Introduction
Smith fracture is an eponym for a distal radius fracture with volar displacement or angulation of the distal fragment. This condition is also known as a reverse Colles fracture since the more common Colles fracture features a dorsally displaced distal fracture fragment (see Image. Colles Fracture Versus Smith Fracture).[1]
The wrist joint is a condyloid-type synovial joint. The distal tip of the radius and the articular disk (triangular ligament) of the distal radioulnar joint (DRUJ) articulate with the proximal carpal bones, except for the pisiform. The triangular fibrocartilage complex (TFCC) stabilizes the DRUJ and serves as a shock absorber in the wrist (radiocarpal) joint. The TFCC is composed of the triangular ligament, meniscus homolog, dorsal and volar radioulnar ligaments, ulnocarpal ligaments, and extensor carpi ulnaris (ECU) tendon sheath.
The ulna has a narrow attachment to the triangular ligament but not to any wrist bone, though it is a pivot point during pronation and supination. Most movement occurs around the radiocarpal articulation during flexion and extension.
A Smith fracture produces what is known as an "inverse dinner fork deformity." The median nerve and scaphoid bone can also get injured. The median nerve passes through the carpal tunnel anterior to the wrist. Median nerve injuries diminish hand sensorimotor function. Meanwhile, the scaphoid's poor vascularity predisposes it to slow healing, malunion, and nonunion.[2] DRUJ and TFCC disruption may also complicate volar displacement of the distal radius, leading to pain and weakness on the ulnar side of the forearm and wrist.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Distal radial fractures are often the result of a fall on an outstretched hand (FOOSH). Colles fractures frequently arise from a FOOSH mechanism. By comparison, Smith fractures commonly occur either as a fall onto a flexed wrist or as a direct blow to the dorsal aspect of the wrist. Volar displacement of the distal radius can also occur with a fall onto the palm.[4]
Epidemiology
The distal radius is the most commonly fractured site in the upper extremity. With over 600,000 cases annually in the United States alone, distal radial fractures account for more than 16% of all adult fractures and 75% of forearm fractures.[5][6][7] Distal radial fractures are the second most common fractures in older adults, next only to hip fractures. However, most distal radial fractures in this population are Colles fractures.[8] Smith fractures comprise approximately 5% of all radial and ulnar fractures combined, with the highest incidence in young men and older women. Almost all distal radius fractures arise in children sustaining high-energy falls or seniors with osteoporosis who suffer low-energy falls.[9]
Between the ages of 64 to 94, women are 6 times more likely than men to sustain a distal radial fracture.[10] Current evidence supports a direct correlation between low-energy, trauma-induced distal radius fracture and decreased bone mineral density.[11]
The Danish National Patient Registry records show a 31% increase in fractures among adult males from 1997 to 2018, mostly driven by the increasing population of older individuals. Increased surgical fixation rates have also been observed within this period, also attributed to the growing number of older patients.[12]
History and Physical
Smith fractures commonly result from trauma. As in any other trauma case, emergency conditions must be quickly ruled out before proceeding with a full workup. For example, open fractures and compartment syndrome require an immediate referral to an orthopedic specialist for emergency surgery.[13][14] The provider may proceed with a focused evaluation once emergency conditions have been ruled out.
History will reveal the patient falling on a flexed hand. Pain, swelling, deformity, and limited joint mobility develop shortly after the injury. Associated numbness or hand weakness suggests nerve involvement.
The physical exam may reveal a warm, tender distal forearm deformity, with edema visible on the volar side and the ulna protruding on the wrist dorsum. However, in some patients, the direction of angulation, whether dorsal (Colles) or volar (Smith), may be difficult to discern on visual inspection alone. The examiner may also elicit limitation of wrist joint movement.
