Introduction
Staphylococcus aureus (S. aureus) is a pathogen that has been published in the literature since the 1800s. At that time, it was better recognized as a cause of sepsis and abscess formation. More than a century after the first descriptions of Staphylococcus were written, we now understand it to be at the forefront of many disease processes, one of which is staphylococcal pneumonia. Staphylococcus remains at the forefront of infectious disease due to its enzyme production of protease, lipase, hyaluronidase, as well as its ability to make penicillin binding protein 2A (PBP-2A) through the mecA gene, leading to the staphylococcal strain known as methicillin-resistant Staphylococcus aureus (MRSA). This escalates its ability to become resistant to previous and current antibiotic therapies.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Community-acquired staphylococcal pneumonia is usually seen in patients that are recovering from influenza. The infection is seen in a bimodal distribution, with the younger and elderly populations being more at risk. It should be noted that Pneumococcus is still the leading cause of post-viral pneumonia in this population.[2] Individuals may also be colonized with S. aureus on the skin or in nares, and this can also lead to pulmonary infections and is seen in both the community and in the hospital setting. Another notable etiology of S. aureus pneumonia is seen in patients who abuse intravenous drugs. Due to contamination of the skin or equipment, IV drug abuse can lead to multiple systemic infections from S. aureus such as tricuspid valve endocarditis, bacteremia, and septic emboli to the lungs.[3]
Epidemiology
When describing S. aureus, it is crucial to delineate methicillin-resistant Staphylococcus aureus (MRSA) from methicillin-susceptible Staphylococcus aureus (MSSA) as this will determine the treatment strategies for these patients. A large, international multicenter study of hospitalized patients with community-acquired pneumonia (CAP) found that 3% of patients developed CAP secondary to MRSA. This had varying prevalence depending on the residency and location of the patient. Fifty-one percent of the S. aureus isolates were found to be secondary to MRSA, and 49% were secondary to MSSA.[4] Another study of inpatients who were hospitalized for CAP in the United States showed that 1.7% were secondary to S. aureus, and of these, 0.7% were secondary to MRSA, and 1% were secondary to MSSA.[5]
Pathophysiology
Bacteria and viruses are part of the healthy microbiome of the lower respiratory tract, and the majority of the microbiome of the alveoli are composed of anaerobic flora and microaerophilic streptococci. One mechanism of the development of pneumonia is the replication and multiplication of these organisms. Another mechanism is a breakdown of the host's innate immune system, which can lead to overwhelming multiplication of the normal healthy lower respiratory tract flora.[6] It is known that tobacco and alcohol use can alter the host defense and predispose to the development of pneumonia. More specific to staphylococcal pneumonia, microaspiration of staph species in the nares can lead to the development of staphylococcal pneumonia. Hematogenous spread from staphylococcal bacteremia can also develop into staphylococcal pneumonia, and this can be seen in staphylococcal endocarditis.
History and Physical
S. aureus infection can preclude patients to a wide range of infectious processes. Therefore, a thorough multisystem history and physical should be performed. When evaluating the need for hospitalization of the patient, care should be taken to assess the onset of symptoms, duration of symptoms, as well as associative symptoms of fever, chills, dyspnea, or productive cough. Eighty percent of patients with pneumonia can be febrile. However, this finding is less reliable in the elderly. Evaluation for sick contacts, recent travel, ongoing or recent infection with influenza can also help delineate those who may have a higher predisposition to developing S. aureus pneumonia. Employment status and recent hospitalizations can be ascertained to raise clinical suspicion for colonization with S. aureus, such as healthcare workers.
In the appropriate clinical scenario, evaluation for IV drug use should be ascertained as tricuspid valve endocarditis from IV drug use can lead to septic emboli to the lungs and cause S. aureus pneumonia. Physical exam should include a complete multisystem evaluation, but the focus should be given to the cardiopulmonary examination to assess for signs of valvular murmur, respiratory distress, tachypnea, or inspiratory crackles in a lobar pattern. Percussion and tactile fremitus can also be utilized if there is a concern for pleural effusion. Unfortunately, there is no specific constellation of history and physical exam findings that can effectively guarantee with certainty a diagnosis of pneumonia, but the above findings do further the clinical suspicion of this disease process.[7]
Evaluation
Initial evaluation for staphylococcal pneumonia starts with the same foundational workup for those suspected of having any etiology of CAP. A complete blood count (CBC) will likely show leukocytosis with a neutrophilic predominance. The gold standard for diagnosing pneumonia with the appropriate clinical suspicion is the presence of infiltrate on a chest radiograph.[8] The infiltrate on a chest radiograph can show lobar infiltrate or in severe patients can show cavitary lesions and empyema. If the clinical syndrome supports the diagnosis of pneumonia, but the chest radiograph does not reveal pathology, a computed tomography (CT) scan can be performed to further evaluate for pathology in the lungs.
