Introduction
The superior cervical ganglia are involved in the autonomic nervous system. They are involved explicitly with sympathetic efferent innervation, particularly to the face and head. The superior cervical ganglion is the most superior ganglion of the sympathetic chain, bilaterally. It is the largest of the three ganglia of the cervical sympathetic trunk, the other two being the stellate and middle cervical ganglion.[1] The superior cervical ganglia are approximately at the levels of the second cervical vertebra (C2) and the third cervical vertebra (C3), bilaterally. They typically lie lateral to the longus colli muscles, bilaterally. The superior cervical ganglia usually lie anteromedial or medial to their respective internal carotid arteries.[1][2] They are considered a landmark for the sympathetic trunk and typically provide sympathetic innervation to the head and neck.[3][4]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The superior cervical ganglia are made up of the paravertebral ganglia of cervical vertebral levels one through four (C1-C4).[3][4] The superior cervical ganglia are oval shaped, cylinder-like, and elongated. They contain neurons.[1][5][6] They receive presynaptic signals from the sympathetic trunk. Postsynaptic signals then convey information from the superior cervical ganglia to targets in the head and neck.[2]
Embryology
The superior cervical ganglia derive from neural crest cells. Neural crest cells come from the ectoderm in embryological development. Many structures of the head, neck, face, and cardiovascular system also originate from the neural crest cells.[5][7]
Blood Supply and Lymphatics
Branches from the ascending pharyngeal artery, coming off of the external carotid artery, provide blood supply to the superior cervical ganglia. Venous drainage is through the internal jugular vein through direct posterior branches. There is a noted deficiency in gross blood supply at the junction of the upper one third and lower two-thirds of the neck; this is important for surgical considerations mentioned in the later part of this activity.[8]
The superior cervical ganglia are anterior to the retropharyngeal lymph nodes.[1][2]
Nerves
As previously described, the superior cervical ganglia are made up of the paravertebral ganglia of cervical vertebral levels one through four (C1-C4).[3][4] The superior cervical ganglia themselves contain neurons that supply sympathetic innervation to the head and neck.[5][6] The superior cervical ganglia provide postsynaptic fibers via the deep petrosal nerve to provide vasoconstriction to the lacrimal gland.[9] The superior cervical ganglia also supply gray rami communicantes to the ventral rami in the cervical plexus.[10] The superior cervical ganglia connect to the next closest ganglia, the middle cervical ganglia, inferiorly via the sympathetic trunk.[4]
Muscles
The superior cervical ganglia provide sympathetic innervation.[10] Their location is lateral to the longus colli muscles.[1][2]
Physiologic Variants
The superior cervical ganglia are typically present at cervical vertebral levels one and two (C1 and C2). However, they have been found between the cervical vertebral levels one through five. (C1-C5).[1] The ranges of the length of the superior cervical ganglia are from 10 to 30mm. The width of the superior cervical ganglia ranges from 5 to 8mm.[1]
Branches coming off of the superior cervical ganglia include the:
- Pharyngeal branch
- The communicating branch of the cervical nerve
- The internal carotid branch
- The communicating branch of the pharyngeal mucosa
- The communicating branch of the vagus nerve
- The communicating branch of the superior laryngeal nerve
- The laryngeal branch
- The communicating branch of the internal jugular vein
There are reports of up to seven different types of branch combinations coming off of the superior cervical ganglia.[2]
It is crucial to recognize that these are common variants of branches coming off of the superior cervical ganglia as damaging these may lead to consequences such as the development of Horner syndrome as described later in this activity.[1]
Surgical Considerations
It is important to avoid this the superior cervical ganglia during open anterior neck surgeries. When the superior cervical ganglia are damaged, Horner syndrome can develop. Horner syndrome comes from tension on the sympathetic trunk during anterior neck surgeries such as anterior cervical disc fusions. The tension causes damage to the fibers along the sympathetic trunk. More about Horner syndrome is described later in this activity.[1][4][11] Knowing the anatomy and landmarks regarding the neck helps to avoid damaging important neurovasculature in the area.[1]
Anterior surgical procedures to the neck area such as anterior cervical discectomies can cause a disruption of the blood supply to the superior cervical ganglia, causing ischemic damage to the ganglia. This ischemic damage can also cause symptoms similar to Horner syndrome.[7]
To prevent damage to the sympathetic ganglia during an anterior approach to the cervical spine, it is always advisable to create longus colli gutter and then place the retractors within the same, thereby minimizing the risk of inadvertent injury to the ganglia that lie lateral to the muscle.