Evaluation of the extremity's neurovascular status is imperative. Up to 15% of Smith fractures may show symptoms of acute carpal tunnel syndrome (ACTS) from median nerve compression.[15] Less commonly, both radial and ulnar nerves may also be compressed following a distal radius fracture.[16] Sensorimotor deficits in these nerves' distribution may be elicited on examination. Acute compartment syndrome may also develop, with signs referred to as the "5 Ps": pain, pallor, pulselessness, paresthesia, and paralysis. Neurovascular compromise warrants immediate surgical treatment.
Evaluation
Anteroposterior and lateral (APL) wrist X-rays are typically the initial imaging tests ordered. The images will reveal a distal radial fracture with volar angulation (see Image. Smith Fracture Radiography). The degree of displacement and angulation must be measured.
In some cases, a wrist radiograph series may be necessary to obtain other vital information about the fracture. This imaging test includes other wrist views besides APL and offers further information about carpal alignment, radiolunate and radioscaphoid stability, and the presence of carpal fractures and foreign bodies.[17] Computed tomography (CT) may be useful in evaluating comminuted and intra-articular fractures, serving as a surgical planning guide.
Treatment / Management
The goals of Smith fracture treatment are to restore alignment and prevent complications. Most of these injuries are not amenable to closed reduction and conservative management. Articular step-off of 2 mm or greater on post-reduction X-rays increases the risk of degenerative arthritis.[18] Besides considerable articular step-off after initial reduction, other indications for operative management include dorsal or volar comminution, intra-articular involvement, instability after initial reduction, surface angulation greater than 20°, and radial shortening greater than 5 mm.[19][20] If none of these features are present, conservative treatment may be attempted.(B2)
Conservative Approach
Closed reduction with subsequent immobilization is the mainstay of treatment of nondisplaced, stable distal radius fractures. Smith fractures require wrist reduction and splinting in extension, opposite the direction when reducing Colles fractures. Pain management during the procedure is given by procedural sedation, hematoma block, regional nerve block, intravenous regional (Bier) block, or general anesthesia.[21]
Evidence does not show any differences in stable distal radius fracture splinting methods.[22] However, research does not support the use of thermoplastic splints or braces on acute distal radius fractures.[23] Regardless of the chosen splinting method, the American Academy of Orthopaedic Surgeons (AAOS) recommends weekly radiographs for the first 3 weeks after reduction and before splint or cast removal. (A1)
A retrospective cohort analysis revealed that re-reduction of conservatively managed distal radius fractures did not significantly improve radiographic alignment or reduce the need for surgery. On the contrary, re-reduction may increase the need for surgery. Thus, alternative treatment options should be considered before attempting a Smith fracture re-reduction.[24] A randomized controlled trial found that 4 weeks of immobilization by casting adequately reduced distal radius fractures.[25](A1)
Surgical Management
Surgery may be considered when conservative management is not enough to reduce a Smith fracture. The choice of surgical approach depends on the injury's extent, degree of displacement, patient's age, occupation, and overall health.
The first option is closed reduction with percutaneous pinning (CRPP). Kirschner wires are minimally invasive, inexpensive, and associated with good functional outcomes for 2 or 3-segment fractures.[26] However, this technique is not recommended in comminuted fractures and the presence of bone-weakening conditions, such as osteoporosis. Complications include soft-tissue injury, pin migration, fracture settling, and pin site track infection.(B2)
The second option is external fixation. This technique utilizes ligamentotaxis, aligning the fracture fragments by tension applied to the surrounding soft tissues. With the advent of ORIF, the use of external fixation is now limited to reducing fractures in patients with multiple injuries (polytrauma) or initial management of open fractures with significant tissue loss.[27] However, Smith fractures are challenging to treat by external fixation due to the distal segment's volar displacement. The potential complications of this procedure include pin-track infection, pin loosening, and complex regional pain syndrome (CRPS), which may be due to carpal over-distraction.[28]