Findings on CT scan may show a developing lobar infiltrate or cavitary lesion that chest radiograph may not reveal.[9] A sputum sample can be obtained, but a 2005 study noted that only 17% of the study population were able to produce an adequate sample. However, if the patient can produce an adequate sample, 82% were found to be diagnostic and could be used to guide antibiotic therapy.[10] An MRSA swab may also be utilized to assess the patient's colonization status for MRSA and, therefore, further the suspicion of this process. A procalcitonin level can also be drawn at the time of treatment in order to guide antibiotic efficacy and aid in antibiotic stewardship.[11]
Treatment / Management
Treatment for staphylococcal pneumonia depends on if this process is categorized into either MRSA or MSSA. If MRSA is suspected or confirmed, either vancomycin or linezolid should be initiated at the start of treatment and be promptly discontinued if MRSA is ruled out. Both vancomycin and linezolid have similar efficacy, and selection should be based on patient tolerance, antibiotic allergy profile, renal function, drug interaction, and intravenous access. As linezolid is systemically bioavailable in its oral form, this is preferred if there is an issue with intravenous access. Vancomycin is preferred if the patient is cytopenic or taking selective serotonin reuptake inhibitors (SSRIs).[12][13] Ceftaroline can be used if vancomycin or linezolid are contraindicated; however, it should be known that it is not FDA approved for hospital-acquired pneumonia or ventilator-associated pneumonia. Clindamycin is also an alternative, but it is also less efficacious in hospital-acquired and ventilator-associated pneumonia.[14] (A1)
If culture results grow MSSA and rule out other causes of pneumonia, then therapy can be de-escalated to nafcillin, oxacillin, or cefazolin.[15] Supportive measures for staphylococcal pneumonia include bronchodilation to help those with underlying lung diseases such as asthma or chronic obstructive pulmonary disease (COPD). Supplemental oxygenation may also be needed due to the restrictive lung disease caused by the pneumonia disease process. This can begin with a nasal cannula. However, if the disease process is severe enough, then mechanical ventilation may be necessary.(A1)
Differential Diagnosis
As the clinical presentation for pneumonia and, therefore, staphylococcal pneumonia is broad and nonspecific, so is the differential for this process. Differential diagnosis may include:
- Pneumonia secondary to:
- Streptococcal pneumonia
- Nontypeable Haemophilus influenza
- Mycoplasma pneumonia
- Chlamydia pneumonia
- Legionella
- Gram-negative bacilli
- Group A Streptococcus
- Anaerobic infection
- Mycoplasma tuberculosis
- Viral infection
- Pulmonary edema secondary to congestive heart failure
- Pulmonary hemorrhage
- Atelectasis
- Pneumonitis from aspiration or chemical exposure
- Interstitial lung disease
- Drug reaction
- Pulmonary embolism
Prognosis
Prognosis of staphylococcal pneumonia is very much dependent on the patient's comorbid conditions, underlying lung disease, and sequelae of this disease process. Prognosis is more guarded if the patient becomes bacteremic, and this further alludes to the importance of astute clinical suspicion and appropriate antibiotic intervention.
Complications
A significant complication of staphylococcal pneumonia is the development of severe necrotizing pneumonia. This can be seen in community associated-MRSA (CA-MRSA).[16] If this is of clinical concern, then a chest CT may be warranted to help further assess for this pathology. It should be noted that a chest CT should not be used in the initial diagnosis of pneumonia, and that chest x-ray should be ordered first as a foundational approach to the initial evaluation of pneumonia. Staphylococcal pneumonia may also lead to complications such as sepsis, septic shock, bacteremia, and respiratory failure leading to invasive mechanical ventilation.
Deterrence and Patient Education
Patients should be educated on the presentation of CAP in the outpatient setting, as this could lead to a faster diagnosis of CAP and possibly staphylococcal pneumonia in the appropriate clinical scenario. This is important for patients to be educated on, as prompt antibiotic therapy can help resolve this infectious process before sequelae such as sepsis, bacteremia, or respiratory failure occur.
Enhancing Healthcare Team Outcomes
Clinicians need to have an interprofessional team approach to the diagnosis and treatment of these patients. There should be a broad clinical suspicion with this and any presentation of patients with pneumonia. Nursing staff should also have a broad suspicion as they are foundational to patient care and help add information that the patient may not have alluded to during the initial encounter. Pharmacy staff should also be utilized to their fullest potential as antibiotic therapy and stewardship are essential to practice to help not only treat this disease process but also prevent antibiotic resistance in the future.
Media
(Click Image to Enlarge)
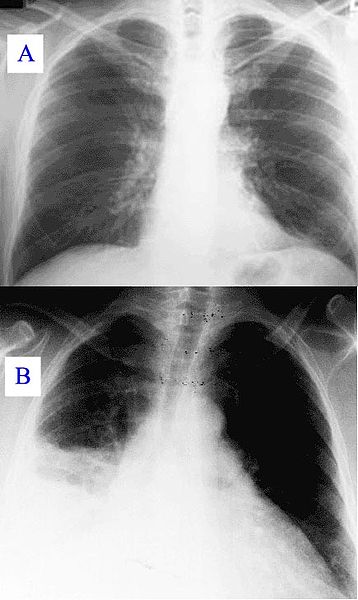
Healthy Lung and Q Fever Pneumatic Lung, Chest X-ray. X-ray A represents a normal healthy lung; X-ray B represents a lung with Q fever pneumonia.
