 Anatomy, Shoulder and Upper Limb, Shoulder Muscles
Anatomy, Shoulder and Upper Limb, Shoulder Muscles
Introduction
The shoulder joint, also known as the glenohumeral joint, is a ball and socket joint with the most extensive range of motion in the human body. The shoulder muscles have a wide range of functions, including abduction, adduction, flexion, extension, internal and external rotation.[1] The central bony structure of the shoulder is the scapula, where all of the muscles interact. At the lateral aspect of the scapula is the articular surface of the glenohumeral joint, the glenoid cavity. The glenoid cavity is peripherally surrounded and reinforced by the glenoid labrum, shoulder joint capsule, supporting ligaments, and the myotendinous attachments of the rotator cuff muscles. The muscles of the shoulder play a critical role in providing stability to the shoulder joint. The primary muscle group that supports the shoulder joint is the rotator cuff muscles. The four rotator cuff muscles include the supraspinatus, infraspinatus, teres minor, and subscapularis.[2][1] Other muscles that form the shoulder girdle include the pectoralis major, pectoralis minor, the deltoids, trapezius, and the serratus anterior.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The upper extremity is attached to the axial skeleton by way of the sternoclavicular joint. The three joints of the pectoral girdle are the sternoclavicular joint, coracoclavicular joint, and acromioclavicular joint. The bones of the pectoral girdle are the clavicle, scapula, and humerus. The clavicle is positioned immediately superior to the first rib. The distal aspect of the clavicle articulates with the acromial process and coracoid process of the scapula, forming the acromioclavicular joint and coracoclavicular joints, respectively. The most important structural ligaments of the shoulder joint are the glenohumeral ligaments and the coracoacromial ligament.[3]
The scapula is a flat bone with multiple muscular attachments. The glenoid fossa serves the articulating function with the humeral head at the lateral angle of the scapula. The glenohumeral joint is the point of articulation between the humerus, the scapula, and the thoracic cavity, with the latter occurring through the scapulothoracic articulation. The scapula connects to the clavicle via the coracoclavicular joint and the acromioclavicular joint.
The coracoclavicular joint is strengthened by the coracoclavicular ligament that unites the undersurface of the clavicle to the coracoid process of the scapula. The acromioclavicular joint is at the lateral aspect of the clavicle and does not provide much structural support to the shoulder joint. The coracoid process, the acromion process, and the coracoacromial ligament provide peripheral reinforcement for the shoulder joint along with the muscles of the shoulder. The shoulder muscles and peripheral structures of the shoulder function to increase the structural integrity of the shoulder joint.[4]
Embryology
Embryologic development of the limbs begins at the end of the fourth week of fetal development. By the sixth week, the fetus develops hand plates and footplates. During limb development, the shape of the limb is formed by mesenchymal cells condensing and differentiating into chondrocytes which will ultimately differentiate into the bones and cartilage of the upper and lower extremity. The upper and lower extremities undergo very similar embryological development patterns. Limb musculature is first seen around the seventh week. The mesenchyme migrates from the dorsolateral cells of somites out to the limb and is differentiated into muscle cells. The shoulder muscles develop earlier than the distal muscles of the upper extremity.[5]
Blood Supply and Lymphatics
The arterial supply to the upper extremity originates from the subclavian artery. These vessels exist on both sides of the body to provide upper extremity blood supply. Both arteries receive their blood supply from the arch of the aorta. The subclavian artery branches on both sides of the body include the vertebral artery, internal thoracic artery, thyrocervical trunk, and dorsal scapular artery.
The subclavian artery becomes the axillary artery once it reaches the lateral border of the first rib.