The third option is ORIF, currently the most commonly performed procedure for Smith fractures. ORIF using locking plates as implants is the best choice for an unstable or irreducible Smith fracture.[29] Internal fixation can be dorsal, volar, or fragment-specific. Cochrane reviews and AAOS do not recommend one method over the others. However, volar plating appears to be the most suitable for Smith fracture management, as it reduces extensor tendon rupture risk and preserves metaphyseal circulation.[30][31]
Dorsal plating has no role in Smith fracture management.[32] Meanwhile, fragment-specific fixation is typically more time-intensive and technically demanding, as it tailors the fixation technique to individual fracture patterns.(A1)
Carpal tunnel syndrome can arise as a Smith fracture complication. One study found that carpal tunnel release (CTR) is performed with distal-radius ORIF in 4.2% of cases. Intra-articular fractures with multiple fragments are associated with higher CTR rates, while being underweight, male, and of advanced age are linked to lower CTR rates.[33]
The ulnar styloid process can also be injured with distal radius fractures. Evidence shows that conservative and surgical management do not significantly differ in reducing ulnar-sided wrist pain and improving functional outcomes in patients with combined distal radial and ulnar styloid fractures. However, nonoperative management is associated with a higher risk of nonunion, which can negatively impact functional outcomes. Additionally, the severity of preoperative displacement was found to be a key factor in predicting ulnar styloid nonunion. Healthcare providers can use this information as a guide when deciding the management of combined distal radial and ulnar styloid fractures.[34] Patients require a period of immobilization and therapy to regain wrist strength and function.
Differential Diagnosis
The differential diagnosis of forearm deformity and pain secondary to trauma includes the following:[35]
- Colles fracture - extra-articular distal radius fracture with dorsal displacement or angulation
- Barton fracture - intra-articular distal radius fracture with dorsal displacement or angulation
- Reverse Barton fracture - intra-articular distal radius fracture with volar displacement or angulation
- Die-punch fracture - fracture of the radial articular surface with depression of the lunate facet
- Chauffer’s fracture - radial styloid avulsion fracture
- DRUJ disruption- injury to the sigmoid notch of the radius and the lunate facet
- TFCC tear - damage to the cartilaginous structure on the ulnar aspect of the wrist
- Galeazzi Fracture - fracture to the distal third of the radius with DRUJ disruption
Differentiating between these conditions and a Smith fracture entails a thorough physical examination, imaging studies, and prudent clinical judgment. Consultation with an orthopedic specialist may be necessary for diagnostic precision and appropriate management.
Staging
Smith fractures are classified into 3 types, based on the degree of articular involvement:
- Type I - Extra-articular distal radial fracture, which involves only the distal radius. This condition accounts for about 85% of cases.
- Type II - Intra-articular oblique fracture, also known as the reverse Barton fracture, which involves the dorsal radial articular surface. This injury comprises approximately 13% of cases.
- Type III - Juxta-articular oblique fracture, which extends into the radiocarpal (wrist) joint. This least common but most severe type comprises less than 2% of cases.
Smith fracture complexity generally impacts management and clinical outcomes.
Prognosis
Patients appropriately treated with a closed reduction have good outcomes, with functional healing around 6 weeks. Meanwhile, evidence does not support early mobility for improving long-term postoperative outcomes. However, the combination of stable fixation, edema management, early mobility with rehabilitation, and functional bracing is essential for athletes to return early to sport.[36]
Complications
Smith fractures produce complications that can impact cosmetic and functional outcomes if inappropriately treated. One of these complications is malunion, which may occur as a residual volar displacement or shortening of the distal radius. A malunion can result in a cosmetic abnormality known as the garden spade deformity.
