Introduction
A subdural hematoma forms because of an accumulation of blood under the dura mater, one of the protective layers to the brain tissue under the calvarium. The understanding of subdural hematoma relies on the knowledge of neuroanatomical sheets covering the brain. The brain is the central repository of delicate neural tissue. This network of neurons and neuronal connective tissue is prone to injury without the protective layers, starting with the scalp and the bony structures of the skull. The brain finds its protection under the skull by the meninges that comprise three layers.
The inner surface of the skull toward the brain includes:
First, there is a leather-like structure called the dura mater, derived from the neural crest, adhering to the periosteum and facing the other meningeal structure, the arachnoid mater. The arachnoid mater lies under the dura mater (middle meningeal layer) forming many villi piercing through the dura with bridging veins acting as one-way valves to drain the neural tissue lying underneath the last meningeal layer called the pia mater. These so-called bridging veins may rupture when direct opposing forces rupture their thin walls, releasing blood under the dura mater forming a subdural hematoma.[1]
When there is a larger space between the dura mater and the brain, as seen in the young, growing brain or an aging brain (because of contraction), the cerebrospinal fluid (CSF) flows between bridging veins occupying a larger space. In this context, the structure stretches bridging veins and renders them prone to rupture. A small extravasation may resolve spontaneously. A larger bleed may augment the distance between the bridging veins and trigger an extensive amount of blood layering around the brain, slowly augmenting subdural space, decreasing the space of the brain leading to herniation of the cerebral structures.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
In the pediatric patient, trauma is the most common cause of subdural hematoma. Contributing factors include blunt and shearing injuries. Cranium extraction device use and traumatic birth delivery accounts for a majority of the SDH in the newborn period.[2] However, after the newborn period until age 2 years, the cause of SDH is predominantly due to accidental injury or intentional head injury. SDH due to intentional injury is frequently referred to as "shaken baby syndrome" The term correlates with the back-and-forth motion of the brain in the skull, held by the fragile bridging veins that rupture after violent, repeated movements against the inertia of the brain. Infants are prone to this as they do not have the muscular strength of the neck muscles to sustain the head during such an event. This also leads to retinal bleeding, a pathognomonic sign of shaken baby syndrome.[3]
Epidemiology
A subdural hematoma is one of the intracranial injuries associated with abusive head trauma (AHT). Other injuries discovered with AHT include epidural hematoma, diffuse axonal injury and parenchymal injury among others. The result of epidemiological studies report these injuries under a common heading for child abuse. The data for abusive head trauma is more robust in Europe and the United-States than in other geographic areas, with an incidence up to 17 per 100.000 child-years. However, the incidence of subdural hematoma occurring in children less than 2 years reaches close to 13 per 100,000 child-years. The risk of developing a subdural hematoma is higher below the age of one year (1:4761) according to a study in South Wales, England with an incidence reaching up to 21 per 100,000 child-years in this age group. Developing countries report similar rates; however, the data is very limited. There is no reported difference in gender for a subdural hematoma in the early stages; however, accidental subdural hematoma caused by trauma in the teenage years favors the male gender.
Pathophysiology
In shaken baby syndrome or battered infant syndrome,[4] the acceleration and decelerating forces of the brain during violent shaking of the head causes the brain to move in an opposite direction to the meninges causing the bridging veins to rupture and bleed in the subdural space. This potential space may accumulate a significant quantity of blood in various stages to exist in an acute or sub-acute form. Often, the bleeding is undetected initially, discovered as a chronic subdural hematoma. When there is a sufficient accumulation of blood to occupy a large intracranial space, the brain midline shifts toward the opposite side, encroaching on the brain structures against the inner surface of the calvarium after decreasing the volume of the lateral third and fourth ventricles. As the intracranial space becomes limited, the volumetric forces push the uncal portion of the temporal lobe toward the foramen magnum causing herniation of the brain.
