Introduction
Stent thrombosis is defined as a thrombotic occlusion of a coronary stent. Stent thrombosis is a major complication associated with stent placement in percutaneous coronary intervention (PCI). Stent thrombosis has been associated with high rates of morbidity and mortality, often leading to events of cardiac death or nonfatal myocardial infarction (MI).[1][2][3] Often compared to in-stent restenosis, which leads to anginal type symptoms, stent thrombosis is typically an acute process resulting in acute coronary syndrome (ACS). Various risk factors have been associated with stent thrombosis, including a history of diabetes mellitus (DM), ACS, and reduced left ventricular ejection fraction (LVEF). In 2008, the Academic Research Consortium (ARC) guidelines were published regarding the classifications of stent thrombosis.[4] Classifications were divided based on the type of underlying stent, clinical scenario, and timing after initial stent placement.
- Based on the underlying stent, stent thrombosis should be divided into categories of a bare-metal stent (BMS), a first-generation drug-eluting stent (DES), and second-generation DES.
In terms of timing, there are a variety of categories for stent thrombosis. Timing may be divided between acute, subacute, early, late, and very late. Early stent thrombosis is divided between acute or subacute:
- Acute thrombosis occurs within 24 hours of initial placement.
- Subacute thrombosis occurs between 24 hours to one month of initial placement.
When classified as early, late, or very late:
- Early stent thrombosis occurs within one month of initial placement.
- Late stent thrombosis occurs between 1 and 12 months of initial placement.
- Very late stent thrombosis occurs after 12 months of initial placement.[5]
Based on the clinical scenario, stent thrombosis may be symptomatic or clinically silent. As noted above, due to the nature of acute thrombotic occlusion stent thrombosis typically results in ACS. Stent thrombus should be classified based on how the diagnosis is confirmed. These classifications include definite, probable, and possible stent thrombosis.
- Silent occlusion- Incidental stent occlusion on angiography in the absence of clinical signs or symptoms is not considered stent thrombosis.
- Possible stent thrombosis
- Consider with unexplained death 30 days or later after stent placement.
- Probable stent thrombosis
- Any unexplained death within 30 days of stent placement.
- Consider if there is active ischemia on electrocardiogram (EKG) or stress in the distribution of prior stent and absence of significant coronary lesion on angiography.
- Definite stent thrombosis
- Requires confirmation of stent thrombosis on angiography
- Within the existing stent
- Within 5 mm proximal or distal to the stent
- Requires confirmation of stent thrombosis on angiography
-
- Plus one of the following within 48 hours
- Acute onset of ischemic symptoms at rest
- New ischemic changes on ECG
- A typical rise in cardiac biomarkers
- Thrombus on autopsy or retrieved with thrombectomy
- Plus one of the following within 48 hours
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Large randomized trials and registry have identified patient/lesion, procedural, or stent factors related to stent thrombosis.[6][7] Champion-phoenix trial identified Non-ST-elevation myocardial infarction (NSTEMI) and ST-elevation myocardial infarction (STEMI) at presentation, angiographic thrombus burden, and total stent length as independent predictors of acute stent thrombosis.[8] An acuity trial revealed diabetes mellitus, renal insufficiency, Duke jeopardy score, final stent minimal luminal diameter, preprocedural thienopyridine administration, baseline hemoglobin, and extent of coronary artery disease as independent factors associated with early stent thrombosis. In an intravascular ultrasound (IVUS) substudy of the Horizon AMI (acute myocardial infarction) trial, the small cross-sectional area of less than 5 mm, malposition of stent struts, plaque prolapse or protrusion, edge dissection, and residual stenosis played significant roles in predicting early stent thrombosis.[9] Also, bifurcation stenting contributed to stent thrombosis. The Triton TIMI 38 trial showed that patients with STEMI are at higher risk of stent thrombosis regardless of stent type and that more potent antiplatelet therapy such as prasugrel reduced that risk by 50%.[10]
Epidemiology
