Introduction
Tracheoesophageal fistula (TEF) is one of the most common congenital anomalies in major pediatric surgical centers. Infants with a TEF classically present with respiratory distress, feeding difficulties, choking, and risk for aspiration. TEF is most commonly associated with other congenital anomalies, particularly cardiac defects. Esophageal atresia is a related congenital malformation with a similar presentation to TEF and can occur with or without a fistula.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Although the events leading to the separation of the primitive trachea and esophagus are not entirely understood, the most commonly accepted hypothesis is that a defect in the lateral septation of the foregut into the trachea and esophagus causes TEF and esophageal atresia. The trachea and esophagus develop from a common primitive foregut, and at approximately 4 weeks of gestation, the developing respiratory and gastrointestinal tracts are separated by epithelial ridges. The foregut divides into a ventral respiratory tract and a dorsal esophageal tract. The fistula tract is thought to derive from an embryonic lung bud that fails to undergo branching. These defects of mesenchymal proliferation are supposed to lead to TEF formation.[1]
The VACTERL complex refers to anomalies of the vertebrae (V), anal or gastrointestinal tract atresia (A), congenital cardiac defects (C), tracheoesophageal defects (TE), renal and distal urinary tract anomalies (R), and limb lesions (L). The Sonic Hedgehog (SHH) gene that encodes for an intracellular signaling molecule is implicated in esophageal atresia. Investigators have shown that mice deficient in regulating the SHH gene exhibit VACTERL-type anomalies.[2][3]
Research in rats has also implicated the Adriamycin-induced TEF model. Adriamycin is an anthracycline antibiotic that affects deoxyribonucleic acid integrity and synthesis. The introduction of adriamycin into the peritoneal cavity of pregnant rats results in a 40% to 90% incidence of esophageal atresia and TEF in the developing embryos. Results from studies on these embryos reveal that TEF and esophageal atresia can develop in rats, as in neonates, and VACTERL anomalies can also arise in rats.[4] Gli-2, a downstream signaling molecule for SHH, was investigated in animals with TEF and controls. Gli-2 messenger ribonucleic acid was reduced in the fistula tract compared to the adjacent esophagus.[5]
Epidemiology
Genetic factors do not seem to play a significant role in the pathogenesis of TEF. The concordance rate for twins is 2.5%.[6] The incidence of TEF is approximately 1 in 3500 births.[7][8] Esophageal atresia and TEF are classified according to their anatomic configuration.[9] Type C, which consists of a proximal esophageal pouch and a distal TEF, accounts for 84% of cases. TEF occurs without esophageal atresia (H-type fistula) in only 4% (see Image. Types of Tracheoesophageal Fistulas).[10]
Depaepe et al identified a decreasing incidence in the birth frequency of TEF in different European regions.[11] TEF does not correlate with maternal age if chromosomal anomalies are excluded. The figures for isolated TEF versus an association with other congenital anomalies vary between 38.7% and 57.3%.[12] The incidence of trisomies and other chromosomal abnormalities in association with TEF is between 6% and 10%. Neonates younger than 28 weeks of gestation have been excluded. Though significantly rarer, trisomy 18 is associated with TEF more frequently than trisomy 21. Feingold syndrome, manifesting with microcephaly, micrognathia, and digital anomalies, may have an associated TEF or esophageal atresia.
In 1962, Waterston et al stratified the risk criteria for patients with TEF based on birth weight, pneumonia, and associated anomalies.[13] Later, Spitz et al proposed a less complicated system based on associated congenital heart defects and low birth weight.[14] Survival in babies less than 1500 g and without significant cardiac anomalies now approaches 97% but falls dramatically to 22% if birth weight is low and cardiac anomalies exist. Acute morbidity and mortality are most commonly due to cardiac and chromosomal defects. Late mortality is due to ongoing respiratory complications.[15]
Pathophysiology
TEF occurs due to abnormal septation of the caudal foregut during the fourth and fifth weeks of embryonic development. Under normal conditions, the trachea forms as a diverticulum of the foregut and develops a complete septum that separates it from the esophagus. Fistula formation with esophageal atresia occurs during an abnormal posterior positioning of the tracheoesophageal septum, resulting in a retained connection between the trachea and esophagus. Isolated esophageal atresia without TEF commonly occurs when the esophagus fails to recanalize during week 8 of embryonic development.[16]
History and Physical
Keckler et al noted that TEF was most commonly associated with congenital heart disease in their series, at a rate of 32.1% of patients, excluding infants with patent foramen ovale and patent ductus arteriosus.[17] A ventricular septal defect was most common, occurring in 22.3% of patients, in association with multiple cardiac defects. An isolated ventricular septal defect occurred in only 7.1%. Cyanotic heart disease was uncommon, noted in 4.5% of patients, and all exhibited tetralogy of Fallot.