Hehkuviini, Public Domain, via Wikimedia Commons.
{kind=link}
(Click Image to Enlarge)

Bilateral Pneumonia, Computed Tomography Scan. Bilateral pneumonia with abscesses, effusions, and cavers in an adult male.
Christaras A, Public Domain, via Wikimedia Commons (CC by 2.5).
References
Lowy FD. Staphylococcus aureus infections. The New England journal of medicine. 1998 Aug 20:339(8):520-32 [PubMed PMID: 9709046]
Francis JS, Doherty MC, Lopatin U, Johnston CP, Sinha G, Ross T, Cai M, Hansel NN, Perl T, Ticehurst JR, Carroll K, Thomas DL, Nuermberger E, Bartlett JG. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2005 Jan 1:40(1):100-7 [PubMed PMID: 15614698]
Level 3 (low-level) evidenceHind CR. Pulmonary complications of intravenous drug misuse. 1. Epidemiology and non-infective complications. Thorax. 1990 Nov:45(11):891-8 [PubMed PMID: 2256022]
Aliberti S, Reyes LF, Faverio P, Sotgiu G, Dore S, Rodriguez AH, Soni NJ, Restrepo MI, GLIMP investigators. Global initiative for meticillin-resistant Staphylococcus aureus pneumonia (GLIMP): an international, observational cohort study. The Lancet. Infectious diseases. 2016 Dec:16(12):1364-1376. doi: 10.1016/S1473-3099(16)30267-5. Epub 2016 Sep 1 [PubMed PMID: 27593581]
Self WH, Wunderink RG, Williams DJ, Zhu Y, Anderson EJ, Balk RA, Fakhran SS, Chappell JD, Casimir G, Courtney DM, Trabue C, Waterer GW, Bramley A, Magill S, Jain S, Edwards KM, Grijalva CG. Staphylococcus aureus Community-acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Aug 1:63(3):300-9. doi: 10.1093/cid/ciw300. Epub 2016 May 8 [PubMed PMID: 27161775]
Strieter RM, Belperio JA, Keane MP. Host innate defenses in the lung: the role of cytokines. Current opinion in infectious diseases. 2003 Jun:16(3):193-8 [PubMed PMID: 12821807]
Level 3 (low-level) evidenceMetlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997 Nov 5:278(17):1440-5 [PubMed PMID: 9356004]
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG, Infectious Diseases Society of America, American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2007 Mar 1:44 Suppl 2(Suppl 2):S27-72 [PubMed PMID: 17278083]
Level 3 (low-level) evidenceSyrjälä H, Broas M, Suramo I, Ojala A, Lähde S. High-resolution computed tomography for the diagnosis of community-acquired pneumonia. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1998 Aug:27(2):358-63 [PubMed PMID: 9709887]
van der Eerden MM, Vlaspolder F, de Graaff CS, Groot T, Jansen HM, Boersma WG. Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2005 Apr:24(4):241-9 [PubMed PMID: 15902529]
Christ-Crain M, Jaccard-Stolz D, Bingisser R, Gencay MM, Huber PR, Tamm M, Müller B. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet (London, England). 2004 Feb 21:363(9409):600-7 [PubMed PMID: 14987884]
Level 1 (high-level) evidenceJiang H, Tang RN, Wang J. Linezolid versus vancomycin or teicoplanin for nosocomial pneumonia: meta-analysis of randomised controlled trials. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2013 Sep:32(9):1121-8. doi: 10.1007/s10096-013-1867-z. Epub 2013 Apr 10 [PubMed PMID: 23568605]
Level 1 (high-level) evidenceWang Y, Zou Y, Xie J, Wang T, Zheng X, He H, Dong W, Xing J, Dong Y. Linezolid versus vancomycin for the treatment of suspected methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a systematic review employing meta-analysis. European journal of clinical pharmacology. 2015 Jan:71(1):107-15. doi: 10.1007/s00228-014-1775-x. Epub 2014 Oct 30 [PubMed PMID: 25355172]
Level 1 (high-level) evidenceLiu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, J Rybak M, Talan DA, Chambers HF, Infectious Diseases Society of America. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2011 Feb 1:52(3):e18-55. doi: 10.1093/cid/ciq146. Epub 2011 Jan 4 [PubMed PMID: 21208910]
Level 1 (high-level) evidenceKalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O'Grady NP, Bartlett JG, Carratalà J, El Solh AA, Ewig S, Fey PD, File TM Jr, Restrepo MI, Roberts JA, Waterer GW, Cruse P, Knight SL, Brozek JL. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Sep 1:63(5):e61-e111. doi: 10.1093/cid/ciw353. Epub 2016 Jul 14 [PubMed PMID: 27418577]
Level 1 (high-level) evidenceGillet Y, Issartel B, Vanhems P, Fournet JC, Lina G, Bes M, Vandenesch F, Piémont Y, Brousse N, Floret D, Etienne J. Association between Staphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia in young immunocompetent patients. Lancet (London, England). 2002 Mar 2:359(9308):753-9 [PubMed PMID: 11888586]