Introduction
Segond fractures are defined as an avulsion type fracture of the lateral proximal tibia at the attachment of the anterolateral ligament.[1] They are especially important because they are pathognomonic of a more complex knee injury, an anterior cruciate ligament (ACL) rupture.[2] Segond fractures confirmed on plain radiographs necessitate further evaluation and investigation to disprove concomitant knee injuries, as Segond fractures are almost never isolated injuries. The one exception to this is in the pediatric population, where Segond fractures are rarely noted to be isolated injuries. This is, however, not the norm, and even children should undergo thorough evaluation and investigation for knee ligamentous injury.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Segond fractures are usually caused by a forced mechanism of internal rotation with varus stress to the knee. It was first described by Paul Segond in his published works in 1879, following a cadaveric study of knee injuries.[2] This has later been correlated with ACL ruptures via the invention of more advanced imaging techniques. Segond also described a fibrous band at the point of the avulsion injury that has been defined as the anterolateral ligament.[4] More recent MRI studies however have been unable to identify any distinct ligamentous attachments associated with the anterolateral ligament, but do show evidence of posterior capsule and iliotibial band fibers attaching to the Segond fragment. These findings however are controversial.[5]
Epidemiology
Segond fractures have a high association with ACL ruptures, being present in 75% to 100% of cases. Conversely, 9-12% of ACL ruptures have an associated Segond fracture.[6][7]
ACL ruptures are a common orthopedic injury with an annual incidence of 68.6 per 100 000 people per year in the United States.[8] Incidence is slightly higher in male patients, with a peak incidence occurring later in men than in women - occurring in men aged 19-25 years of age with an incidence of 0.00241 and in women aged 14-18 with an incidence of 0.002276.
History and Physical
As Segond fractures have such a strong correlation with ACL ruptures, it is of no surprise that their history and mechanism of injury are also the same. Patients commonly describe a ‘pop’ following a twisting mechanism. They generally have an associated discomfort, swelling, decreased range of motion at the knee, and difficulty mobilizing.
There is no specific physical test for a Segond fracture, as they are generally noted on radiographs of the knee. However, as Segond fractures are often pathognomonic of ACL ruptures, testing for an intact ACL is imperative. Lachmann's test is the most sensitive physical examination maneuver in assessing for ACL tears, but there is also utility in the anterior drawer test. Integrity of all other ligaments of the knee should be assessed as well, including posterior drawer, varus/valgus stress testing, and pivot shift testing.
Evaluation
A Segond fracture can normally be diagnosed with a plain radiograph. A bony fragment (avulsion fracture) is seen in the anteroposterior view of the knee on the lateral aspect of the proximal tibia.
As previously discussed, with likely underlying ligamentous and or meniscal injuries, magnetic resonance imaging (MRI) is necessary for further evaluation, which may also highlight the more subtle Segond fractures.
Computed tomography is not usually used in the diagnosis of Segond fractures. While there is a much higher sensitivity for diagnosing fractures with CT Scan, MRI is the imaging modality of choice to identify the specific associated ligamentous injuries in the knees.
Treatment / Management
Initial treatment should be supportive. This includes resting the affected knee, elevating it whenever possible, simple analgesia, and icing the knee. Patients are highly likely to require walking aids, such as crutches. Having a knee brace early can also help support the knee before the consideration of surgery.
Surgical intervention is directed at underlying injuries rather than the Segond fracture itself. There is no evidence that Segond fractures need to be fixed. Furthermore, evidence suggests that ACL reconstructions are not at greater risk of failure with the presence of a Segond fracture.[9] While Segond fractures suggest higher instability associated with ligamentous knee injuries pre-operatively, the post-operative comparison suggests no difference in tested stability after the ligamentous injury is addressed.[10]
Direct repair of Segond fractures by repairing the anterolateral ligament is an option, as some suggest that it may restore rotational stability to the knee. Segond fractures can be repaired by either direct suture repair, suture anchor techniques, or screw fixation dependant on the size and characteristics of the fracture. Surgical repair of Segond fractures has shown good results with minimal complications, however, these were not compared to a control group.[2]
All surgical interventions should be undertaken following shared decision making with the patient and following informed consent. The decision to proceed with surgery is often largely swayed by the patient’s co-morbidities, activity levels, the patient’s expectations, and their likelihood of a favorable outcome.