Histopathology
The histopathological examination of the clot surrounding the dura gives insight into the post-traumatic interval (PTI).[5] The determination of this interval has relevant medico-legal implications. Where children are the subjects of abuse, the timing of the insult may help to identify a perpetrator. The examination focuses on the visualization of various cellular components of the dura and within the clot itself. Red blood cells, leukocytes, phagocytes, fibroblasts, hemosiderin containing cells, fibrin and proliferation of blood vessels. Clots that contain relatively intact blood cells without significant differentiation nor evidence of lysis are acute. Once the subdural clot organizes with fibrin, macrophages laden with hemosiderin and red blood cells and lysed red blood cells in the center, the clot is subacute. These findings are not absolute and are rarely definitive but reserved for the forensic postmortem examination.[6]
History and Physical
The history and physical examination in the infant and child may be problematic when it relates with abusive head trauma.[7] Often, the clinician faces an injury that contradicts the history given by the caretaker. In this context, any suspicion must trigger the proper clinical investigation and report to the authorities tasked for such an endeavor. The newborn who has experienced a traumatic birth often presents with a history of a difficult passage through the birth canal. The utilization of forceps or vacuum extraction devices that may occur during the extraction of the baby is of particular interest.[8] The caretaker often reports abnormal breathing patterns, apneic episodes associated with changes in the patient's behavior, vomiting, abnormal movements or seizures. Careful observation of the patient may reveal subtle or a more obvious alteration in the mental status presenting either as irritability or lethargy. When there is a clear history of trauma, external injury to the scalp where an underlying cephalohematoma is visible or palpated. In the infant having an open fontanel, the palpating of the latter may reveal to be tense, non-compliant or bulging. Often, other signs of abusive trauma are obvious on the skin in the form of bruising or limb deformities. Occasionally, no external visual injury is present on physical examination.
Evaluation
The management of the patient should include a complete blood count (CBC) with particular attention to the hemoglobin and hematocrit level. Patients may accumulate a significant amount of blood in the subdural space and display anemia due to blood loss before neurological signs. When there is longstanding accumulation as in chronic subdural hematoma, platelets decrease, signaling the beginning of consumptive coagulopathy. Prolonged prothrombin and activated prothrombin time, a decrease in fibrinogen, and elevation of fibrin degradation products may confirm this condition. A basic metabolic panel (BMP) is informative with particular attention to the serum potassium. Hyperkalemia heralds the breakdown of red blood cells that have extravasated into the subdural space. Stabilization of the patient to minimize the likelihood of secondary injury is of paramount importance. Following the initial stabilization, radiological investigation including a computerized tomography of the head is imperative. If time permits and the risks of sedation mitigated, a magnetic resonance imaging (MRI)[9] of the brain may reveal better imaging with subtle changes in the brain including the brain stem. The initial MRI of the brain can also help in aging of the subdural hematoma.[10]
Treatment / Management
The immediate treatment of a subdural hematoma initially includes management of the airway, breathing with stabilization of the circulation for the critical care professional. After stabilization and monitoring of the patient, a secondary plan of care should follow. The management must include the involvement of neurosurgery and neurological consultation with a consensus on the injury and a determination of the immediate and long-term consequences. Conservative non-surgical management for subacute and chronic subdural hematomas is appropriate if the accumulation has not extended further into the calvarium as to cause impingement on the brain or the brain stem. In contrast, a subdural hematoma that is quickly increasing or causing any signs of increased intracranial pressure, for example, hypertension, bradycardia with erratic respirations should prompt surgical evacuation and is paramount to preserve vital functions. In the interim, the clinician must begin immediate medical management. These measures include sedation, neuromuscular blockade when appropriate, moderate hyperventilation to a Pc02 (32 to 36), adequate oxygenation to maintain Sp02 greater than 95%, head elevation, and avoidance of hyperthermia.[11] The infusion of hypertonic saline or mannitol serves to decrease the intracranial pressure by promoting osmotic changes in the brain and transiently affecting the rheologic properties of the cerebral blood flow, respectively.[12][13](A1)
Differential Diagnosis
Other fluid substances may collections within the layers of the meninges to give the appearance of a subdural hematoma. A careful history and evaluation of radiological findings are necessary to rule out Purulent accumulation in the subdural abscess. In certain cases, the subarachnoid space occupied by the normally-occurring cerebrospinal fluid (CSF) with a natively decreased brain mass as in hydrocephalus ex vacuo may give the appearance of a subdural hematoma.
Prognosis
The prognosis of children affected by subdural hematoma is widely variable and depends on the extent of the intracranial injury. Many cases of subdural hematoma either traumatic or abusive remain undetected. However, many children live with severe neurological deficits including seizures, neurodevelopmental delay with static encephalopathy because of severe, devastating neurological injury.[14][9][15]
Consultations
The medical team should consider a neurosurgical consultation early into the management of a patient with a subdural hematoma. A pediatric neurologist is also an important addition to the consulting physicians. An ophthalmology consultation with complete the assessment of the retina is essential to determine abusive trauma in children.
