
Introduction
The subthalamic nucleus is located at the junction of the midbrain and diencephalon. It is a small lens-shaped structure that functionally participates with the basal ganglia (see Figure. Circuits of the Basal Ganglia). The subthalamic nucleus contains glutaminergic neurons with projections to the internal globus pallidus. The glutamatergic neurons increase the activity of the internal globus pallidus, which contains GABAergic neurons that, in turn, decrease the activity of the thalamus and inhibit movement. Lesions of the subthalamic nucleus can disrupt the inhibition of movement by the internal globus pallidus and result in hemiballismus (see Video. Hemiballism, Involuntary Movement, Cerebrovascular Accident, Stroke, Subthalamic Nucleus).
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The subthalamic nucleus is a small lens-shaped structure located within the diencephalon near the junction with the midbrain. The subthalamic nucleus composes the majority of the subthalamus along with the subthalamic fasciculus, ansa lenticularis, and several other smaller structures. The subthalamic nucleus is located medially to the internal capsule, dorsally to the substantia nigra, and ventrally to the thalamus. The primary function of the subthalamic nucleus is movement regulation along with the rest of the basal ganglia. Most neurons arising from the subthalamic nucleus are excitatory glutaminergic neurons and project to the internal globus pallidus. The internal globus pallidus primarily contains inhibitory GABAergic neurons that project to the thalamus. The thalamus then sends excitatory outputs to the cortex. The subthalamic nucleus receives input from the external globus pallidus, which contains mostly inhibitory GABAergic neurons. The subthalamic nucleus plays an essential role in the indirect pathway of the basal ganglia by preventing unwanted movements by increasing its glutaminergic output to the internal globus pallidus. Stimulating the GABAergic neurons of the internal globus pallidus results in decreased excitation of the thalamus and decreased movement. The medial portion of the subthalamic nucleus also contains limbic connections with the substantia nigra and ventral tegmental area. Chronic deep brain stimulation of the subthalamic nucleus in patients with Parkinson Disease can result in limbic system-related symptoms due to these connections.[1]
Embryology
The entirety of the central nervous system derives from the ectoderm. The mesodermally derived notochord induces the neural ectoderm formation. The notochord induces the formation of the neural groove. The neural groove develops into the neural fold on day 20, post-conception. The neural fold closes over itself both rostrally and caudally to form the neural tube. At 4 weeks gestation, the neural tube develops 3 outpouchings: the prosencephalon (forebrain), rhombencephalon (hindbrain), and mesencephalon (midbrain). At 6 weeks, the prosencephalon again divides into the telencephalon and diencephalon. The diencephalon forms the subthalamic nucleus and the thalamus, hypothalamus, retina, and third ventricle.[2]
Blood Supply and Lymphatics
Most subthalamic nuclei receive blood from the posteromedial branches of the posterior cerebral artery (P1 segment). The lateral portions of the subthalamic nucleus can receive vascular supply from the lenticulostriate arteries of the middle cerebral artery. The CNS lymphatic system is poorly understood but contains lymphatic drainage within the meninges.[3] The subthalamic nucleus does not contain any direct lymphatic drainage.
Nerves
The subthalamic nucleus plays a vital role in the modulation of movement. It helps to modulate movement through the indirect pathway of the basal ganglia with the other components of the basal ganglia. The indirect pathway of the basal ganglia consists of the glutaminergic excitatory neurons from the cortex and substantia nigra to the striatum. The striatum then projects inhibitory GABAergic neurons to the external globus pallidus, which projects inhibitory GABAergic neurons to the subthalamic nucleus. The subthalamic nucleus projects excitatory glutaminergic neurons to the internal globus pallidus and substantia nigra reticularis. These structures then project inhibitory GABAergic neurons to the thalamus. The thalamus then sends excitatory glutaminergic neurons to the cortex. Disruption of the neurons of the subthalamic nucleus results in the decreased firing of its glutaminergic neuronal outputs to the internal globus pallidus and substantia nigra reticularis. Decreased excitation of the GABAergic neurons of the globus pallidus internal results in reduced inhibition of the thalamic neurons. With no inhibition, the thalamic neurons fire excessively, resulting in hemiballismus.