Regardless of whether a patient elects for operative versus non-operative management, all patients need some form of rehabilitation from an interprofessional team approach. They will need to see a therapist for rehabilitation and may benefit from bracing to add stability and comfort to the knee.[11]
Differential Diagnosis
"Arcuate sign" is an avulsion fracture of the fibular head and is frequently mistaken for a Segond fracture on radiographs. The arcuate ligament complex or the posterolateral ligaments may avulse from the fibular head during a traumatic deformity to the knee. Like Segond fractures, this finding is pathognomonic for ligamentous knee injury and instability and should be investigated in a similar fashion. There are, however, subtle differences on plain radiographs, as an arcuate avulsion is normally more horizontal, lateral, and posterior than would be seen in a true Segond fracture.
Prognosis
The prognosis for a Segond fracture itself is good. As previously discussed, there has not been shown to be any benefit to fixing this fracture. Furthermore, the presence of Segond fractures do not appear to represent a higher risk of requiring revision surgery.[11] The main concern with regards to prognosis is appropriately addressing the associated ligamentous injuries in the knee. If addressed appropriately, patients will generally have a favorable outcome. Any alteration of the mechanics of the knee often leads to an increased risk of osteoarthritis (OA). It is well known that an ACL rupture leads to OA in a high proportion of patients. Unfortunately, ACL reconstruction has not been shown to completely reduce the risk of developing OA but has been shown to reduce its prevalence.[12]
Complications
The most common short-term complications from a Segond fracture are ongoing pain and stiffness. If the patient undergoes an ACL reconstruction, additional short to mid-term complications exist associated with the surgical procedure. Generally, however, ACL reconstruction is considered a safe procedure, with a 0.75% risk of a wound complication. Although thromboprophylaxis for ACL reconstruction is felt to be unnecessary, one paper has quoted deep vein thrombosis levels at 0.30% and pulmonary embolism levels at 0.18%.[13] The topic of thromboprophylaxis after ligamentous repair of the knee is controversial, and the decision to provide anticoagulation postoperatively should be made on a case by case basis by the surgeon considering each patient's specific medical comorbidities.