Malunions may also narrow the carpal tunnel, resulting in delayed carpal tunnel syndrome. In older individuals, decreased bone density is a risk for malunion due to difficulty maintaining closed reduction.[37] Patients of advanced age have been reported to have a 50% malunion rate after a closed reduction.[38]. Osteotomy can improve function and appearance in malunited bones.[39]
Median nerve compression may result from volar angulation of the distal radius, though it may also arise from conservative management with excessive flexion or extension.[40] A less common complication after distal radius trauma is extensor pollicis longus (EPL) tendon entrapment with malunion, which may occur after both conservative treatment and ORIF.[41][42][43] Late EPL rupture is also commonly cited in the literature.[44][45]
De Quervain synovitis is another possible complication of Smith fractures. The risk factors include high-energy fracture patterns and poor response to corticosteroid injections. Patients nonoperatively treated for distal radial fractures are more likely to develop this complication than those who have undergone surgery. Both groups have a higher risk of developing de Quervain synovitis than the general population.[46]
CRPS has also been reported in up to 40% of distal radius fractures.[47] A recent meta-analysis reported that fractures with greater complexity or associated tissue damage, the female sex, a high BMI, and psychiatric disorders were risk factors for the development of CRPS in patients who sustained distal radial injuries.[48]
Postoperative and Rehabilitation Care
Stable fractures are typically immobilized for 4 to 8 weeks. The patient then undergoes rehabilitation and bracing for another 4 to 6 weeks until pain-free range of motion and normal strength have been achieved. Unstable fractures are often immobilized for 6 to 12 weeks, then rehabilitated until full motion and strength are regained.[49]
Pain management is always a concern in the postoperative period. One study showed that transdermal buprenorphine and codeine-acetaminophen provided superior pain control than celecoxib post-ORIF, improving treatment compliance and functional recovery.[50] However, clinicians should try to limit opioid use beyond the acute postoperative period. An interprofessional strategy—involving the operative team and primary care physician—may be employed when managing pain during the postoperative period. The AAOS recommends vitamin D supplementation to prevent CRPS in patients with a distal radial fracture.
Deterrence and Patient Education
Preventing a Smith fracture involves minimizing the risk of falls or traumatic injuries that could result in this type of wrist fracture. While it's not always possible to prevent traumatic events, providers can teach patients certain measures that may help reduce the risk of these injuries.
The first is to implement fall prevention strategies at home. Installing handrails on stairs, using non-slip flooring material, ensuring proper lighting, removing tripping hazards, and encouraging household members to wear the appropriate footwear are some measures that may help. The second is to comply with safety guidelines at work. Wearing the appropriate gear, avoiding hazardous areas, and following machine operation safety protocols are essential. People engaging in high-risk sports must execute movement patterns cautiously during games and condition their bodies in between.
The third is maintaining bone health. Bone resiliency can be achieved with the right diet and weight-bearing exercises. The fourth is environment assessment. Patients must avoid activities and locations that put them at risk of injuries. As a form of secondary prevention, patients must be advised to seek treatment for traumatic injuries immediately to minimize complications.
Enhancing Healthcare Team Outcomes
Smith fractures are best managed by a multidisciplinary team to ensure excellent outcomes. The members of this team include the following:
- Emergency medicine physician - Most patients with Smith fractures present first to the emergency department. The emergency medicine physician is the first health provider these patients encounter. The emergency medicine physician will order the patient's initial imaging tests and treatments. These providers will coordinate with the radiologist to properly interpret imaging tests and refer the patient to an orthopedic surgeon once stable.
- Radiologist - This provider will evaluate imaging test results and recommend further diagnostic imaging if needed.
- Orthopedic surgeon - This specialist will administer nonsurgical and surgical treatment to patients with Smith fractures.
- Pain management specialist - This professional will provide the appropriate pain management modality during reductive procedures. They may also be consulted in the postoperative period if patients require better pain control.
- Vascular surgeon - Referrals to these specialists may be necessary if the Smith fracture is accompanied by severe vascular injury.
- Nursing staff - The nurses will coordinate care, administer medications, help with patient education, and ensure patient comfort. Nurses are present in every phase of care for patients with Smith fractures.
- Physical therapists - These providers will help patients regain upper limb range of motion, strength, and function so they can resume normal routines.
- Occupational therapist - This specialist helps patients become more functionally independent as they recover from the injury.
- Pharmacist - This professional will coordinate with clinicians about medication prescriptions, dispense medications, and educate patients on proper medication intake.
- Primary care physician - This provider will render outpatient care, monitor rehabilitation progress, and educate patients on recurrence prevention.