There are three parts to the axillary artery, with each portion having arterial branches to supply the shoulder muscles. Multiple arteries branch from the axillary artery, including the superior thoracic artery, thoracoacromial artery, circumflex humeral artery, and the lateral thoracic artery. The subscapular artery is a division of the third part of the axillary artery. The subscapular artery gives off the circumflex scapular artery and the thoracodorsal artery. In general, the muscles of the shoulder receive vascular supply by named arteries associated with the muscles they supply.[6]
Efferent lymphatic vessels arise from the distal upper extremity and pass through the shoulder. Additionally, axillary lymph nodes contribute to efferent lymphatic vessels in the shoulder region and pass proximally through the shoulder. Deep lymphatic vessels accompany superficial lymphatic vessels. The deep lymphatic vessels drain lymph from the joint capsule, tendons, and nerves. The lymphatics of the shoulder and axillary region are drained by the subclavian lymphatic trunk. On the right, the subclavian trunk drains into the right lymphatic duct. On the left, the subclavian trunk drains into the thoracic duct.[7]
Nerves
The upper and lower branches of the subscapular nerve innervate the subscapularis muscle. The suprascapular nerve innervates the supraspinatus and infraspinatus muscles. The posterior branch of the axillary nerve supplies the teres minor. The axillary nerve also innervates the deltoid muscle. The nerve supply to the trapezius is by the spinal accessory nerve/11th cranial nerve with some direct branches from the cervical plexus. Innervation to levator scapula is by C3-C5. The nerve supply to the rhomboids is the dorsal scapular nerve. The nerve supply to the serratus anterior is the long thoracic nerve. The pectoralis major muscle receives its nerve supply via the medial and lateral pectoral nerves.[8]
Muscles
The primary muscle group that supports the shoulder joint is the rotator cuff muscles. The four rotator cuff muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. Together the rotator cuff muscles form a musculotendinous cuff as they insert on the proximal humerus.
The rotator cuff muscles attach to the proximal humerus anteriorly at the greater tuberosity. The rotator cuff muscles provide considerable structural support to the glenohumeral joint and keep the humeral head in a firm position by articulating with the scapula within the glenoid cavity. The muscles of the chest also provide structural support to the shoulder joint.[8]
The origin of the supraspinatus is from the supraspinatus fossa above the spine of the scapula crossing the shoulder joint, passing under the coracoacromial arch, and above the glenohumeral joint where it inserts at the greater tubercle of the humerus. The supraspinatus muscle functions by abduction of the humerus up to 30 degrees and stabilizing the glenohumeral joint.[8]
The infraspinatus muscle originates from the infraspinatus fossa below the spine of the scapula and inserts on the greater tubercle of the proximal humerus below the supraspinatus tendon. The infraspinatus muscle functions by externally rotating the humerus.
The teres minor muscle is positioned immediately inferior to infraspinatus, originating at the inferior aspect of the dorsal scapula at the lateral border of the scapula. The teres minor inserts on the greater tubercle of the humerus below the infraspinatus. The Teres minor acts to externally rotate the humerus and assists with abduction of the humerus.
The subscapularis originates from the subscapular fossa of the scapula and inserts on the lesser tubercle of the humerus as well as a portion of the anterior capsule of the shoulder joint. A large bursa separates the muscle from the neck of the scapula—the subscapularis functions by internally rotating and abducting the humerus.
The rhomboid minor originates from the nuchal ligament and spinous processes of C7-T1. The rhomboid major originates from the spinous processes of T2-T5. The rhomboid muscles insert on the medial border of the scapula and work in combination with the levator scapulae muscles to elevate the medial border of the scapula. The only muscle which acts to depress the shoulder is the lower trapezius, which is assisted by gravity in the upright position.[8]
The trapezius is a large triangular-shaped muscle that overlies the shoulder posteriorly. The trapezius originates from the superior aspect of the nuchal line in the occipital, cervical, and upper thoracic region and inserts at the lateral aspect of the clavicle, the acromion, and spine of the scapula. The function of the trapezius muscle is both elevation and depression of the shoulder depending on whether the upper or lower muscle fibers are activated. When the entire trapezius muscle contracts, the fibers are geometrically opposed, and the forces are balanced, resulting in no shoulder movement.