Deterrence and Patient Education
Patient education for Segond fractures and ACL ruptures is very challenging. Most injuries are caused by recreational or sporting injuries. Females, in particular, can decrease the risk of ligamentous injury to the knee by hamstring strengthening exercises and improved landing mechanics. Generally speaking, recreational activity should not be limited to prevent ligamentous injury, as exercise plays an important role in mental wellbeing and cardiovascular health.[14]
Enhancing Healthcare Team Outcomes
Segond fractures will require input from multiple members of the interprofessional team. Diagnosticians and radiologists must recognize Segond fractures and other avulsion fractures from the posterolateral corner of the knee as being pathognomonic for a more sinister soft tissue injury warranting further evaluation. Surgical repair of ligamentous injuries requires a dedicated OR team to optimize patient outcomes. Finally, therapists and surgeons must work together to provide the appropriate rehabilitation protocol for each individual patient to assist in maximal return to function. [Level V]
Media
(Click Image to Enlarge)
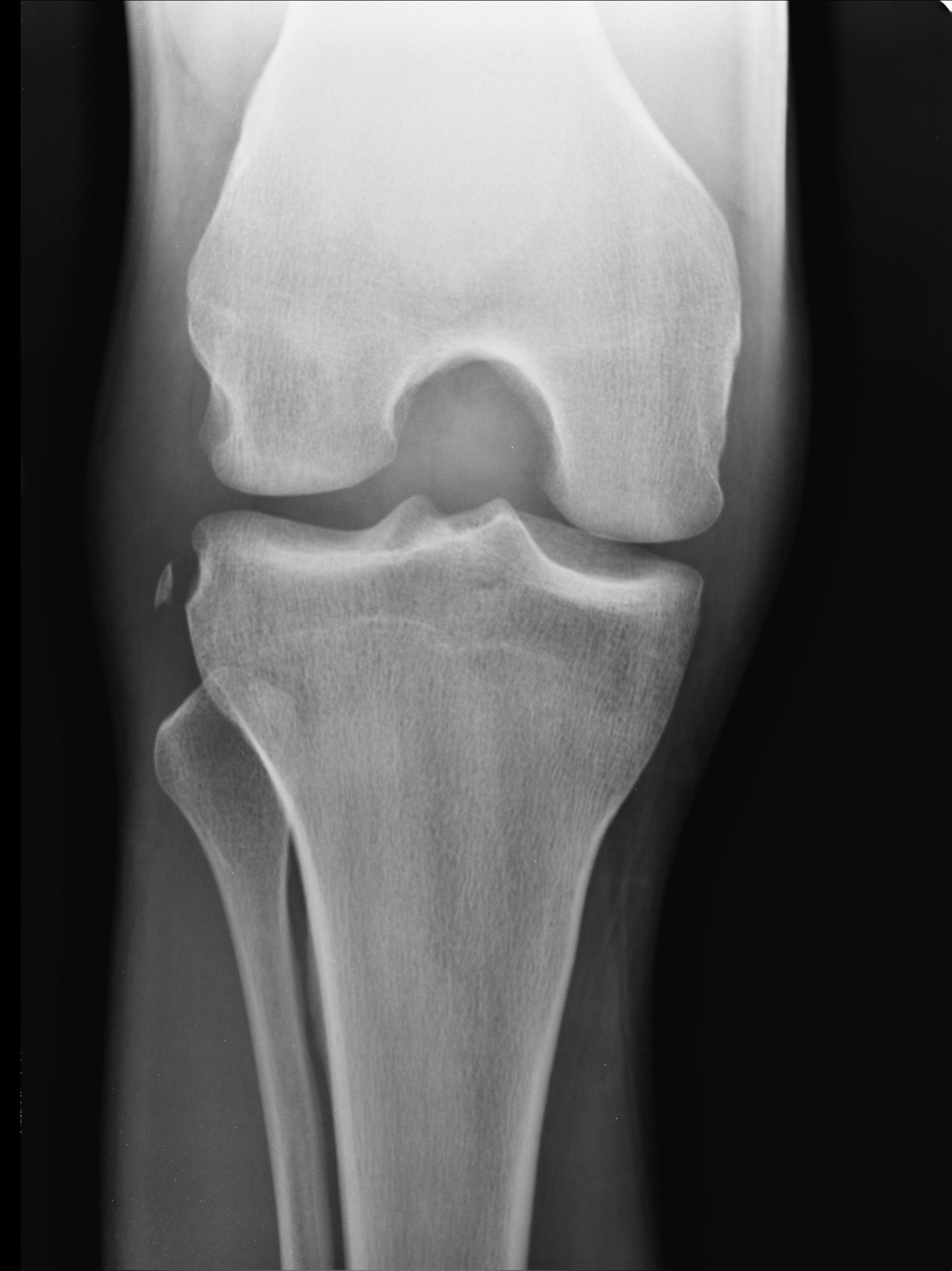
Segond fracture Case courtesy of Dr Maulik S Patel
References
Davis DS, Post WR. Segond fracture: lateral capsular ligament avulsion. The Journal of orthopaedic and sports physical therapy. 1997 Feb:25(2):103-6 [PubMed PMID: 9007767]
Ferretti A, Monaco E, Wolf MR, Guzzini M, Carli A, Mazza D. Surgical Treatment of Segond Fractures in Acute Anterior Cruciate Ligament Reconstruction. Orthopaedic journal of sports medicine. 2017 Oct:5(10):2325967117729997. doi: 10.1177/2325967117729997. Epub 2017 Oct 3 [PubMed PMID: 29051899]
Sferopoulos NK, Rafailidis D, Traios S, Christoforides J. Avulsion fractures of the lateral tibial condyle in children. Injury. 2006 Jan:37(1):57-60 [PubMed PMID: 16246341]
Level 3 (low-level) evidenceVincent JP, Magnussen RA, Gezmez F, Uguen A, Jacobi M, Weppe F, Al-Saati MF, Lustig S, Demey G, Servien E, Neyret P. The anterolateral ligament of the human knee: an anatomic and histologic study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2012 Jan:20(1):147-52. doi: 10.1007/s00167-011-1580-3. Epub 2011 Jun 30 [PubMed PMID: 21717216]
Shaikh H, Herbst E, Rahnemai-Azar AA, Bottene Villa Albers M, Naendrup JH, Musahl V, Irrgang JJ, Fu FH. The Segond Fracture Is an Avulsion of the Anterolateral Complex. The American journal of sports medicine. 2017 Aug:45(10):2247-2252. doi: 10.1177/0363546517704845. Epub 2017 May 12 [PubMed PMID: 28499093]