Open communication among the interprofessional team members can reduce morbidity from Smith fractures.
Media
(Click Image to Enlarge)

Smith Fracture Radiography. Posteroanterior and lateral (PAL) view of a type I right Smith fracture.
Image courtesy of the Muneeb Shah (CC By 4.0 https://creativecommons.org/licenses/by/4.0/deed.en ) https://commons.wikimedia.org/wiki/File:11751_2012_127_Fig1_HTML.jpg
(Click Image to Enlarge)
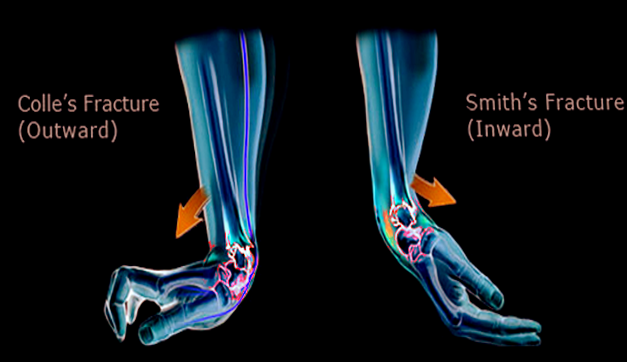
Colles Fracture Versus Smith Fracture. This illustration shows the different mechanisms giving rise to Colles and Smith fractures. Colles fractures arise from falling on an outstretched hand. In contrast, Smith fractures are caused by falling on a flexed hand.
Image courtesy O.Chaigasame
References
Shah HM, Chung KC. Robert William Smith: his life and his contributions to medicine. The Journal of hand surgery. 2008 Jul-Aug:33(6):948-51. doi: 10.1016/j.jhsa.2007.12.020. Epub [PubMed PMID: 18656770]
Omokawa S, Iida A, Fujitani R, Onishi T, Tanaka Y. Radiographic Predictors of DRUJ Instability with Distal Radius Fractures. Journal of wrist surgery. 2014 Feb:3(1):2-6. doi: 10.1055/s-0034-1365825. Epub [PubMed PMID: 24533238]
MILLS TJ. Smith's fracture and anterior marginal fracture of radius. British medical journal. 1957 Sep 14:2(5045):603-5 [PubMed PMID: 13460329]
Matsuura Y, Rokkaku T, Kuniyoshi K, Takahashi K, Suzuki T, Kanazuka A, Akasaka T, Hirosawa N, Iwase M, Yamazaki A, Orita S, Ohtori S. Smith's fracture generally occurs after falling on the palm of the hand. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2017 Nov:35(11):2435-2441. doi: 10.1002/jor.23556. Epub 2017 Apr 7 [PubMed PMID: 28262985]
Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. The Journal of hand surgery. 2001 Sep:26(5):908-15 [PubMed PMID: 11561245]
ALFFRAM PA, BAUER GC. Epidemiology of fractures of the forearm. A biomechanical investigation of bone strength. The Journal of bone and joint surgery. American volume. 1962 Jan:44-A():105-14 [PubMed PMID: 14036674]
Owen RA, Melton LJ 3rd, Johnson KA, Ilstrup DM, Riggs BL. Incidence of Colles' fracture in a North American community. American journal of public health. 1982 Jun:72(6):605-7 [PubMed PMID: 7072880]
Vannabouathong C, Hussain N, Guerra-Farfan E, Bhandari M. Interventions for Distal Radius Fractures: A Network Meta-analysis of Randomized Trials. The Journal of the American Academy of Orthopaedic Surgeons. 2019 Jul 1:27(13):e596-e605. doi: 10.5435/JAAOS-D-18-00424. Epub [PubMed PMID: 31232797]
Level 1 (high-level) evidenceLawson GM, Hajducka C, McQueen MM. Sports fractures of the distal radius--epidemiology and outcome. Injury. 1995 Jan:26(1):33-6 [PubMed PMID: 7868207]
Singer BR, McLauchlan GJ, Robinson CM, Christie J. Epidemiology of fractures in 15,000 adults: the influence of age and gender. The Journal of bone and joint surgery. British volume. 1998 Mar:80(2):243-8 [PubMed PMID: 9546453]
Hung LK, Wu HT, Leung PC, Qin L. Low BMD is a risk factor for low-energy Colles' fractures in women before and after menopause. Clinical orthopaedics and related research. 2005 Jun:(435):219-25 [PubMed PMID: 15930942]