The next most commonly associated congenital defect with TEF was reported to be vertebral anomalies, seen in 24% of patients. Most vertebral defects commonly occur with other axial spine complications, including rib anomalies and a tethered cord. Axial spine abnormalities were associated with an increased anastomotic leak rate, likely due to greater tension at the site. Theoretically, a wider gap may exist between the 2 ends of the esophagus due to a higher proximal pouch in patients with this skeletal deformity.[18]
The clinical presentation of TEF depends on the presence of esophageal atresia. Polyhydramnios occurs in two-thirds of pregnancies, although many cases are not detected prenatally.[19] Newborns with esophageal atresia present immediately after birth with excessive secretions that cause drooling, choking, respiratory distress, and feeding inability. Gastric distension is a common fistula complication between the trachea and distal esophagus. Reflux of gastric contents through the fistula tract results in aspiration pneumonia and increasing morbidity.
Patients with H-type TEFs may present early if the defect is significant, primarily with coughing and choking associated with aspiration of feeds through the fistula. However, according to one series, minor H-type defects may not be symptomatic in the newborn period, and diagnosis may even be delayed from 26 days to 4 years.[20] These patients may have a prolonged history of mild respiratory distress associated with feeding or recurrent episodes of pneumonia. In rare cases, the diagnosis may be delayed into adulthood.[21]
Evaluation
TEF may be suspected prenatally from maternal polyhydramnios and the absence of the fetal stomach bubble. Results from a study by Stringer et al revealed that prenatal scans diagnosing esophageal atresia had a sensitivity of 42% with a positive predictive value of 56%.[22] Karyotyping may be helpful in the prenatal diagnosis of esophageal atresia due to the high reported incidence of trisomy 18 in affected infants. Ultrasound imaging may also reveal cardiac defects, which indicate a worse fetal prognosis.[23]
If esophageal atresia or TEF is suspected, delivery should be planned at an obstetrical center with access to a neonatal intensive care unit and an operating room. Esophageal atresia and TEF are commonly associated with the VACTERL sequence, CHARGE syndrome (coloboma of the eye, heart defects, atresia of the choanae, retarded development, genital hypoplasia, and ear abnormalities), trisomies 18 and 21, and DiGeorge syndrome. An increased incidence of anomalies is associated with up to 65% of pure esophageal atresia. The risk of recurrence in subsequent pregnancies for nonsyndromic esophageal atresia or TEF is 1%.[24]
Esophageal atresia may be diagnosed when an orogastric or nasogastric catheter cannot be passed further than 10 to 15 cm into the stomach. This finding may be confirmed with an anterior-posterior chest radiograph demonstrating the catheter curled in the upper esophageal pouch. A distal TEF can be seen on a lateral chest radiograph. Both views typically reveal a gas-filled gastrointestinal tract. Water-soluble contrast can be instilled into the esophageal pouch under fluoroscopic guidance to evaluate for TEF.[25] Barium contrast should be avoided as it causes pneumonitis if aspirated. Contrast material must be immediately removed to prevent regurgitation and aspiration.
The diagnosis of isolated TEF should be attempted with an upper gastrointestinal series using thickened water-soluble contrast material. The distal esophagus is filled first, and then the catheter is pulled in a cephalad direction. Contrast swallow radiography may also be helpful, but the fistulous tract may be difficult to identify in these studies.[26] Esophageal endoscopy and bronchoscopy should be used to detect the TEF. Methylene blue can be injected into the trachea, and the fistula should be apparent by its appearance in the esophagus. Three-dimensional computed tomography (CT) scanning has also been utilized to diagnose TEF.[27]
Treatment / Management
The first successful primary repair of TEF was performed by an American surgeon, Cameron Haight, in 1941.[28] Because pediatric surgical centers now have a survival rate greater than 90% for patients with this condition, the emphasis is now on reducing morbidity and enhancing these patients’ quality of life. Open surgical repair of TEF and esophageal atresia involves a right posterolateral thoracotomy, fistula ligation, and the creation of a primary esophageal anastomosis. Preoperative evaluation with an echocardiogram is essential, as a right-sided aortic arch, seen in 2.5% of cases, signifies a higher morbidity rate and necessitates a left thoracotomy.[29] A renal ultrasoueend, spinal ultrasound, and limb radiographs may rule out other VACTERL anomalies.(B2)