Enhancing Healthcare Team Outcomes
In summary, a comprehensive management strategy focuses on maintaining the airway, supporting adequate oxygenation, maintaining adequate cerebral perfusion without further increasing the intracranial pressure and decreasing the cerebral metabolic rate are key for a positive outcome. This effort is best achieved with a coordinated collaboration among emergency department teams, radiology suites, neurology and neurosurgical teams, critical care teams including physicians, nurses and respiratory therapists. Social workers are helpful to navigate the complex social and legal aspects of abusive injury most times of subdural hematoma.[16][17] (Level V)
Outcomes
A subdural hematoma is not a benign disorder; mortality rates of 30% to 80% have been reported. Even those who survive may never fully regain functioning. Good outcomes are seen in less than one-third of patients. Younger patients tend to have better outcomes compared to older individuals. However, the ultimate prognosis depends on the cause and extent of brain injury. Those patients with minimal brain parenchymal injury have the best outcomes. [18][19] (Level V)
Media
(Click Image to Enlarge)
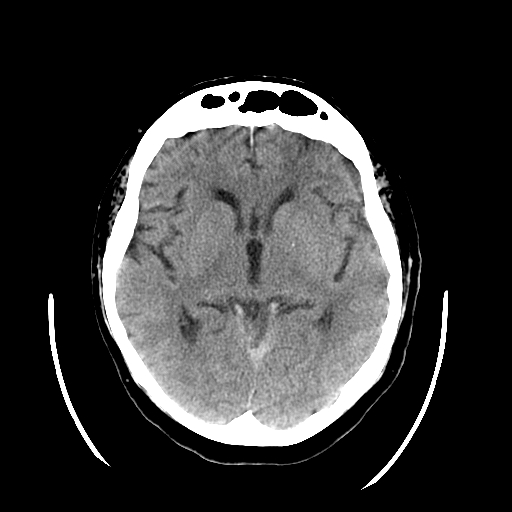
Head CT, Subdural Hematoma Tentorium
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)
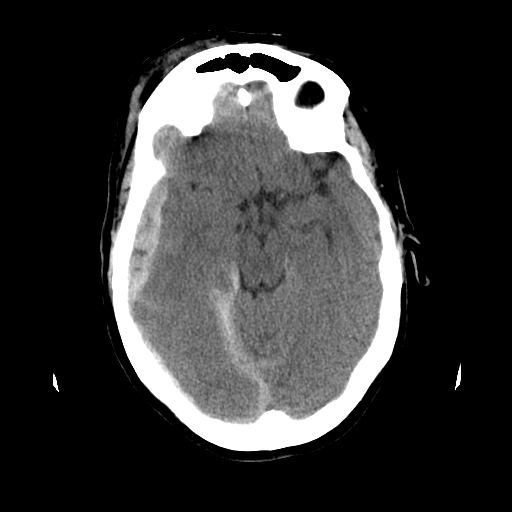
Head CT, Subdural Hematoma
Contributed by Scott Dulebohn, MD
(Click Image to Enlarge)
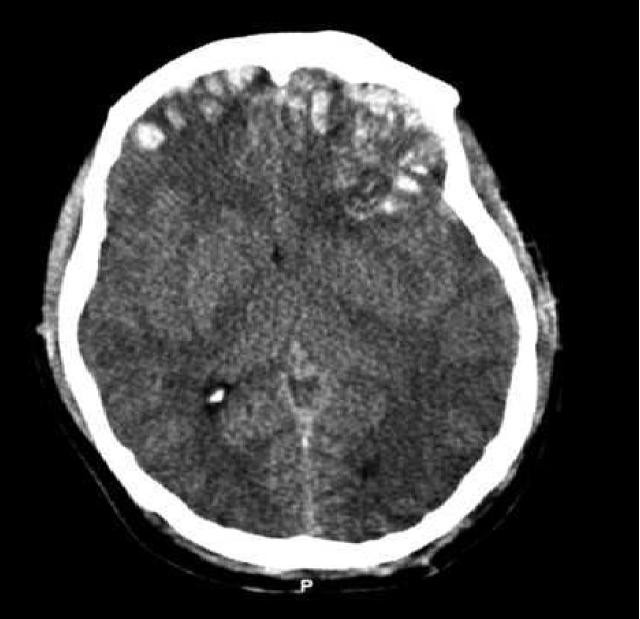
Brain Trauma Computed Tomography. This image shows a preoperative computed tomography (CT) scan of a patient with a Glasgow Coma Scale score of 14. The article reads, "Emergent CT imaging revealed a sagittally oriented skull fracture extending from the vertex to the foramen magnum as well as a transverse parietal and temporal bone fracture. Multiple frontal, parietal, and temporal lobe contusions with associated interhemispheric hemorrhage and a left-sided subdural hematoma measuring 1.7 mm in greatest depth were appreciated. Effacement of the basilar cisterns was noted without shift of midline structures."