The deltoid muscle overlies the shoulder superficially and functions to abduct the humerus. The deltoid muscle has three origins; the body of the clavicle, the spine of the scapula, and the acromion. The deltoid muscle has its insertion on the deltoid tuberosity of the humerus. The function of the deltoid muscle is variable depending on which muscle fibers are activated. The anterior deltoid flexes and medially rotations the humerus, the middle deltoid abducts the humerus, and the posterior deltoid performs the actions of extension and external rotation of the humerus.[9]
The short head of the biceps brachii originates from the coracoid process, and the long head originates from the supraglenoid tubercle, passing through the intertubercular groove of the proximal humerus. The biceps brachii is not actually considered a shoulder muscle, but the tendon of its long head originates on the superior lip of the glenoid labrum.
Physiologic Variants
The infraspinatus muscle tendon is sometimes separated from the capsule of the shoulder joint by a bursa. An accessory muscle of the biceps brachii may be confused with a split tear along the biceps tendon. There is some variability of the location that the rotator cuff muscles insert on the proximal humerus.[10]
Surgical Considerations
Rotator cuff injuries and tendon degeneration result from multifactorial processes and pathological changes, both of which affect the quality of tendons.[11] A pathology affecting the rotator cuff muscles is common, and surgical intervention is routinely performed in patients who have failed conservative treatment for various pathologies, including full and partial-thickness rotator cuff tears and subacromial impingement syndrome. Subacromial decompression with rotator cuff debridement and acromioplasties are performed in cases of subacromial impingement and provide increased clearance for the supraspinatus tendon.[12]
Arthroscopic procedures can be used to access the shoulder joint and repair the rotator cuff muscles. Several port sites are used to access the joint, and they are made relative to bony landmarks and pass between or through the muscles of the shoulder. Posterior access is attained by making a port site that allows access to the joint by passing between the infraspinatus muscle and the teres minor muscle or directly through the infraspinatus muscle. Anterior access is obtained by passing a portal through the pectoralis major and the deltoid muscle. Lateral access is obtained by placing a portal directly through the deltoid muscle.
Surgical repair of individuals with partial-thickness rotator cuff tears refractory to conservative management as well as full-thickness cuff tears is typically done arthroscopically. The torn tendon(s) are repaired by anchoring them back to the humerus, their original insertion site.
Tendinopathies of the long head of the biceps tendon commonly co-occurs with rotator cuff pathologies and often contribute to shoulder pain. As the tendon attaches to the superior lip of the glenoid labrum, it is encountered during arthroscopic shoulder operations and is often included as a component of the operation. Biceps tendon tenotomy, or tendon release, is a common technique that clinicians can use to relieve pain caused by biceps tendinopathies. Tenodesis of the biceps tendon, or release and re-anchoring, is another technique used. There is some debate about which technique is superior.[13]
The functionality of the shoulder muscles is important when considering total shoulder replacement options. For example, reverse total shoulder arthroplasties are frequently used in individuals with poor rotator cuff function, but successful operation necessitates a functional deltoid muscle to allow for shoulder abduction.[14]
Clinical Significance
Rotator Cuff Injury
Rotator cuff tears are either partial-thickness or full-thickness tears. Partial-thickness tears most commonly occur at the articular or bursal side of the rotator cuff tendons. Full-thickness tears often involve some degree of tendon retraction. The patient's age, baseline shoulder function, tear size, chronicity, and degree of tendon retraction are several critical elements to be considered when deciding how to manage each patient most appropriately.[15][12]
The supraspinatus tendon is the most commonly injured tendon of the rotator cuff muscles, followed by infraspinatus, subscapularis, and teres minor. The teres minor tendon is only rarely involved in rotator cuff injuries. The subscapularis tendon tear can be associated with a biceps tendon dislocation from the bicipital tendon groove moving into the subscapularis tendon medially. Confirmation of intra-articular tendon tears is by the absence of the biceps tendon in the empty bicipital groove.[10]
Labral Injuries and Dislocations
Multiple types of shoulder labral injuries can occur in different patient populations. One particularly common injury subgroup includes young athletes afflicted with a traumatic shoulder dislocation. In the setting of glenohumeral instability, clinicians should recognize the importance of not only a recurrent dislocation but the risk of increased bone loss and soft tissue compromise, which may ultimately affect the outcome following surgical repair.