Complications of primary repair include anastomotic leak, recurrent laryngeal nerve injury with resulting vocal cord paralysis, esophageal stricture, a persistent sec upper pouch fistula, recurrent fistula, and death.[30] Spontaneous closure of a recurrent TEF is exceedingly rare.[31] Most commonly, a primary anastomosis cannot be achieved when greater than 2 vertebral bodies separate the upper and lower esophageal segments. In this instance, surgical options include Livaditis myotomy, mobilization of the distal esophageal segment to the diaphragmatic hiatus, and the Foker technique.(B2)
An esophageal anastomosis created under tension puts the patient at risk for an increased leak rate, esophageal stricture, and reflux disease.[32] Sixty years after the first successful primary repair, Tom Lobe and Steve Rothenberg accomplished the first minimally invasive thoracoscopic TEF repair.[33] Minimally invasive techniques should only be performed at advanced pediatric surgical institutions and have not been proven to decrease the potential for stricture and anastomotic leaks.[34] Thoracoscopic surgery provides excellent visibility of anatomic structures and decreases morbidity if performed adequately due to the avoidance of open thoracotomy. Avoidance of open surgical repair also prevents potential chest wall deformity, scoliosis, fusion of ribs, muscle contractures, and chronic pain.[35](B2)
Immediate surgical management involves the creation of a gastrostomy for feeding and continuous suctioning of the blind esophageal pouch to protect the patient from aspiration. Options for reconstruction include primary repair using the native esophagus or replacement procedures with parts of the stomach or large intestine. Preserving the native esophagus is ideal, as replacement procedures increase the risk of recurrent aspiration and chronic respiratory complications. A staged procedure can be performed as the infant ages, and the esophagus elongates if primary repair is not feasible.[36]
The esophageal segment can be mechanically elongated with procedures such as bougienage, electromagnetic stimulation, and graded tension applied to the disconnected esophageal segment using traction sutures, although success remains unproven.[37] A staged approach has improved outcomes in infants with meager birth weight. H-type fistula repair is performed via a cervical neck dissection to expose where the fistula is to be divided and repaired. This surgical procedure incurs the risk of recurrent laryngeal nerve injury and operative trauma.[38] The neodymium-doped yttrium aluminum garnet (Nd:YAG) laser has also been utilized for H-type fistula repair, with limited experience.[39](B2)
Meier et al [40] describe the endoscopic repair of TEF with tissue adhesive (Histoacryl: B. Braun Melsungen AG, Mesungen, Germany) and fibrin adhesive (TisseelTM), with success rates of 48% (29 patients) and 55% (22 patients), respectively. Five patients in the tissue adhesive group also had a sclerosing agent (polidocanol or aethoxysklerol) applied during endoscopic repair with a success rate of 100%. The morbidity from endoscopic repair is minimal to none.[41](B3)
Hoelzer et al also describe 2 of 3 successful recurrent TEF closures with the bronchoscopic application of fibrin glue, an organic compound causing rapid granulation tissue formation and early epithelialization.[42] Endoscopic repair of recurrent TEF was first described in the 1970s using tissue adhesive (Histoacryl), where numerous attempts led to the successful closure of the fistula.[43] A rigid bronchoscope is the device of choice to enable the successful delivery of the obliterating agent. Rod-lens telescopes are particularly useful for the diagnosis of H-type fistulas.(B3)
All infants should have laryngoscopy and bronchoscopy before an open surgical repair of TEF or esophageal atresia. Laryngoscopy and bronchoscopy are used to identify the level of the fistula, as well as tracheomalacia and tracheobronchitis, before primary repair. Bronchoscopy may also elucidate laryngeal abnormalities, including a posterior laryngeal cleft, laryngomalacia, vocal cord dysfunction, the position of the aortic arch, and other fistulas.[44] Bronchoscopic findings help plan surgical repair. Carinal fistulas are associated with wide-gap atresia, and midtracheal fistulas are associated with minimal-gap atresia.
Because gastroesophageal reflux disease (GERD) is common following repair, an expert panel has recommended that infants with repaired TEF be routinely treated with a proton pump inhibitor (PPI) for at least a year after repair and longer for those with evidence of ongoing GERD. Infants with TEF are also at increased risk for chronic feeding difficulties. GERD persists in most patients and is associated with Barrett esophagitis. This panel has recommended that children with repaired TEFs be monitored for pulmonary and gastrointestinal complications throughout childhood.[45]
Differential Diagnosis
The differential diagnosis of TEF and esophageal atresia includes esophageal stricture or diverticulum, pharyngeal pseudodiverticulum, severe GERD, vascular ring, iatrogenic esophageal perforation, laryngotracheoesophageal cleft, esophageal webs, esophageal duplication, congenital shortened esophagus, and tracheal agenesis or atresia.