Muscles
The subthalamic nucleus is composed entirely of neural tissue. It does not directly influence any muscles, but it plays a role in modulating movement with the other basal ganglia components. Damage to the subthalamic nucleus can result in a disorder of movement called hemiballismus.
Physiologic Variants
Dysfunction of the subthalamic nucleus results in phenotypically observable pathology. Its structure and function do not demonstrate common physiological variations.
Surgical Considerations
The first-line treatment for movement disorders involving the basal ganglia is medication.[4] However, deep brain stimulation or pallidotomy can be used in patients with severe cases unresponsive to medications. If deep brain stimulation is necessary, the patient is put under anesthesia and fitted with a stereotactic head frame. The patient is then imaged with a brain CT to determine the best path for electrode implantation. An incision is made in the scalp, and a burr hole is made into the skull for the electrode to pass into the brain. The patient is awake for the electrode placement so that the patient can provide immediate feedback about the electrode's effects. The patient is then placed back under anesthesia for tunneling of the leads behind the ear to the stimulator implanted in the chest. Absolute contraindications to deep brain stimulator implantation include uncorrectable coagulopathy, significant cognitive impairment, or severe psychopathology.
Clinical Significance
When the subthalamic nucleus or the tracts leading to or from the structure are damaged, hemiballismus can result. Hemiballismus characteristically causes ballistic flailing movements of an extremity that occurs contralaterally to the injured subthalamic nucleus. The most common etiology of hemiballismus is stroke. Hemiballismus is a relatively rare condition occurring as the sole manifestation of stroke in only roughly 0.4% to 0.54% of acute stroke.[5] MRI is the most sensitive imaging modality in cases where hemiballismus is present or suspected. Lesions resulting in hemiballismus may not appear on CT.[6] Lesions resulting in hemiballismus can be caused by an infarct, hemorrhage, trauma, infection, neurodegenerative disease, or neoplasm.[7] In some cases, lesions within the basal ganglia that do not involve the subthalamic nucleus can still produce hemiballismus.[8] First-line treatment for hemiballismus includes medications such as tetrabenazine, intrathecal baclofen, topiramate, or antidopaminergics such as haloperidol or chlorpromazine. In severe cases that are unresponsive to medication, surgery to implant electrodes for deep brain stimulation is a potential intervention. Surgical pallidotomy is another mechanism that has been used to treat intractable hemiballismus.[9] Subthalamic deep brain stimulation can also help patients with Parkinson disease with excessive movement-related symptoms and not responding to medications. Deep brain stimulation of the subthalamic nucleus has also been an option for treatment-resistant obsessive-compulsive disorder.[10]
Other Issues
Hemiballismus can also occur as a postoperative complication of neurological surgery if the subthalamic nucleus is damaged. Historically, surgical procedures have sought to avoid the subthalamic nucleus to avoid creating movement disorders. The effects of the subthalamic nucleus on the indirect pathway of the basal ganglia are critical for normal movement. When hemiballismus does occur, it can result in a high degree of morbidity for the patient.
Media
(Click Video to Play)
Hemiballism, Involuntary Movement, Cerebrovascular Accident, Stroke, Subthalamic Nucleus
Contributed by RS Menon, MD
(Click Image to Enlarge)
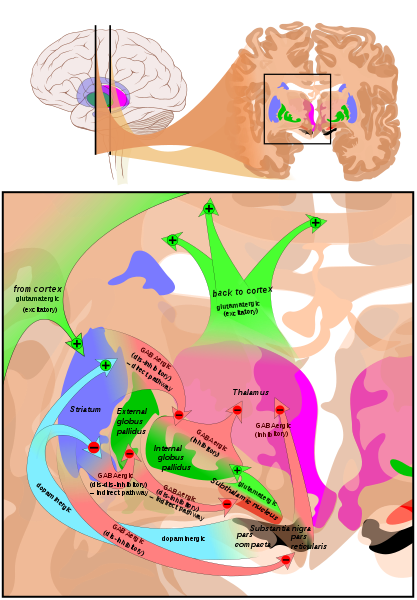
Circuits of the Basal Ganglia. The illustration depicts 2 coronal slices that have been superimposed to include the involved basal ganglia structures. + and - signs at the point of the arrows indicate, respectively, whether the pathway is excitatory or inhibitory in effect. Green arrows refer to excitatory glutamatergic pathways, red arrows refer to inhibitory GABAergic pathways, and turquoise arrows refer to dopaminergic pathways that are excitatory on the direct pathway and inhibitory on the indirect pathway. Note that dis-inhibitory pathways in effect are excitatory on the feedback to the cortex, while dis-dis-inhibitory pathways in effect are inhibitory.