Level 2 (mid-level) evidenceViberg B, Tofte S, Rønnegaard AB, Jensen SS, Karimi D, Gundtoft PH. Changes in the incidence and treatment of distal radius fractures in adults - a 22-year nationwide register study of 276,145 fractures. Injury. 2023 Jul:54(7):110802. doi: 10.1016/j.injury.2023.05.033. Epub 2023 May 10 [PubMed PMID: 37211473]
Duckworth AD, Mitchell SE, Molyneux SG, White TO, Court-Brown CM, McQueen MM. Acute compartment syndrome of the forearm. The Journal of bone and joint surgery. American volume. 2012 May 16:94(10):e63. doi: 10.2106/JBJS.K.00837. Epub [PubMed PMID: 22617929]
Level 2 (mid-level) evidenceMcQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk? The Journal of bone and joint surgery. British volume. 2000 Mar:82(2):200-3 [PubMed PMID: 10755426]
Level 2 (mid-level) evidenceFord DJ, Ali MS. Acute carpal tunnel syndrome. Complications of delayed decompression. The Journal of bone and joint surgery. British volume. 1986 Nov:68(5):758-9 [PubMed PMID: 3782239]
Level 3 (low-level) evidenceMcKay SD, MacDermid JC, Roth JH, Richards RS. Assessment of complications of distal radius fractures and development of a complication checklist. The Journal of hand surgery. 2001 Sep:26(5):916-22 [PubMed PMID: 11561246]
Dóczi J, Springer G, Renner A, Martsa B. Occult distal radial fractures. Journal of hand surgery (Edinburgh, Scotland). 1995 Oct:20(5):614-7 [PubMed PMID: 8543866]
Level 2 (mid-level) evidenceKnirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. The Journal of bone and joint surgery. American volume. 1986 Jun:68(5):647-59 [PubMed PMID: 3722221]
Level 2 (mid-level) evidenceSchneppendahl J, Windolf J, Kaufmann RA. Distal radius fractures: current concepts. The Journal of hand surgery. 2012 Aug:37(8):1718-25. doi: 10.1016/j.jhsa.2012.06.001. Epub 2012 Jul 3 [PubMed PMID: 22763062]
Jupiter JB, Fernandez DL, Toh CL, Fellman T, Ring D. Operative treatment of volar intra-articular fractures of the distal end of the radius. The Journal of bone and joint surgery. American volume. 1996 Dec:78(12):1817-28 [PubMed PMID: 8986658]
Level 2 (mid-level) evidenceMauck BM, Swigler CW. Evidence-Based Review of Distal Radius Fractures. The Orthopedic clinics of North America. 2018 Apr:49(2):211-222. doi: 10.1016/j.ocl.2017.12.001. Epub [PubMed PMID: 29499822]
Bong MR, Egol KA, Leibman M, Koval KJ. A comparison of immediate postreduction splinting constructs for controlling initial displacement of fractures of the distal radius: a prospective randomized study of long-arm versus short-arm splinting. The Journal of hand surgery. 2006 May-Jun:31(5):766-70 [PubMed PMID: 16713840]
Level 1 (high-level) evidenceLichtman DM, Bindra RR, Boyer MI, Putnam MD, Ring D, Slutsky DJ, Taras JS, Watters WC 3rd, Goldberg MJ, Keith M, Turkelson CM, Wies JL, Haralson RH 3rd, Boyer KM, Hitchcock K, Raymond L. Treatment of distal radius fractures. The Journal of the American Academy of Orthopaedic Surgeons. 2010 Mar:18(3):180-9 [PubMed PMID: 20190108]