Contributed by Wikimedia Commons, Rehman T, Ali R, Tawil I, Yonas H (CC by 2.0) https://creativecommons.org/licenses/by/2.0/deed.es
(Click Image to Enlarge)
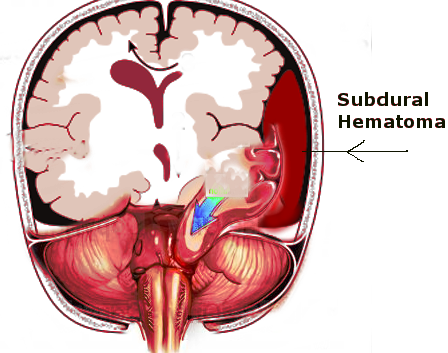
Subdural hematoma and uncal herniation Image courtesy S Bhimji MD
(Click Image to Enlarge)
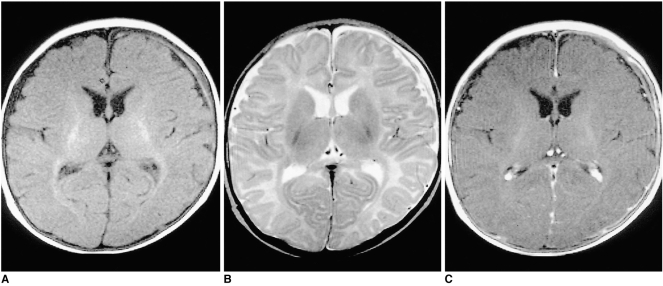
Shaken Baby Syndrome MRI Chronic subdural hematoma (SDH) in a three-month-old female patient A T1-weighted image shows mainly low-signal SDH, with a high signal focus in the left frontal area. B On a T2-weighted image the signal intensity of the chronic SDH is mainly high, with a focal area of low intensity. C Contrast-enhanced T1-weighted image shows overlying linear dural enhancement. Contributed by The National Center for Biotechnology Information (MRI by The Korean Radiological Society; http://creativecommons.org/licenses/by-nc/3.0)
References
Cheshire EC, Malcomson RDG, Sun P, Mirkes EM, Amoroso JM, Rutty GN. A systematic autopsy survey of human infant bridging veins. International journal of legal medicine. 2018 Mar:132(2):449-461. doi: 10.1007/s00414-017-1714-3. Epub 2017 Oct 26 [PubMed PMID: 29075919]
Level 3 (low-level) evidenceBode-Jänisch S,Bültmann E,Hartmann H,Schroeder G,Zajaczek JE,Debertin AS, Serious head injury in young children: birth trauma versus non-accidental head injury. Forensic science international. 2012 Jan 10 [PubMed PMID: 21868179]
Level 3 (low-level) evidenceChoudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, Moreno JA, Dias MS, Christian CW, Nelson MD Jr, Silvera VM, Palasis S, Raissaki M, Rossi A, Offiah AC. Consensus statement on abusive head trauma in infants and young children. Pediatric radiology. 2018 Aug:48(8):1048-1065. doi: 10.1007/s00247-018-4149-1. Epub 2018 May 23 [PubMed PMID: 29796797]
Level 3 (low-level) evidenceJoyce T, Gossman W, Huecker MR. Pediatric Abusive Head Trauma. StatPearls. 2023 Jan:(): [PubMed PMID: 29763011]
Rao MG,Singh D,Vashista RK,Sharma SK, Dating of Acute and Subacute Subdural Haemorrhage: A Histo-Pathological Study. Journal of clinical and diagnostic research : JCDR. 2016 Jul [PubMed PMID: 27630864]
Walter T, Meissner C, Oehmichen M. Pathomorphological staging of subdural hemorrhages: statistical analysis of posttraumatic histomorphological alterations. Legal medicine (Tokyo, Japan). 2009 Apr:11 Suppl 1():S56-62. doi: 10.1016/j.legalmed.2009.01.112. Epub 2009 Mar 18 [PubMed PMID: 19299189]
Amagasa S, Matsui H, Tsuji S, Moriya T, Kinoshita K. Accuracy of the history of injury obtained from the caregiver in infantile head trauma. The American journal of emergency medicine. 2016 Sep:34(9):1863-7. doi: 10.1016/j.ajem.2016.06.085. Epub 2016 Jun 29 [PubMed PMID: 27422215]
Doumouchtsis SK,Arulkumaran S, Head injuries after instrumental vaginal deliveries. Current opinion in obstetrics [PubMed PMID: 16601472]