Glenohumeral instability, especially in the setting of trauma, is most commonly seen anteriorly. Posterior shoulder instability can be seen in weightlifters or football linemen. Rare dislocation patterns include the superior and inferior glenohumeral dislocation (luxatio erecta).
It is important to note that in the setting of multidirectional instability (MDI), especially in cases of bilateral ligamentous laxity or in a patient with a personal or family history of a connective tissue disorder, the probability of recurrent instability is relatively common. The mainstay treatment for these injuries centers on physical therapy and shoulder strengthening programs.
Para-labral cysts are most often seen in association with glenoid labral tears. Para-labral cyst formation can cause subsequent nerve compression and denervation of shoulder muscles. The suprascapular nerve is susceptible to compression from a para-labral cyst due to its location as it passes through the suprascapular and spinoglenoid notches adjacent to the anterior-inferior labrum. The subscapular nerve is also susceptible to compression from a para-labral cyst in the subscapular recess. Isolated atrophy of the teres minor implies injury to the axillary nerve.[16]
Adhesive Capsulitis
The cause of frozen shoulder is the deposition of hydroxyapatite crystals into the muscle-tendon. The shoulder is the most common site of hydroxyapatite calcification in the human body. The supraspinatus tendon is the most common site of hydroxyapatite crystal deposition. Frozen shoulder is associated with diabetes mellitus but may also be associated with coronary artery disease, cerebral vascular disease, rheumatoid arthritis, and thyroid disease.[17]
Subacromial Bursitis
Subacromial bursitis, specifically the acute phase, results in painful overhead movement. This is due to friction between the acromion and deltoid superiorly and the humeral head and supraspinatus inferiorly. Chronic bursitis leads to chronic pain because there is inflammation within the bursa. This inflammatory process can lead to weakness and rupture of the nearby ligaments and tendons. When confronted with chronic bursitis cases, it is also important to consider tendinitis since it can present simultaneously with bursitis.
Subacromial bursitis can be caused by repeated steroid injections as they increase the risk of infection within the shoulder and can also lead to damage to the rotator cuff muscles. Treatment most commonly consists of avoiding activities that include repetitive overhead movements, taking oral NSAIDs, and rest.[18]