Prognosis
The prognosis for isolated TEF is generally good.[46] Infants with TEF and esophageal atresia have a more guarded prognosis, depending on the presence of associated abnormalities. In one report, 87% of patients with esophageal atresia or esophageal atresia and TEF survived, although 61% of early deaths were associated with cardiac and chromosomal anomalies.[47][48] Mortality rates for esophageal atresia and TEF were greater for infants with associated cardiac disease (42% with versus 12% without). One review reported very low birth weight as a significant factor in reduced patient survival.[49] The gap length of the esophageal atresia may also determine the patient's prognosis.[50]
Children with esophageal atresia and TEF tend to have considerable deficiencies in their growth. Poor in-utero development has been noted, with almost one-third having birth weights less than the fifth percentile.[51] Little et al reported that up to 50% of children had weights less than the 25th percentile during the first 5 years of life.[52] This trend was primarily due to significant respiratory and gastrointestinal morbidity associated with TEF.
Long-term height and weight outcomes are overwhelmingly positive as these children age.[53] Feeding abnormalities are an important cause of morbidity during early childhood. A subgroup of patients have aversive feeding behavior with refusal to eat orally due to GERD, anastomotic strictures, and esophageal dysmotility. Children with such complications require gastrostomy tube placement for aggressive nutritional supplementation. Feeding aversion is more common in children with isolated esophageal atresia because they are exclusively fed via a gastrostomy tube in the first few months of life.
Respiratory complications are also common in children with TEF and esophageal atresia. Severe tracheomalacia and bronchomalacia occur in 10% to 20% of infants. Airway reactivity and instability can lead to life-threatening airway obstruction.[54] A small subset of infants will require aortopexy for tracheal stabilization and weaning from mechanical ventilation.
Children may exhibit a harsh barking cough, which is characteristic of iatrochemicals. Children may also suffer from recurrent bronchitis and pneumonia, common in up to two-thirds of TEF patients in the first few years of life.[55] If left untreated, recurrent infections or frequent aspiration can lead to irreversible lung damage with bronchiectasis and persistent atelectasis. Wheezing is common in up to 40% of survivors and does not improve with age. Recurrent respiratory symptoms are caused by abnormal airway epithelium, which impairs mucociliary clearance of airway secretions. The severity of GERD will increase the risk for esophageal strictures and dysmotility, thereby potentiating aspiration in such patients. Rarely, persistence or worsening of symptoms may be due to recurrent TEF.
Respiratory morbidity decreases in frequency and severity once children reach late adolescence.[55] Hyperinflation of the lungs, reduced lung volumes, and overall abnormal pulmonary function are common in up to 40% of survivors, but some do not affect children’s daily activities. Management of pulmonary pathology includes tailored use of antibiotics, physiotherapy, and GERD treatment to prevent aspiration. Inhaled bronchodilators and steroids help treat asthmatic symptoms. Serial pulmonary function tests and chest CT scans help monitor patient progress.[56]
Complications
Common complications after esophageal atresia and TEF repair in a series of 227 cases included anastomotic leak (16%), esophageal stricture (35%), and recurrent fistulae (3%). Esophageal stricture has been successfully managed with endoscopic balloon dilation.[57] Tracheomalacia occurred in 15% of cases, with 40% of patients requiring surgical repair. Disturbed peristalsis and delayed gastric emptying are typical and contribute to GERD and aspiration. Strictures at the anastomotic site are an early complication requiring dilatation in nearly half of all patients.[58] A minority require resection of the strictured esophageal segment. GERD can significantly increase the risk of stricture formation, but fundoplication may be helpful.
Esophageal dysmotility is an expected finding and can be visualized on manometry in 75% to 100% of children after primary repair.[59] Patients often experience dysphagia, obstruction of food particles, failure to thrive, and choking.[60] Dietary modification is helpful in these instances, including avoiding certain foods and frequent drinking when eating.
Open thoracotomy can lead to significant musculoskeletal morbidity. Vertebral defects associated with the VACTERL sequence can contribute to chest wall or spinal deformities. One report noted that 24% of patients had a winged scapula due to latissimus dorsi muscle paralysis. In contrast, 20% of children exhibited chest wall asymmetry secondary to atrophy of the serratus anterior muscle.[61] Girl infants may have breast asymmetry with disfigurement.[62] Modified axillary incisions described by Bianchi et al or thoracoscopic techniques may reduce morbidity.[63]
Motility disorders and respiratory function abnormalities are common after esophageal atresia and TEF repair and warrant monitoring. A systematic review of long-term outcomes in adulthood after esophageal atresia repair during infancy reported the following pooled estimated prevalences:
- Dysphagia: 50.3%
- GERD with esophagitis: 40.2%
- GERD without esophagitis: 56.5%
- Respiratory tract infections: 24.1%
- Asthma: 22.3%
- Wheeze: 34.7%
- Persistent cough: 14.6%
- Barrett esophagus: 6.4%
- Squamous cell esophageal cancer: 1.4%
The prevalence of Barrett esophagus in adulthood was 4 times that of the general population, and it is a recognized risk factor for esophageal cancer.[64] The risk of esophageal cancer is approximately 50 times that in the general population over 40.[65]
Postoperative and Rehabilitation Care
Postoperative laryngoscopy and bronchoscopy are used to determine tracheomalacia's severity and identify missed and recurrent fistulae.[66]
Enhancing Healthcare Team Outcomes
Persistent respiratory and gastrointestinal complications are common in patients with TEF repair. Long-term management focuses on early detection and aggressive management of these common complications, led by an interprofessional team of pediatric surgeons, pulmonologists, gastroenterologists, otolaryngologists, and neonatal intensive care unit nurses.[67] Patients and families should be educated about these health risks and the importance of clinical and endoscopic surveillance into adulthood. Specific recommendations have been made by a panel, primarily based on expert opinion:
- All children and adults should be routinely monitored for symptoms of GERD, dysphagia, and aspiration.