Level 3 (low-level) evidenceGencturk M, Tore HG, Nascene DR, Zhang L, Koksel Y, McKinney AM. Various Cranial and Orbital Imaging Findings in Pediatric Abusive and Non-abusive Head trauma, and Relation to Outcomes. Clinical neuroradiology. 2019 Jun:29(2):253-261. doi: 10.1007/s00062-018-0663-7. Epub 2018 Jan 23 [PubMed PMID: 29362831]
Kralik SF,Yasrebi M,Supakul N,Lin C,Netter LG,Hicks RA,Hibbard RA,Ackerman LL,Harris ML,Ho CY, Diagnostic Performance of Ultrafast Brain MRI for Evaluation of Abusive Head Trauma. AJNR. American journal of neuroradiology. 2017 Apr [PubMed PMID: 28183837]
Czosnyka M, Pickard JD, Steiner LA. Principles of intracranial pressure monitoring and treatment. Handbook of clinical neurology. 2017:140():67-89. doi: 10.1016/B978-0-444-63600-3.00005-2. Epub [PubMed PMID: 28187815]
Wakai A, McCabe A, Roberts I, Schierhout G. Mannitol for acute traumatic brain injury. The Cochrane database of systematic reviews. 2013 Aug 5:2013(8):CD001049. doi: 10.1002/14651858.CD001049.pub5. Epub 2013 Aug 5 [PubMed PMID: 23918314]
Level 1 (high-level) evidenceMangat HS,Härtl R, Hypertonic saline for the management of raised intracranial pressure after severe traumatic brain injury. Annals of the New York Academy of Sciences. 2015 May [PubMed PMID: 25726965]
Level 3 (low-level) evidenceRumalla K,Letchuman V,Smith KA,Arnold PM, Hydrocephalus in Pediatric Traumatic Brain Injury: National Incidence, Risk Factors, and Outcomes in 124,444 Hospitalized Patients. Pediatric neurology. 2018 Mar [PubMed PMID: 29429778]
Castellani RJ, Mojica-Sanchez G, Schwartzbauer G, Hersh DS. Symptomatic Acute-on-Chronic Subdural Hematoma: A Clinicopathological Study. The American journal of forensic medicine and pathology. 2017 Jun:38(2):126-130. doi: 10.1097/PAF.0000000000000300. Epub [PubMed PMID: 28319470]
Zakaria Z, Kaliaperumal C, Crimmins D, Caird J. Neurosurgical management in children with bleeding diathesis: auditing neurological outcome. Journal of neurosurgery. Pediatrics. 2018 Jan:21(1):38-43. doi: 10.3171/2017.6.PEDS16574. Epub 2017 Nov 10 [PubMed PMID: 29125443]
Payne FL, Fernandez DN, Jenner L, Paul SP. Recognition and nursing management of abusive head trauma in children. British journal of nursing (Mark Allen Publishing). 2017 Sep 28:26(17):974-981. doi: 10.12968/bjon.2017.26.17.974. Epub [PubMed PMID: 28956988]
Rumalla K, Smith KA, Letchuman V, Gandham M, Kombathula R, Arnold PM. Nationwide incidence and risk factors for posttraumatic seizures in children with traumatic brain injury. Journal of neurosurgery. Pediatrics. 2018 Dec 1:22(6):684-693. doi: 10.3171/2018.6.PEDS1813. Epub [PubMed PMID: 30239282]
van Essen TA, Dijkman MD, Cnossen MC, Moudrous W, Ardon H, Schoonman GG, Steyerberg EW, Peul WC, Lingsma HF, de Ruiter GCW. Comparative Effectiveness of Surgery for Traumatic Acute Subdural Hematoma in an Aging Population. Journal of neurotrauma. 2019 Apr 1:36(7):1184-1191. doi: 10.1089/neu.2018.5869. Epub 2018 Oct 17 [PubMed PMID: 30234429]
Level 2 (mid-level) evidence