Other Issues
An important imaging consideration in patients with previous orthopedic surgical repair of the shoulder and proximal humerus is metallic MRI artifacts. Performing MRIs at lower magnetic fields can decrease artifacts from implanted metal hardware.[19]
Media
(Click Image to Enlarge)
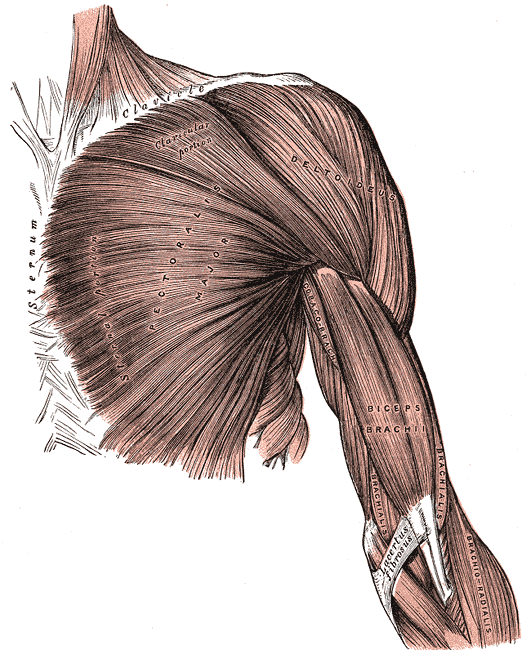
Superficial Muscles of the Chest and Shoulder. This illustration shows the pectoralis major, deltoid, coracobrachialis biceps brachii, brachialis, and brachioradialis. Other structures included in this image are the clavicle, sternum, and lacertus fibrosus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
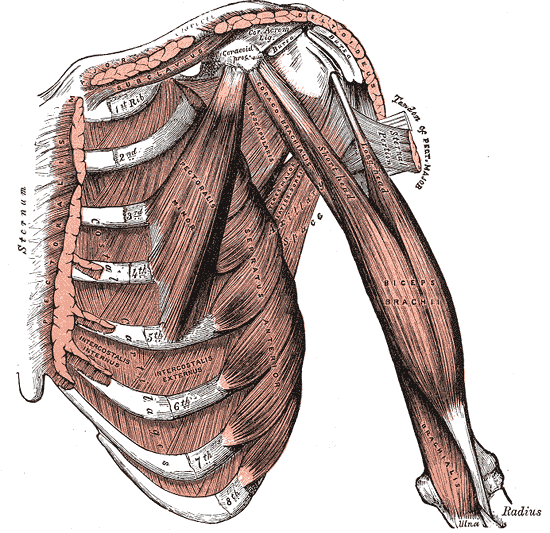
Internal Muscles of the Chest and Shoulder. The internal muscles of the chest and shoulder include the pectoralis, deltoid, subclavius, costal cartilages, ribs, pectoralis minor, serratus anterior, biceps brachii, coracobrachialis, and brachialis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
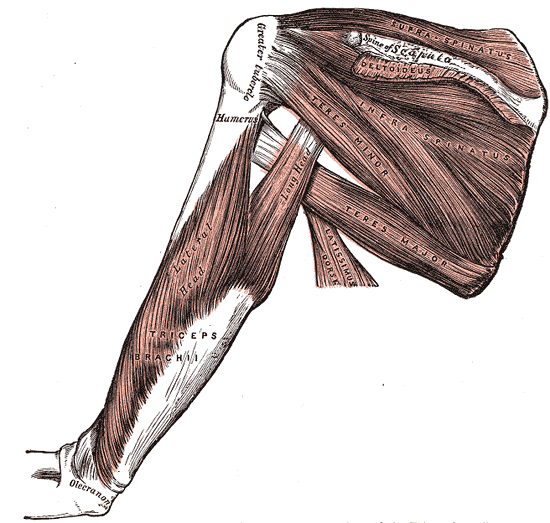
Muscles and Fascia of the Shoulder, Supraspinatus, Scapula, Humerus, Deltoid, Infraspinatus, Teres minor and major, Latissimus Dorsi, Triceps brachii,
Henry Vandyke Carter, Public domain, via Wikimedia Commons
References
Bakhsh W, Nicandri G. Anatomy and Physical Examination of the Shoulder. Sports medicine and arthroscopy review. 2018 Sep:26(3):e10-e22. doi: 10.1097/JSA.0000000000000202. Epub [PubMed PMID: 30059442]
Cowan PT, Mudreac A, Varacallo M. Anatomy, Back, Scapula. StatPearls. 2023 Jan:(): [PubMed PMID: 30285370]
Card RK, Lowe JB. Anatomy, Shoulder and Upper Limb, Elbow Joint. StatPearls. 2024 Jan:(): [PubMed PMID: 30422543]
Holt RG, Helms CA, Steinbach L, Neumann C, Munk PL, Genant HK. Magnetic resonance imaging of the shoulder: rationale and current applications. Skeletal radiology. 1990:19(1):5-14 [PubMed PMID: 2183366]
Warmbrunn MV, de Bakker BS, Hagoort J, Alefs-de Bakker PB, Oostra RJ. Hitherto unknown detailed muscle anatomy in an 8-week-old embryo. Journal of anatomy. 2018 Aug:233(2):243-254. doi: 10.1111/joa.12819. Epub 2018 May 3 [PubMed PMID: 29726018]
de la Garza O, Lierse W, Steiner D. Anatomical study of the blood supply in the human shoulder region. Acta anatomica. 1992:145(4):412-5 [PubMed PMID: 10457786]
Cuadrado GA, de Andrade MFC, Akamatsu FE, Jacomo AL. Lymph drainage of the upper limb and mammary region to the axilla: anatomical study in stillborns. Breast cancer research and treatment. 2018 Jun:169(2):251-256. doi: 10.1007/s10549-018-4686-1. Epub 2018 Jan 29 [PubMed PMID: 29380209]