- All patients should undergo at least 3 surveillance endoscopies during childhood to detect early esophagitis. Routine endoscopic surveillance should be continued in adulthood, every 5 to 10 years.
- Patients with symptoms of GERD or dysphagia should be evaluated with an esophageal contrast study and endoscopy. Esophagitis should be managed aggressively with proton pump inhibitors (PPIs). Esophageal strictures should be treated with dilation and PPIs. Patients who are asymptomatic do not require routine screening or dilation for strictures.
- Respiratory symptoms should be carefully evaluated for anastomotic stricture, laryngeal cleft, vocal cord paralysis, congenital esophageal stenosis, recurrent fistula, or congenital vascular malformations. Acid suppression alone probably does not improve respiratory symptoms and may predispose to respiratory infection.
- Fundoplication has a limited role in patients with TEF because their underlying esophageal dysmotility predisposes them to post-fundoplication complications, including esophageal stasis and aspiration. However, fundoplication may be considered in patients with poorly controlled GERD despite maximal PPI therapy, long-term dependency on transpyloric feeding, or cyanotic spells due to GERD. Eosinophilic esophagitis should be excluded before proceeding to fundoplication.
Managing TEF requires a well-coordinated interprofessional team to ensure complete care and optimal outcomes for the patient. The collaborative approach to TEF management ensures that all aspects of the patient’s condition are addressed, from diagnosis and surgery to postoperative care and long-term follow-up, improving the overall prognosis and quality of life for children with this condition.
Media
(Click Image to Enlarge)
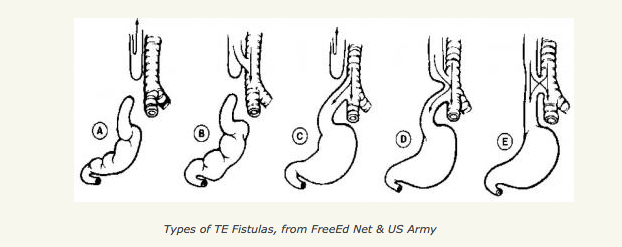
Types of Tracheoesophageal Fistulas. This image shows the differences between tracheoesophageal fistula subtypes.
Free-Ed.Net & The US Army
References
Crisera CA, Grau JB, Maldonado TS, Kadison AS, Longaker MT, Gittes GK. Defective epithelial-mesenchymal interactions dictate the organogenesis of tracheoesophageal fistula. Pediatric surgery international. 2000:16(4):256-61 [PubMed PMID: 10898225]
Level 3 (low-level) evidenceNgan ES, Kim KH, Hui CC. Sonic Hedgehog Signaling and VACTERL Association. Molecular syndromology. 2013 Feb:4(1-2):32-45. doi: 10.1159/000345725. Epub [PubMed PMID: 23653575]
Walk RM. Esophageal Atresia and Tracheoesophageal Fistula: Overview and Considerations for the General Surgeon. The Surgical clinics of North America. 2022 Oct:102(5):759-778. doi: 10.1016/j.suc.2022.07.008. Epub 2022 Sep 7 [PubMed PMID: 36209744]
Level 3 (low-level) evidenceDiez-Pardo JA, Baoquan Q, Navarro C, Tovar JA. A new rodent experimental model of esophageal atresia and tracheoesophageal fistula: preliminary report. Journal of pediatric surgery. 1996 Apr:31(4):498-502 [PubMed PMID: 8801299]
Level 3 (low-level) evidenceSpilde T, Bhatia A, Ostlie D, Marosky J, Holcomb G 3rd, Snyder C, Gittes G. A role for sonic hedgehog signaling in the pathogenesis of human tracheoesophageal fistula. Journal of pediatric surgery. 2003 Mar:38(3):465-8 [PubMed PMID: 12632368]
Robert E, Mutchinick O, Mastroiacovo P, Knudsen LB, Daltveit AK, Castilla EE, Lancaster P, Källén B, Cocchi G. An international collaborative study of the epidemiology of esophageal atresia or stenosis. Reproductive toxicology (Elmsford, N.Y.). 1993 Sep-Oct:7(5):405-21 [PubMed PMID: 8274816]
Level 2 (mid-level) evidenceHarper PS. Some pioneers of European human genetics. European journal of human genetics : EJHG. 2017 May 10:():. doi: 10.1038/ejhg.2017.47. Epub 2017 May 10 [PubMed PMID: 28488680]