Clinical Significance
The superior cervical ganglia can be a site for locally injected anesthetics such as opioids, which is useful for neuropathic pain management of the face.[1][2] The superior cervical ganglia are the main source of sympathetic innervation to the head and face. Buprenorphine has been specifically utilized in these ganglionic local opioid analgesia injections to provide pain relief to patients suffering from neuropathic facial pain stemming from atypical facial pain, postherpetic neuralgia, and trigeminal neuralgia.[12] Understanding the anatomic positioning of the superior cervical ganglia allows this injection to be performed safely by avoiding important structures such as the internal carotid arteries which lie close to the superior cervical ganglia.[1][2][12]. Ultrasound guidance can be utilized to visualize the superior cervical ganglia during this procedure properly.[12]
Damage to the superior cervical ganglia can cause a postganglionic pattern of Horner syndrome. The symptoms of Horner syndrome include miosis, facial anhidrosis, and partial ptosis; this is due to the superior cervical ganglia's role in providing sympathetic innervation to these targets.[4][11] These symptoms arise from the disruption of the sympathetic nervous system, which includes superior cervical ganglia. Care is necessary during superior cervical ganglia blocks as well as head and neck procedures to prevent Horner syndrome from occurring.[11]
Other Issues
The superior cervical ganglion can appear as pathologic retropharyngeal lymph nodes on imaging. The superior cervical ganglia are anterior to the retropharyngeal lymph nodes.[1][2] The proximity of the superior cervical ganglia to the retropharyngeal lymph nodes can make the staging of neck neoplasms difficult. Nasopharyngeal cancer, thyroid cancer, as well as oropharyngeal cancer, typically metastasizes to the retropharyngeal lymph nodes, therefore delineating them from the superior cervical ganglia is very important.[1][2][3] Magnetic resonance imaging can be utilized to delineate the difference between pathologic retropharyngeal lymph nodes from the superior ganglia.[1][2]
Media
(Click Image to Enlarge)
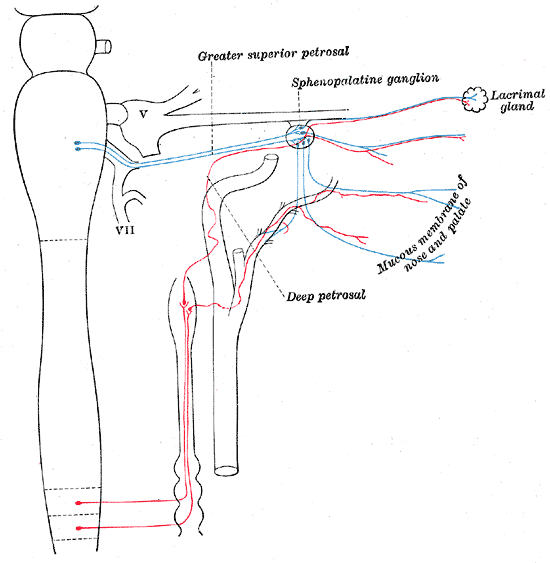
The Sympathetic Nerves, Sympathetic connections of the sphenopalatine and superior cervical ganglia
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
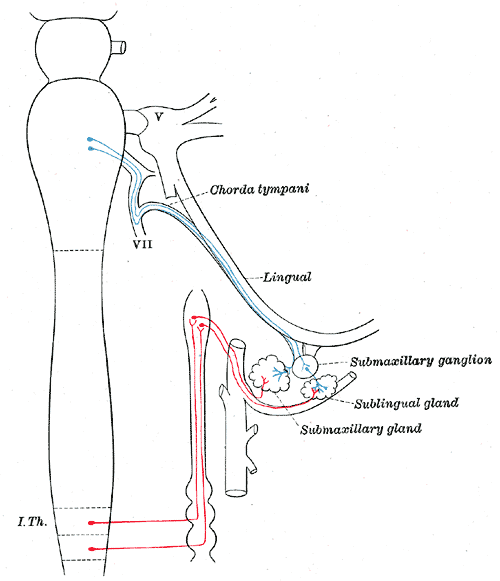
The Sympathetic Nerves, Sympathetic connections of the submaxillary and superior cervical ganglia
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
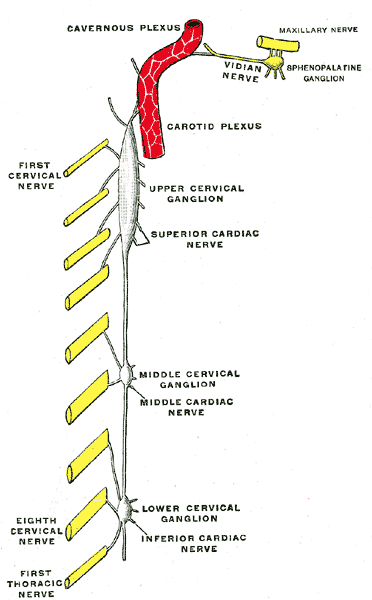
The Cervical Portion of the Sympathetic System, Diagram of the cervical sympathetic
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
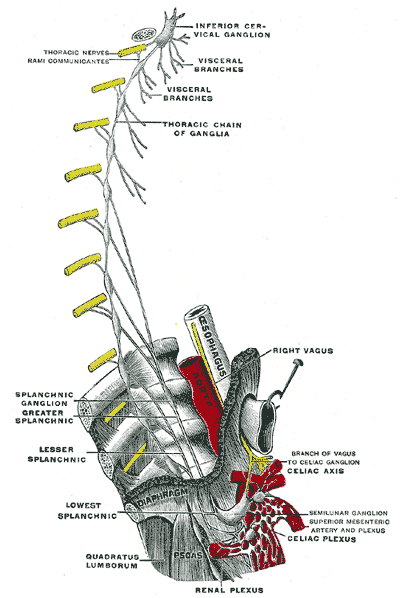
The Cervical Portion of the Sympathetic System, Plan of right sympathetic cord and splanchnic nerves