Mikael Häggström, Public Domain, via Wikimedia Commons.
References
Mavridis I, Boviatsis E, Anagnostopoulou S. Anatomy of the human subthalamic nucleus: a combined morphometric study. Anatomy research international. 2013:2013():319710. doi: 10.1155/2013/319710. Epub 2013 Dec 15 [PubMed PMID: 24416591]
Martinez-Ferre A, Martinez S. Molecular regionalization of the diencephalon. Frontiers in neuroscience. 2012:6():73. doi: 10.3389/fnins.2012.00073. Epub 2012 May 25 [PubMed PMID: 22654731]
Dupont G, Schmidt C, Yilmaz E, Oskouian RJ, Macchi V, de Caro R, Tubbs RS. Our current understanding of the lymphatics of the brain and spinal cord. Clinical anatomy (New York, N.Y.). 2019 Jan:32(1):117-121. doi: 10.1002/ca.23308. Epub [PubMed PMID: 30362622]
Level 3 (low-level) evidenceShannon KM. Hemiballismus. Current treatment options in neurology. 2005 May:7(3):203-210 [PubMed PMID: 15814073]
Mahale RR, Mehta A, John AA, Buddaraju K, Shankar AK, Srinivasa R. Acute hemichorea-hemiballism as a sole manifestation of acute thalamic infarct: An unusual occurrence. Journal of neurosciences in rural practice. 2016 Jul-Sep:7(3):478-80. doi: 10.4103/0976-3147.181454. Epub [PubMed PMID: 27365980]
Katsumata T, Kitamura S, Inamura K, Terashi A. [Clinical and CT-findings in hemiballismus]. Nihon Ronen Igakkai zasshi. Japanese journal of geriatrics. 1992 Feb:29(2):123-8 [PubMed PMID: 1583799]
Level 3 (low-level) evidenceEtemadifar M, Abtahi SH, Abtahi SM, Mirdamadi M, Sajjadi S, Golabbakhsh A, Savoj MR, Fereidan-Esfahani M, Nasr Z, Tabrizi N. Hemiballismus, Hyperphagia, and Behavioral Changes following Subthalamic Infarct. Case reports in medicine. 2012:2012():768580. doi: 10.1155/2012/768580. Epub 2012 Oct 18 [PubMed PMID: 23125861]
Level 3 (low-level) evidenceLang AE. Persistent hemiballismus with lesions outside the subthalamic nucleus. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 1985 May:12(2):125-8 [PubMed PMID: 3926289]
Slavin KV, Baumann TK, Burchiel KJ. Treatment of hemiballismus with stereotactic pallidotomy. Case report and review of the literature. Neurosurgical focus. 2004 Jul 15:17(1):E7 [PubMed PMID: 15264776]
Level 3 (low-level) evidenceAlonso P, Cuadras D, Gabriëls L, Denys D, Goodman W, Greenberg BD, Jimenez-Ponce F, Kuhn J, Lenartz D, Mallet L, Nuttin B, Real E, Segalas C, Schuurman R, du Montcel ST, Menchon JM. Deep Brain Stimulation for Obsessive-Compulsive Disorder: A Meta-Analysis of Treatment Outcome and Predictors of Response. PloS one. 2015:10(7):e0133591. doi: 10.1371/journal.pone.0133591. Epub 2015 Jul 24 [PubMed PMID: 26208305]
Level 1 (high-level) evidence