Okwumabua E, Thompson JH. Anatomy, Shoulder and Upper Limb, Nerves. StatPearls. 2023 Jan:(): [PubMed PMID: 30252312]
Precerutti M, Garioni E, Madonia L, Draghi F. US anatomy of the shoulder: Pictorial essay. Journal of ultrasound. 2010 Dec:13(4):179-87. doi: 10.1016/j.jus.2010.10.005. Epub 2010 Nov 12 [PubMed PMID: 23396832]
Cook TS, Stein JM, Simonson S, Kim W. Normal and variant anatomy of the shoulder on MRI. Magnetic resonance imaging clinics of North America. 2011 Aug:19(3):581-94. doi: 10.1016/j.mric.2011.05.005. Epub [PubMed PMID: 21816332]
Plachel F, Moroder P, Gehwolf R, Tempfer H, Wagner A, Auffarth A, Matis N, Pauly S, Tauber M, Traweger A. Risk Factors for Rotator Cuff Disease: An Experimental Study on Intact Human Subscapularis Tendons. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2020 Jan:38(1):182-191. doi: 10.1002/jor.24385. Epub 2019 Jun 25 [PubMed PMID: 31161610]
Varacallo M, El Bitar Y, Mair SD. Rotator Cuff Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 30285401]
Friedman JL,FitzPatrick JL,Rylander LS,Bennett C,Vidal AF,McCarty EC, Biceps Tenotomy Versus Tenodesis in Active Patients Younger Than 55 Years: Is There a Difference in Strength and Outcomes? Orthopaedic journal of sports medicine. 2015 Feb [PubMed PMID: 26535382]
Familiari F, Rojas J, Nedim Doral M, Huri G, McFarland EG. Reverse total shoulder arthroplasty. EFORT open reviews. 2018 Feb:3(2):58-69. doi: 10.1302/2058-5241.3.170044. Epub 2018 Feb 28 [PubMed PMID: 29657846]
Varacallo M, El Bitar Y, Mair SD. Rotator Cuff Tendonitis. StatPearls. 2023 Jan:(): [PubMed PMID: 30335303]
Carroll KW, Helms CA, Otte MT, Moellken SM, Fritz R. Enlarged spinoglenoid notch veins causing suprascapular nerve compression. Skeletal radiology. 2003 Feb:32(2):72-7 [PubMed PMID: 12589484]
Level 3 (low-level) evidenceSuh CH, Yun SJ, Jin W, Lee SH, Park SY, Park JS, Ryu KN. Systematic review and meta-analysis of magnetic resonance imaging features for diagnosis of adhesive capsulitis of the shoulder. European radiology. 2019 Feb:29(2):566-577. doi: 10.1007/s00330-018-5604-y. Epub 2018 Jul 5 [PubMed PMID: 29978436]
Level 1 (high-level) evidenceFaruqi T, Rizvi TJ. Subacromial Bursitis. StatPearls. 2023 Jan:(): [PubMed PMID: 31082140]
Level 2 (mid-level) evidenceFahlenkamp UL,Gerhardt C,Hermann KG, [Magnetic resonance imaging findings after shoulder surgery: What the radiologist needs to know]. Der Radiologe. 2017 Nov [PubMed PMID: 29018890]