Arneja SS, Furey MJ, Alvarez CM, Reilly CW. Segond fractures: not necessarily pathognemonic of anterior cruciate ligament injury in the pediatric population. Sports health. 2010 Sep:2(5):437-9 [PubMed PMID: 23015973]
Yoon KH, Kim JS, Park SY, Park SE. The Influence of Segond Fracture on Outcomes After Anterior Cruciate Ligament Reconstruction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2018 Jun:34(6):1900-1906. doi: 10.1016/j.arthro.2018.01.023. Epub 2018 Feb 24 [PubMed PMID: 29487001]
Sanders TL,Maradit Kremers H,Bryan AJ,Larson DR,Dahm DL,Levy BA,Stuart MJ,Krych AJ, Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. The American journal of sports medicine. 2016 Jun; [PubMed PMID: 26920430]
Gaunder CL, Bastrom T, Pennock AT. Segond Fractures Are Not a Risk Factor for Anterior Cruciate Ligament Reconstruction Failure. The American journal of sports medicine. 2017 Dec:45(14):3210-3215. doi: 10.1177/0363546517726962. Epub 2017 Sep 26 [PubMed PMID: 28949245]
Melugin HP, Johnson NR, Wu IT, Levy BA, Stuart MJ, Krych AJ. Is Treatment of Segond Fracture Necessary With Combined Anterior Cruciate Ligament Reconstruction? The American journal of sports medicine. 2018 Mar:46(4):832-838. doi: 10.1177/0363546517745280. Epub 2017 Dec 29 [PubMed PMID: 29286825]
Slagstad I, Parkar AP, Strand T, Inderhaug E. Incidence and Prognostic Significance of the Segond Fracture in Patients Undergoing Anterior Cruciate Ligament Reconstruction. The American journal of sports medicine. 2020 Apr:48(5):1063-1068. doi: 10.1177/0363546520905557. Epub 2020 Mar 2 [PubMed PMID: 32119785]
Friel NA, Chu CR. The role of ACL injury in the development of posttraumatic knee osteoarthritis. Clinics in sports medicine. 2013 Jan:32(1):1-12. doi: 10.1016/j.csm.2012.08.017. Epub [PubMed PMID: 23177457]
Jameson SS, Dowen D, James P, Serrano-Pedraza I, Reed MR, Deehan D. Complications following anterior cruciate ligament reconstruction in the English NHS. The Knee. 2012 Jan:19(1):14-9. doi: 10.1016/j.knee.2010.11.011. Epub 2011 Jan 8 [PubMed PMID: 21216599]
Sadoghi P, von Keudell A, Vavken P. Effectiveness of anterior cruciate ligament injury prevention training programs. The Journal of bone and joint surgery. American volume. 2012 May 2:94(9):769-76. doi: 10.2106/JBJS.K.00467. Epub [PubMed PMID: 22456856]
Level 1 (high-level) evidence