Hoffer AJ, St George SA, Banaszek DK, Roffey DM, Broekhuyse HM, Potter JM. If at first you don't succeed, should you try again? The efficacy of repeated closed reductions of distal radius fractures. Archives of orthopaedic and trauma surgery. 2023 Aug:143(8):5095-5103. doi: 10.1007/s00402-023-04904-z. Epub 2023 May 13 [PubMed PMID: 37178164]
Elbardesy H, Yousaf MI, Reidy D, Ansari MI, Harty J. Distal radial fractures in adults: 4 versus 6 weeks of cast immobilisation after closed reduction, a randomised controlled trial. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2023 Dec:33(8):3469-3474. doi: 10.1007/s00590-023-03574-2. Epub 2023 May 16 [PubMed PMID: 37191887]
Level 1 (high-level) evidenceGlickel SZ, Catalano LW, Raia FJ, Barron OA, Grabow R, Chia B. Long-term outcomes of closed reduction and percutaneous pinning for the treatment of distal radius fractures. The Journal of hand surgery. 2008 Dec:33(10):1700-5. doi: 10.1016/j.jhsa.2008.08.002. Epub [PubMed PMID: 19084166]
Level 2 (mid-level) evidenceBindra RR. Biomechanics and biology of external fixation of distal radius fractures. Hand clinics. 2005 Aug:21(3):363-73 [PubMed PMID: 16039448]
Slutsky DJ. External fixation of distal radius fractures. The Journal of hand surgery. 2007 Dec:32(10):1624-37 [PubMed PMID: 18070654]
Tang JB. Distal radius fracture: diagnosis, treatment, and controversies. Clinics in plastic surgery. 2014 Jul:41(3):481-99. doi: 10.1016/j.cps.2014.04.001. Epub [PubMed PMID: 24996466]
Orbay JL, Touhami A. Current concepts in volar fixed-angle fixation of unstable distal radius fractures. Clinical orthopaedics and related research. 2006 Apr:445():58-67 [PubMed PMID: 16505728]
Downing ND, Karantana A. A revolution in the management of fractures of the distal radius? The Journal of bone and joint surgery. British volume. 2008 Oct:90(10):1271-5. doi: 10.1302/0301-620X.90B10.21293. Epub [PubMed PMID: 18827233]
Ring D, Jupiter JB, Brennwald J, Büchler U, Hastings H 2nd. Prospective multicenter trial of a plate for dorsal fixation of distal radius fractures. The Journal of hand surgery. 1997 Sep:22(5):777-84 [PubMed PMID: 9330133]
Level 1 (high-level) evidenceRothman A, Samineni AV, Sing DC, Zhang JY, Stein AB. Carpal Tunnel Release Performed during Distal Radius Fracture Surgery. Journal of wrist surgery. 2023 Jun:12(3):211-217. doi: 10.1055/s-0042-1756501. Epub 2022 Nov 9 [PubMed PMID: 37223388]
Velmurugesan PS, Nagashree V, Devendra A, Dheenadhayalan J, Rajasekaran S. Should ulnar styloid be fixed following fixation of a distal radius fracture?(). Injury. 2023 Jul:54(7):110768. doi: 10.1016/j.injury.2023.04.055. Epub 2023 May 2 [PubMed PMID: 37210301]
Szymanski JA, Reeves RA, Taqi M, Carter KR. Barton Fracture. StatPearls. 2023 Jan:(): [PubMed PMID: 29763081]
Level 2 (mid-level) evidenceLozano-Calderón SA, Souer S, Mudgal C, Jupiter JB, Ring D. Wrist mobilization following volar plate fixation of fractures of the distal part of the radius. The Journal of bone and joint surgery. American volume. 2008 Jun:90(6):1297-304. doi: 10.2106/JBJS.G.01368. Epub [PubMed PMID: 18519324]