Stent thrombosis has been recognized from the early era of stent deployment, with an incidence as high as 16% in earlier studies. Fifteen to 30% of the patients with stent thrombosis die within 30 days of the event.[11] Acetylsalicylic acid (ASA), dipyridamole, coumadin, and dextran were tried in the early stenting era to prevent the event. With the current practice of dual antiplatelet therapy and high-pressure inflation has significantly decreased incidence to 0.7% in one year and about 0.2% to 0.6% the year after that. The rate is lower for elective percutaneous intervention (PCI) (0.3% to 0.5%) but as high as 3.4% for acute coronary syndrome. There has been overall no significant difference between the rate of stent thrombosis between bare-metal stents and eluting drug stents. Only the timing of the event varies. The bare-metal stent tends to have an early event with a peak of around 30 days compared to drug-eluting stents around three months to even later depending on the drug-coated.[12][13]
Pathophysiology
Virchow’s triad explains the major factors that lead to stent thrombosis.[14] First, stasis and turbulence caused by an under-expanded stent, a stent in a small vessel, or a long lesion. Second, injury or endothelial disruption caused by edge dissection or delayed healing with eluting drug stents. Finally, hypercoagulability caused by congenital or acquired or nonresponder.[15]
History and Physical
A thorough history, medication compliance review, laboratory testing for P2Y12 resistance, a 12 lead EKG, echocardiogram looking for a new wall motion abnormality, and laboratory testing of cardiac enzymes is recommended for initial evaluation of a patient with recent percutaneous coronary intervention presenting with angina.[16] Universally, 60% of the patients with stent thrombosis present with STEMI and 40% with NSTEMI or unstable angina. Patients with STEMI, in the context of stent thrombosis, have greater rates of in-hospital mortality (17.4%). Patients with early stent thrombosis are more likely to develop cardiogenic shock than to develop late or very late stent thrombosis. It is very unlikely that a patient with nonacute coronary syndrome presentation would have evidence of stent thrombosis on subsequent coronary angiograms performed.
Evaluation
High clinical suspicion is the most important evaluation for a patient presenting with angina and a recent history of coronary stenting. The patient is usually evaluated with history, physical examination, EKG, echocardiogram, and cardiac enzymes. Almost all patients with STEMI undergo urgent coronary angiography.[11]
Treatment / Management
During angiography, a prompt aspiration thrombectomy or angioplasty should be performed to restore the patency of the thrombosed vessel. Compliance and drug resistance should be evaluated. More potent antiplatelet therapy should be considered, for example, prasugrel or ticagrelor.[17][18][19] The current recommendation is to continue the dual antiplatelet drug therapy for one year after drug-eluting stent placement and at least one month following bare-metal stent. The stent should be assessed with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT) to determine stent apposition, expansion, and the presence of edge dissections. Optimization of stent deployment with appropriate postulation and treatment of edge dissections with additional stents are imperative to prevent repeat stent thrombosis. Additional stent implantation should be avoided if possible because each millimeter of the stent increases the probability of stent thrombosis.
Differential Diagnosis
One differential diagnosis includes:
- in-stent restenosis, which leads to anginal type symptoms.
Stent thrombosis is typically a more acute process resulting in acute coronary syndrome (ACS). Additionally, episodes of ACS within native vessels should be excluded.
Prognosis
Stent thrombosis has been associated with high rates of morbidity and mortality, often leading to events of cardiac death or nonfatal myocardial infarction (MI). When compared to in-stent restenosis, which leads to anginal type symptoms, stent thrombosis is typically an acute process resulting in acute coronary syndrome (ACS). Prognosis improves greatly with early identification and intervention. High clinical suspicion and detailed history taking are crucial for an accurate diagnosis.[15]
Complications
Stent thrombosis is a major complication associated with stent placement in PCI. Complications associated with untreated stent thrombosis include death, myocardial infarction, and cardiogenic shock. Complications related to the treatment of stent thrombosis are similar to that of PCI. These include but are not limited to bruising, hematoma, pseudoaneurysm, retroperitoneal hemorrhage, arrhythmia, contrast-induced nephropathy, thrombus formation, infection, ischemic stroke, and myocardial infarction.[20]
Deterrence and Patient Education
Patients should be educated following PCI with DES placement of the risks associated with stent thrombosis in the postoperative period.[21] Additionally, patients should be instructed to present to the emergency department for further evaluation if typical anginal or acute coronary syndrome symptoms should develop.
