dayan V, Cura L, Cubas S, Carriquiry G. Surgical anatomy of the saphenous nerve. The Annals of thoracic surgery. 2008 Mar:85(3):896-900. doi: 10.1016/j.athoracsur.2007.11.032. Epub [PubMed PMID: 18291167]
Mercer D, Morrell NT, Fitzpatrick J, Silva S, Child Z, Miller R, DeCoster TA. The course of the distal saphenous nerve: a cadaveric investigation and clinical implications. The Iowa orthopaedic journal. 2011:31():231-5 [PubMed PMID: 22096447]
Ekin EE, Kurtul Yildiz H. The importance of great saphenous vein types and segmental aplasia in venous reflux. Journal of clinical ultrasound : JCU. 2017 Jul 8:45(6):332-336. doi: 10.1002/jcu.22457. Epub 2017 Feb 10 [PubMed PMID: 28186621]
Goldman S, Zadina K, Moritz T, Ovitt T, Sethi G, Copeland JG, Thottapurathu L, Krasnicka B, Ellis N, Anderson RJ, Henderson W, VA Cooperative Study Group #207/297/364. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: results from a Department of Veterans Affairs Cooperative Study. Journal of the American College of Cardiology. 2004 Dec 7:44(11):2149-56 [PubMed PMID: 15582312]
Ozcan AV, Evrengul H, Goksin I, Gur S, Kaftan A. 30-year patency of a saphenous vein graft in coronary bypass graft surgery. The Annals of thoracic surgery. 2008 Apr:85(4):e23. doi: 10.1016/j.athoracsur.2008.01.069. Epub [PubMed PMID: 18355484]
Level 3 (low-level) evidenceHarskamp RE, Lopes RD, Baisden CE, de Winter RJ, Alexander JH. Saphenous vein graft failure after coronary artery bypass surgery: pathophysiology, management, and future directions. Annals of surgery. 2013 May:257(5):824-33. doi: 10.1097/SLA.0b013e318288c38d. Epub [PubMed PMID: 23574989]
Level 3 (low-level) evidenceWilmot VV, Evans DJ. Categorizing the distribution of the saphenous nerve in relation to the great saphenous vein. Clinical anatomy (New York, N.Y.). 2013 May:26(4):531-6. doi: 10.1002/ca.22168. Epub 2012 Sep 19 [PubMed PMID: 22997057]
Pendergrass TL, Moore JH. Saphenous neuropathy following medial knee trauma. The Journal of orthopaedic and sports physical therapy. 2004 Jun:34(6):328-34 [PubMed PMID: 15233394]
Level 3 (low-level) evidenceSipahioglu S, Zehir S, Sarikaya B, Levent A. Injury of the infrapatellar branch of the saphenous nerve due to hamstring graft harvest. Journal of orthopaedic surgery (Hong Kong). 2017 Jan:25(1):2309499017690995. doi: 10.1177/2309499017690995. Epub [PubMed PMID: 28219309]
Figueroa D, Calvo R, Vaisman A, Campero M, Moraga C. Injury to the infrapatellar branch of the saphenous nerve in ACL reconstruction with the hamstrings technique: clinical and electrophysiological study. The Knee. 2008 Oct:15(5):360-3. doi: 10.1016/j.knee.2008.05.002. Epub 2008 Jun 26 [PubMed PMID: 18583136]
Level 2 (mid-level) evidencePortland GH, Martin D, Keene G, Menz T. Injury to the infrapatellar branch of the saphenous nerve in anterior cruciate ligament reconstruction: comparison of horizontal versus vertical harvest site incisions. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005 Mar:21(3):281-5 [PubMed PMID: 15756180]
Level 2 (mid-level) evidenceEspejo-Baena A, Golano P, Meschian S, Garcia-Herrera JM, Serrano Jiménez JM. Complications in medial meniscus suture: a cadaveric study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2007 Jun:15(6):811-6 [PubMed PMID: 16758232]
Plasschaert F, Vandekerckhove B, Verdonk R. A known technique for meniscal repair in common practice. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 1998 Nov-Dec:14(8):863-8 [PubMed PMID: 9848600]
Level 2 (mid-level) evidenceDunaway DJ, Steensen RN, Wiand W, Dopirak RM. The sartorial branch of the saphenous nerve: its anatomy at the joint line of the knee. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005 May:21(5):547-51 [PubMed PMID: 15891719]
Gocmen-Mas N, Aksu F, Edizer M, Magden O, Tayfur V, Seyhan T. The arterial anatomy of the saphenous flap: a cadaveric study. Folia morphologica. 2012 Feb:71(1):10-4 [PubMed PMID: 22532178]
Horn JL, Pitsch T, Salinas F, Benninger B. Anatomic basis to the ultrasound-guided approach for saphenous nerve blockade. Regional anesthesia and pain medicine. 2009 Sep-Oct:34(5):486-9. doi: 10.1097/AAP.0b013e3181ae11af. Epub [PubMed PMID: 19920424]
Level 2 (mid-level) evidenceLabropoulos N, Summers KL, Sanchez IE, Raffetto J. Saphenous vein wall thickness in age and venous reflux-associated remodeling in adults. Journal of vascular surgery. Venous and lymphatic disorders. 2017 Mar:5(2):216-223. doi: 10.1016/j.jvsv.2016.11.003. Epub 2017 Jan 16 [PubMed PMID: 28214490]