McGowan NA, Grosel J. An overview of esophageal atresia and tracheoesophageal fistula. JAAPA : official journal of the American Academy of Physician Assistants. 2022 Jun 1:35(6):34-37. doi: 10.1097/01.JAA.0000830180.79745.b9. Epub [PubMed PMID: 35617475]
Level 3 (low-level) evidenceFelix JF, de Jong EM, Torfs CP, de Klein A, Rottier RJ, Tibboel D. Genetic and environmental factors in the etiology of esophageal atresia and/or tracheoesophageal fistula: an overview of the current concepts. Birth defects research. Part A, Clinical and molecular teratology. 2009 Sep:85(9):747-54. doi: 10.1002/bdra.20592. Epub [PubMed PMID: 19452513]
Level 3 (low-level) evidenceClark DC. Esophageal atresia and tracheoesophageal fistula. American family physician. 1999 Feb 15:59(4):910-6, 919-20 [PubMed PMID: 10068713]
Level 3 (low-level) evidenceDepaepe A, Dolk H, Lechat MF. The epidemiology of tracheo-oesophageal fistula and oesophageal atresia in Europe. EUROCAT Working Group. Archives of disease in childhood. 1993 Jun:68(6):743-8 [PubMed PMID: 8333763]
Torfs CP, Curry CJ, Bateson TF. Population-based study of tracheoesophageal fistula and esophageal atresia. Teratology. 1995 Oct:52(4):220-32 [PubMed PMID: 8838292]
Level 2 (mid-level) evidenceWATERSTON DJ, BONHAM-CARTER RE, ABERDEEN E. Congenital tracheo-oesophageal fistula in association with oesophageal atresia. Lancet (London, England). 1963 Jul 13:2(7298):55-7 [PubMed PMID: 13999160]
Spitz L, Kiely EM, Morecroft JA, Drake DP. Oesophageal atresia: at-risk groups for the 1990s. Journal of pediatric surgery. 1994 Jun:29(6):723-5 [PubMed PMID: 8078005]
Choudhury SR, Ashcraft KW, Sharp RJ, Murphy JP, Snyder CL, Sigalet DL. Survival of patients with esophageal atresia: influence of birth weight, cardiac anomaly, and late respiratory complications. Journal of pediatric surgery. 1999 Jan:34(1):70-3; discussion 74 [PubMed PMID: 10022146]
Level 2 (mid-level) evidenceGoyal A, Jones MO, Couriel JM, Losty PD. Oesophageal atresia and tracheo-oesophageal fistula. Archives of disease in childhood. Fetal and neonatal edition. 2006 Sep:91(5):F381-4 [PubMed PMID: 16923940]
Keckler SJ, St Peter SD, Valusek PA, Tsao K, Snyder CL, Holcomb GW 3rd, Ostlie DJ. VACTERL anomalies in patients with esophageal atresia: an updated delineation of the spectrum and review of the literature. Pediatric surgery international. 2007 Apr:23(4):309-13 [PubMed PMID: 17377826]
Level 2 (mid-level) evidenceTouloukian RJ, Keller MS. High proximal pouch esophageal atresia with vertebral, rib, and sternal anomalies: an additional component to the VATER association. Journal of pediatric surgery. 1988 Jan:23(1 Pt 2):76-9 [PubMed PMID: 3351734]
Pretorius DH, Drose JA, Dennis MA, Manchester DK, Manco-Johnson ML. Tracheoesophageal fistula in utero. Twenty-two cases. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 1987 Sep:6(9):509-13 [PubMed PMID: 3312629]
Level 2 (mid-level) evidenceKarnak I, Senocak ME, Hiçsönmez A, Büyükpamukçu N. The diagnosis and treatment of H-type tracheoesophageal fistula. Journal of pediatric surgery. 1997 Dec:32(12):1670-4 [PubMed PMID: 9433996]
Level 2 (mid-level) evidenceZacharias J, Genc O, Goldstraw P. Congenital tracheoesophageal fistulas presenting in adults: presentation of two cases and a synopsis of the literature. The Journal of thoracic and cardiovascular surgery. 2004 Aug:128(2):316-8 [PubMed PMID: 15282472]
Level 3 (low-level) evidenceStringer MD, McKenna KM, Goldstein RB, Filly RA, Adzick NS, Harrison MR. Prenatal diagnosis of esophageal atresia. Journal of pediatric surgery. 1995 Sep:30(9):1258-63 [PubMed PMID: 8523220]