Enhancing Healthcare Team Outcomes
When patients with stents present with chest pain to the primary care provider, internist, and nurse practitioner, one should always consider stent thrombosis. These patients should be immediately referred to the cardiologist for further investigation and treatment. Stent thrombosis, when it occurs acutely, can be fatal if not treated right away. The triage nurse should be aware of this condition and immediately admit the patient and consult with the emergency department provider. Careful monitoring by the nursing staff is required with frequent reports to the providers. Due to the complexity of treatment, a specially trained cardiac pharmacist should assist with medication selection, dosing, and monitoring working with the clinical team. The prognosis depends on many factors, including patient age, duration of thrombosis, number of stents involved, and response to medical treatment. In some cases, an urgent coronary bypass is required.[22][23][24] (Level 2)
Media
(Click Image to Enlarge)
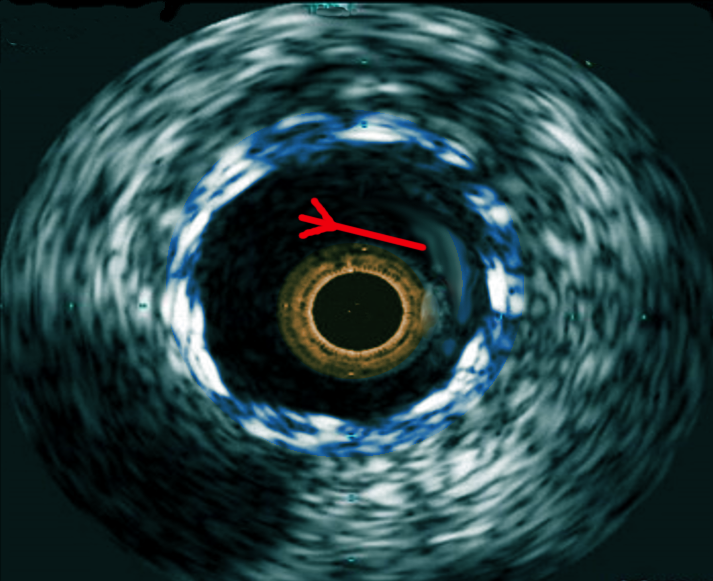
IVUS-in stent thrombosis Image courtesy S Bhimji MD
References
Longobardo L, Mattesini A, Valente S, Di Mario C. OCT-guided Percutaneous Coronary Intervention in Bifurcation Lesions. Interventional cardiology (London, England). 2019 Feb:14(1):5-9. doi: 10.15420/icr.2018.17.2. Epub [PubMed PMID: 30858885]
Piranavan P, Kaur NJ, Marmoush F, Burton A, Hannan J. Ticagrelor-induced Angioedema After Percutaneous Coronary Intervention in a Patient with a History of Ischemic Stroke and Low Response to Clopidogrel: A Rare Dilemma. Cureus. 2018 Dec 11:10(12):e3720. doi: 10.7759/cureus.3720. Epub 2018 Dec 11 [PubMed PMID: 30891370]
Lee SN, Moon D, Moon KW, Yoo KD. The Glasgow prognostic score as a significant predictor of clinical outcomes in patients with acute coronary syndrome. Journal of cardiology. 2019 Aug:74(2):130-135. doi: 10.1016/j.jjcc.2019.02.007. Epub 2019 Mar 13 [PubMed PMID: 30878352]
Level 2 (mid-level) evidenceCutlip DE, Nakazawa G, Krucoff MW, Vorpahl M, Mehran R, Finn AV, Vranckx P, Kimmelstiel C, Berger C, Petersen JL, Palabrica T, Virmani R. Autopsy validation study of the academic research consortium stent thrombosis definition. JACC. Cardiovascular interventions. 2011 May:4(5):554-9. doi: 10.1016/j.jcin.2011.01.011. Epub [PubMed PMID: 21596329]
Level 1 (high-level) evidenceChe QQ, Wu Q, Liang YB, Sun RM, Lyu QW, Ma JL, Hu H, Lin X, Xu GL, Sun SG, Zhang C, Wang QY, Yu J, Bai F. [Meta-analysis on safety and efficacy of dual antiplatelet therapy combining with proton pump inhibitors for patients after percutaneous coronary intervention]. Zhonghua xin xue guan bing za zhi. 2019 Feb 24:47(2):129-140. doi: 10.3760/cma.j.issn.0253-3758.2019.02.010. Epub [PubMed PMID: 30818941]
Level 1 (high-level) evidenceGuo C, Li M, Lv YH, Zhang MB, Wang ZL. De-escalation versus standard dual antiplatelet therapy in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. Platelets. 2020:31(1):15-25. doi: 10.1080/09537104.2019.1574969. Epub 2019 Feb 13 [PubMed PMID: 30759033]
Level 1 (high-level) evidenceWang Z, Xie Q, Xiang Q, Gong Y, Jiang J, Cui Y. Predictive Value of Methods Measuring Platelet Activation for Ischemic Events in Patients Receiving Clopidogrel: A Systematic Review and Meta-analysis. Current pharmaceutical design. 2018:24(44):5313-5333. doi: 10.2174/1381612825666190206114724. Epub [PubMed PMID: 30727868]