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Yokota H, Mukai H, Hattori S, Yamada K, Anzai Y, Uno T. MR Imaging of the Superior Cervical Ganglion and Inferior Ganglion of the Vagus Nerve: Structures That Can Mimic Pathologic Retropharyngeal Lymph Nodes. AJNR. American journal of neuroradiology. 2018 Jan:39(1):170-176. doi: 10.3174/ajnr.A5434. Epub 2017 Nov 9 [PubMed PMID: 29122764]
Mitsuoka K, Kikutani T, Sato I. Morphological relationship between the superior cervical ganglion and cervical nerves in Japanese cadaver donors. Brain and behavior. 2017 Feb:7(2):e00619. doi: 10.1002/brb3.619. Epub 2016 Dec 29 [PubMed PMID: 28239529]
Loke SC, Karandikar A, Ravanelli M, Farina D, Goh JP, Ling EA, Maroldi R, Tan TY. Superior cervical ganglion mimicking retropharyngeal adenopathy in head and neck cancer patients: MRI features with anatomic, histologic, and surgical correlation. Neuroradiology. 2016 Jan:58(1):45-50. doi: 10.1007/s00234-015-1598-1. Epub 2015 Sep 30 [PubMed PMID: 26423907]
Fazliogullari Z, Kilic C, Karabulut AK, Yazar F. A morphometric analysis of the superior cervical ganglion and its surrounding structures. Surgical and radiologic anatomy : SRA. 2016 Apr:38(3):299-302. doi: 10.1007/s00276-015-1551-3. Epub 2015 Sep 12 [PubMed PMID: 26364034]
Moriyama H, Shimada K, Goto N. Morphometric analysis of neurons in ganglia: geniculate, submandibular, cervical spinal and superior cervical. Okajimas folia anatomica Japonica. 1995 Oct:72(4):185-90 [PubMed PMID: 8570139]
Rusu MC, Pop F. The anatomy of the sympathetic pathway through the pterygopalatine fossa in humans. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2010 Feb 20:192(1):17-22. doi: 10.1016/j.aanat.2009.10.003. Epub 2009 Nov 5 [PubMed PMID: 19939656]
Kameda Y, Saitoh T, Nemoto N, Katoh T, Iseki S. Hes1 is required for the development of the superior cervical ganglion of sympathetic trunk and the carotid body. Developmental dynamics : an official publication of the American Association of Anatomists. 2012 Aug:241(8):1289-300. doi: 10.1002/dvdy.23819. Epub 2012 Jun 22 [PubMed PMID: 22689348]
Level 3 (low-level) evidenceTubbs RS, Salter G, Wellons JC 3rd, Oakes WJ. Blood supply of the human cervical sympathetic chain and ganglia. European journal of morphology. 2002 Dec:40(5):283-8 [PubMed PMID: 15101443]
Goosmann MM, Dalvin M. Anatomy, Head and Neck, Deep Petrosal Nerve. StatPearls. 2023 Jan:(): [PubMed PMID: 30521238]
Waxenbaum JA, Reddy V, Bordoni B. Anatomy, Head and Neck: Cervical Nerves. StatPearls. 2023 Jan:(): [PubMed PMID: 30844163]
Khan Z, Bollu PC. Horner Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 29763176]
Siegenthaler A, Haug M, Eichenberger U, Suter MR, Moriggl B. Block of the superior cervical ganglion, description of a novel ultrasound-guided technique in human cadavers. Pain medicine (Malden, Mass.). 2013 May:14(5):646-9. doi: 10.1111/pme.12061. Epub 2013 Feb 25 [PubMed PMID: 23438374]