Level 2 (mid-level) evidenceSparey C, Jawaheer G, Barrett AM, Robson SC. Esophageal atresia in the Northern Region Congenital Anomaly Survey, 1985-1997: prenatal diagnosis and outcome. American journal of obstetrics and gynecology. 2000 Feb:182(2):427-31 [PubMed PMID: 10694347]
Level 2 (mid-level) evidenceOkamoto T, Takamizawa S, Arai H, Bitoh Y, Nakao M, Yokoi A, Nishijima E. Esophageal atresia: prognostic classification revisited. Surgery. 2009 Jun:145(6):675-81. doi: 10.1016/j.surg.2009.01.017. Epub 2009 Apr 11 [PubMed PMID: 19486772]
Reed MF, Mathisen DJ. Tracheoesophageal fistula. Chest surgery clinics of North America. 2003 May:13(2):271-89 [PubMed PMID: 12755313]
Laffan EE, Daneman A, Ein SH, Kerrigan D, Manson DE. Tracheoesophageal fistula without esophageal atresia: are pull-back tube esophagograms needed for diagnosis? Pediatric radiology. 2006 Nov:36(11):1141-7 [PubMed PMID: 16967270]
Level 2 (mid-level) evidenceNagata K, Kamio Y, Ichikawa T, Kadokura M, Kitami A, Endo S, Inoue H, Kudo SE. Congenital tracheoesophageal fistula successfully diagnosed by CT esophagography. World journal of gastroenterology. 2006 Mar 7:12(9):1476-8 [PubMed PMID: 16552825]
Level 3 (low-level) evidenceHaight C. Congenital Atresia of the Esophagus With Tracheoesophageal Fistula : Reconstruction of Esophageal Continuity by Primary Anastomosis. Annals of surgery. 1944 Oct:120(4):623-52 [PubMed PMID: 17858517]
Babu R, Pierro A, Spitz L, Drake DP, Kiely EM. The management of oesophageal atresia in neonates with right-sided aortic arch. Journal of pediatric surgery. 2000 Jan:35(1):56-8 [PubMed PMID: 10646774]
Level 2 (mid-level) evidenceEngum SA, Grosfeld JL, West KW, Rescorla FJ, Scherer LR 3rd. Analysis of morbidity and mortality in 227 cases of esophageal atresia and/or tracheoesophageal fistula over two decades. Archives of surgery (Chicago, Ill. : 1960). 1995 May:130(5):502-8; discussion 508-9 [PubMed PMID: 7748088]
Level 3 (low-level) evidenceEin SH, Stringer DA, Stephens CA, Shandling B, Simpson J, Filler RM. Recurrent tracheoesophageal fistulas seventeen-year review. Journal of pediatric surgery. 1983 Aug:18(4):436-41 [PubMed PMID: 6620086]
Level 2 (mid-level) evidenceHagberg S, Rubenson A, Sillén U, Werkmäster K. Management of long-gap esophagus: experience with end-to-end anastomosis under maximal tension. Progress in pediatric surgery. 1986:19():88-92 [PubMed PMID: 3081964]
Rothenberg SS. Thoracoscopic management of non-type C esophageal atresia and tracheoesophageal atresia. Journal of pediatric surgery. 2017 Oct 12:():. pii: S0022-3468(17)30647-4. doi: 10.1016/j.jpedsurg.2017.10.025. Epub 2017 Oct 12 [PubMed PMID: 29092772]
Rothenberg SS. Thoracoscopic repair of esophageal atresia and tracheo-esophageal fistula. Seminars in pediatric surgery. 2005 Feb:14(1):2-7 [PubMed PMID: 15770583]
Level 2 (mid-level) evidenceHolcomb GW 3rd, Rothenberg SS, Bax KM, Martinez-Ferro M, Albanese CT, Ostlie DJ, van Der Zee DC, Yeung CK. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. Annals of surgery. 2005 Sep:242(3):422-8; discussion 428-30 [PubMed PMID: 16135928]
Level 2 (mid-level) evidencePuri P, Ninan GK, Blake NS, Fitzgerald RJ, Guiney EJ, O'Donnell B. Delayed primary anastomosis for esophageal atresia: 18 months' to 11 years' follow-up. Journal of pediatric surgery. 1992 Aug:27(8):1127-30 [PubMed PMID: 1403548]
Foker JE, Kendall TC, Catton K, Khan KM. A flexible approach to achieve a true primary repair for all infants with esophageal atresia. Seminars in pediatric surgery. 2005 Feb:14(1):8-15 [PubMed PMID: 15770584]
Level 2 (mid-level) evidenceGoyal A, Potter F, Losty PD. Transillumination of H-type tracheoesophageal fistula using flexible miniature bronchoscopy: an innovative technique for operative localization. Journal of pediatric surgery. 2005 Jun:40(6):e33-4 [PubMed PMID: 15991163]