Level 1 (high-level) evidenceGénéreux P, Stone GW, Harrington RA, Gibson CM, Steg PG, Brener SJ, Angiolillo DJ, Price MJ, Prats J, LaSalle L, Liu T, Todd M, Skerjanec S, Hamm CW, Mahaffey KW, White HD, Bhatt DL, CHAMPION PHOENIX Investigators. Impact of intraprocedural stent thrombosis during percutaneous coronary intervention: insights from the CHAMPION PHOENIX Trial (Clinical Trial Comparing Cangrelor to Clopidogrel Standard of Care Therapy in Subjects Who Require Percutaneous Coronary Intervention). Journal of the American College of Cardiology. 2014 Feb 25:63(7):619-629. doi: 10.1016/j.jacc.2013.10.022. Epub 2013 Oct 30 [PubMed PMID: 24184169]
Level 1 (high-level) evidenceDangas GD, Claessen BE, Mehran R, Xu K, Stone GW. Stent thrombosis after primary angioplasty for STEMI in relation to non-adherence to dual antiplatelet therapy over time: results of the HORIZONS-AMI trial. EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2013 Jan 22:8(9):1033-9. doi: 10.4244/EIJV8I9A159. Epub [PubMed PMID: 23339809]
Level 1 (high-level) evidenceHusted S, Boersma E. Case Study: Ticagrelor in PLATO and Prasugrel in TRITON-TIMI 38 and TRILOGY-ACS Trials in Patients With Acute Coronary Syndromes. American journal of therapeutics. 2016 Nov/Dec:23(6):e1876-e1889 [PubMed PMID: 25830867]
Level 3 (low-level) evidenceNoaman S, O'Brien J, Andrianopoulos N, Brennan AL, Dinh D, Reid C, Sharma A, Chan W, Clark D, Stub D, Biswas S, Freeman M, Ajani A, Yip T, Duffy SJ, Oqueli E, Melbourne Interventional Group Investigators. Clinical outcomes following ST-elevation myocardial infarction secondary to stent thrombosis treated by percutaneous coronary intervention. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2020 Oct 1:96(4):E406-E415. doi: 10.1002/ccd.28802. Epub 2020 Feb 22 [PubMed PMID: 32087042]
Level 2 (mid-level) evidenceKim YH, Her AY, Jeong MH, Kim BK, Hong SJ, Ahn CM, Kim JS, Ko YG, Choi D, Hong MK, Jang Y. A comparison of the impact of current smoking on 2-year major clinical outcomes of first- and second-generation drug-eluting stents in acute myocardial infarction: Data from the Korea Acute Myocardial Infarction Registry. Medicine. 2019 Mar:98(10):e14797. doi: 10.1097/MD.0000000000014797. Epub [PubMed PMID: 30855497]
Level 2 (mid-level) evidenceZhao XY, Li JX, Tang XF, Xu JJ, Song Y, Jiang L, Chen J, Song L, Gao LJ, Gao Z, Qiao SB, Yang YJ, Gao RL, Xu B, Yuan JQ. Validation of Predictive Value of Patterns of Nonadherence to Antiplatelet Regimen in Stented Patients Thrombotic Risk Score in Chinese Population Undergoing Percutaneous Coronary Intervention: A Prospective Observational Study. Chinese medical journal. 2018 Nov 20:131(22):2699-2704. doi: 10.4103/0366-6999.245263. Epub [PubMed PMID: 30425196]
Level 2 (mid-level) evidenceYahagi K, Kolodgie FD, Otsuka F, Finn AV, Davis HR, Joner M, Virmani R. Pathophysiology of native coronary, vein graft, and in-stent atherosclerosis. Nature reviews. Cardiology. 2016 Feb:13(2):79-98. doi: 10.1038/nrcardio.2015.164. Epub 2015 Oct 27 [PubMed PMID: 26503410]
Ge J, Yu H, Li J. Acute Coronary Stent Thrombosis in Modern Era: Etiology, Treatment, and Prognosis. Cardiology. 2017:137(4):246-255. doi: 10.1159/000464404. Epub 2017 May 5 [PubMed PMID: 28472800]