Level 1 (high-level) evidenceNesbitt KS, Failla JM, Les C. Assessment of instability factors in adult distal radius fractures. The Journal of hand surgery. 2004 Nov:29(6):1128-38 [PubMed PMID: 15576227]
Mackenney PJ, McQueen MM, Elton R. Prediction of instability in distal radial fractures. The Journal of bone and joint surgery. American volume. 2006 Sep:88(9):1944-51 [PubMed PMID: 16951109]
Evans BT, Jupiter JB. Best Approaches in Distal Radius Fracture Malunions. Current reviews in musculoskeletal medicine. 2019 Jun:12(2):198-203. doi: 10.1007/s12178-019-09540-y. Epub [PubMed PMID: 30847731]
Mackinnon SE. Pathophysiology of nerve compression. Hand clinics. 2002 May:18(2):231-41 [PubMed PMID: 12371026]
Franz T. Entrapment of Extensor Pollicis Longus Tendon after Volar Plating of a Smith Type Pediatric Distal Forearm Fracture. The journal of hand surgery Asian-Pacific volume. 2016 Jun:21(2):253-6. doi: 10.1142/S2424835516720085. Epub [PubMed PMID: 27454642]
Mansour AA 3rd, Watson JT, Martus JE. Displaced dorsal metaphyseal cortex associated with delayed extensor pollicis longus tendon entrapment in a pediatric Smith's fracture. Journal of surgical orthopaedic advances. 2013 Summer:22(2):173-5 [PubMed PMID: 23628574]
Level 3 (low-level) evidenceMurakami Y, Todani K. Traumatic entrapment of the extensor pollicis longus tendon in Smith's fracture of the radius-case report. The Journal of hand surgery. 1981 May:6(3):238-40 [PubMed PMID: 7240677]
Level 3 (low-level) evidenceBonatz E, Kramer TD, Masear VR. Rupture of the extensor pollicis longus tendon. American journal of orthopedics (Belle Mead, N.J.). 1996 Feb:25(2):118-22 [PubMed PMID: 8640381]
Level 2 (mid-level) evidenceRoth KM, Blazar PE, Earp BE, Han R, Leung A. Incidence of extensor pollicis longus tendon rupture after nondisplaced distal radius fractures. The Journal of hand surgery. 2012 May:37(5):942-7. doi: 10.1016/j.jhsa.2012.02.006. Epub 2012 Mar 29 [PubMed PMID: 22463927]
Carroll TJ, Caraet B, Madsen N, Wilbur D. Development of de Quervain Tenosynovitis After Distal Radius Fracture. Hand (New York, N.Y.). 2023 May 28:():15589447231174042. doi: 10.1177/15589447231174042. Epub 2023 May 28 [PubMed PMID: 37246426]
Li Z, Smith BP, Tuohy C, Smith TL, Andrew Koman L. Complex regional pain syndrome after hand surgery. Hand clinics. 2010 May:26(2):281-9. doi: 10.1016/j.hcl.2009.11.001. Epub [PubMed PMID: 20494753]
Lorente A, Mariscal G, Lorente R. Incidence and risk factors for complex regional pain syndrome in radius fractures: meta-analysis. Archives of orthopaedic and trauma surgery. 2023 Sep:143(9):5687-5699. doi: 10.1007/s00402-023-04909-8. Epub 2023 May 20 [PubMed PMID: 37209231]
Level 1 (high-level) evidenceChristensen OM, Christiansen TG, Krasheninnikoff M, Hansen FF. Length of immobilisation after fractures of the distal radius. International orthopaedics. 1995:19(1):26-9 [PubMed PMID: 7768655]
Level 1 (high-level) evidenceLuo P, Lou J, Yang S. Pain Management during Rehabilitation after Distal Radius Fracture Stabilized with Volar Locking Plate: A Prospective Cohort Study. BioMed research international. 2018:2018():5786089. doi: 10.1155/2018/5786089. Epub 2018 Nov 5 [PubMed PMID: 30519581]