Godschalk TC, Willemsen LM, Zwart B, Bergmeijer TO, Janssen PWA, Kelder JC, Hackeng CM, Ten Berg JM. Effect of Tailored Antiplatelet Therapy to Reduce Recurrent Stent Thrombosis and Cardiac Death After a First Episode of Stent Thrombosis. The American journal of cardiology. 2017 May 15:119(10):1500-1506. doi: 10.1016/j.amjcard.2017.02.033. Epub 2017 Feb 27 [PubMed PMID: 28318511]
Redfors B, Dworeck C, Haraldsson I, Angerås O, Odenstedt J, Ioanes D, Petursson P, Völz S, Albertsson P, Råmunddal T, Persson J, Koul S, Erlinge D, Omerovic E. Pretreatment with P2Y12 receptor antagonists in ST-elevation myocardial infarction: a report from the Swedish Coronary Angiography and Angioplasty Registry. European heart journal. 2019 Apr 14:40(15):1202-1210. doi: 10.1093/eurheartj/ehz069. Epub [PubMed PMID: 30851037]
Guy JM, Wilson M, Schnell F, Chevalier L, Verdier JC, Corone S, Doutreleau S, Kervio G, Carré F. Incidence of major adverse cardiac events in men wishing to continue competitive sport following percutaneous coronary intervention. Archives of cardiovascular diseases. 2019 Apr:112(4):226-233. doi: 10.1016/j.acvd.2018.11.008. Epub 2019 Jan 3 [PubMed PMID: 30612894]
Capodanno D, Alfonso F, Levine GN, Valgimigli M, Angiolillo DJ. ACC/AHA Versus ESC Guidelines on Dual Antiplatelet Therapy: JACC Guideline Comparison. Journal of the American College of Cardiology. 2018 Dec 11:72(23 Pt A):2915-2931. doi: 10.1016/j.jacc.2018.09.057. Epub [PubMed PMID: 30522654]
Torrado J, Buckley L, Durán A, Trujillo P, Toldo S, Valle Raleigh J, Abbate A, Biondi-Zoccai G, Guzmán LA. Restenosis, Stent Thrombosis, and Bleeding Complications: Navigating Between Scylla and Charybdis. Journal of the American College of Cardiology. 2018 Apr 17:71(15):1676-1695. doi: 10.1016/j.jacc.2018.02.023. Epub [PubMed PMID: 29650125]
Rokoszak V, Syed MH, Salata K, Greco E, de Mestral C, Hussain MA, Aljabri B, Verma S, Al-Omran M. A systematic review and meta-analysis of plain versus drug-eluting balloon angioplasty in the treatment of juxta-anastomotic hemodialysis arteriovenous fistula stenosis. Journal of vascular surgery. 2020 Mar:71(3):1046-1054.e1. doi: 10.1016/j.jvs.2019.07.075. Epub [PubMed PMID: 32089200]
Level 1 (high-level) evidenceAbdelaziz HK, Abuomara HZ, Ali MH, Eichhofer J, Patel B, Saad M. Routine use of optical coherence tomography in bioresorbable vascular scaffold implantation: insights on technique optimization and long-term outcomes. Coronary artery disease. 2019 Jun:30(4):263-269. doi: 10.1097/MCA.0000000000000736. Epub [PubMed PMID: 30883433]
Agarwal N, Mahmoud AN, Mojadidi MK, Golwala H, Elgendy IY. Dual versus triple antithrombotic therapy in patients undergoing percutaneous coronary intervention-meta-analysis and meta-regression. Cardiovascular revascularization medicine : including molecular interventions. 2019 Dec:20(12):1134-1139. doi: 10.1016/j.carrev.2019.02.022. Epub 2019 Mar 5 [PubMed PMID: 30862490]
Level 1 (high-level) evidenceHommels TM, Hermanides RS, Rasoul S, Berta B, IJsselmuiden AJJ, Jessurun GAJ, Benit E, Pereira B, De Luca G, Kedhi E. Everolimus-eluting bioresorbable scaffolds for treatment of coronary artery disease in patients with diabetes mellitus: the midterm follow-up of the prospective ABSORB DM Benelux study. Cardiovascular diabetology. 2019 Mar 9:18(1):25. doi: 10.1186/s12933-019-0827-z. Epub 2019 Mar 9 [PubMed PMID: 30851731]