Bhatnagar V, Lal R, Sriniwas M, Agarwala S, Mitra DK. Endoscopic treatment of tracheoesophageal fistula using electrocautery and the Nd:YAG laser. Journal of pediatric surgery. 1999 Mar:34(3):464-7 [PubMed PMID: 10211655]
Meier JD, Sulman CG, Almond PS, Holinger LD. Endoscopic management of recurrent congenital tracheoesophageal fistula: a review of techniques and results. International journal of pediatric otorhinolaryngology. 2007 May:71(5):691-7 [PubMed PMID: 17408757]
Level 3 (low-level) evidenceHolland AJ, Ford WD, Guerin RL. Median sternotomy and use of a pedicled sternocleidomastoid muscle flap in the management of recurrent tracheoesophageal fistula. Journal of pediatric surgery. 1998 Apr:33(4):657-9 [PubMed PMID: 9574775]
Level 3 (low-level) evidenceHoelzer DJ, Luft JD. Successful long-term endoscopic closure of a recurrent tracheoesophageal fistula with fibrin glue in a child. International journal of pediatric otorhinolaryngology. 1999 May 25:48(3):259-63 [PubMed PMID: 10402124]
Level 3 (low-level) evidenceGdanietz K, Wiesner B, Krause I, Mau H, Jung FJ. [Tissue-adhesive for sealing of oesophagotracheal fistulae in children (author's transl)]. Zeitschrift fur Erkrankungen der Atmungsorgane. 1974:141(1):46-50 [PubMed PMID: 4460420]
HOLINGER PH, BROWN WT, MAURIZI DG. ENDOSCOPIC ASPECTS OF POST-SURGICAL MANAGEMENT OF CONGENITAL ESOPHAGEAL ATRESIA AND TRACHEOESOPHAGEAL FISTULA. The Journal of thoracic and cardiovascular surgery. 1965 Jan:49():22-32 [PubMed PMID: 14261873]
Krishnan U, Mousa H, Dall'Oglio L, Homaira N, Rosen R, Faure C, Gottrand F. ESPGHAN-NASPGHAN Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children With Esophageal Atresia-Tracheoesophageal Fistula. Journal of pediatric gastroenterology and nutrition. 2016 Nov:63(5):550-570 [PubMed PMID: 27579697]
Teich S, Barton DP, Ginn-Pease ME, King DR. Prognostic classification for esophageal atresia and tracheoesophageal fistula: Waterston versus Montreal. Journal of pediatric surgery. 1997 Jul:32(7):1075-9; discussion 1079-80 [PubMed PMID: 9247237]
Feng C, Li L, Zhang Y, Zhao Y, Huang J. Diagnosis and management of congenital type D esophageal atresia. Pediatric surgery international. 2023 Oct 10:39(1):280. doi: 10.1007/s00383-023-05519-6. Epub 2023 Oct 10 [PubMed PMID: 37815659]
Gutierrez RS, Guelfand M, Balbontin PV. Congenital and acquired tracheoesophageal fistulas in children. Seminars in pediatric surgery. 2021 Jun:30(3):151060. doi: 10.1016/j.sempedsurg.2021.151060. Epub 2021 May 21 [PubMed PMID: 34172208]
Konkin DE, O'hali WA, Webber EM, Blair GK. Outcomes in esophageal atresia and tracheoesophageal fistula. Journal of pediatric surgery. 2003 Dec:38(12):1726-9 [PubMed PMID: 14666453]
Upadhyaya VD, Gangopadhyaya AN, Gupta DK, Sharma SP, Kumar V, Pandey A, Upadhyaya AD. Prognosis of congenital tracheoesophageal fistula with esophageal atresia on the basis of gap length. Pediatric surgery international. 2007 Aug:23(8):767-71 [PubMed PMID: 17579871]
David TJ, O'Callaghan SE. Oesophageal atresia in the South West of England. Journal of medical genetics. 1975 Mar:12(1):1-11 [PubMed PMID: 1121014]
Little DC, Rescorla FJ, Grosfeld JL, West KW, Scherer LR, Engum SA. Long-term analysis of children with esophageal atresia and tracheoesophageal fistula. Journal of pediatric surgery. 2003 Jun:38(6):852-6 [PubMed PMID: 12778380]
Chetcuti P, Phelan PD. Gastrointestinal morbidity and growth after repair of oesophageal atresia and tracheo-oesophageal fistula. Archives of disease in childhood. 1993 Feb:68(2):163-6 [PubMed PMID: 8481035]
Spitz L. Esophageal atresia and tracheoesophageal fistula in children. Current opinion in pediatrics. 1993 Jun:5(3):347-52 [PubMed PMID: 8374655]
Level 3 (low-level) evidenceChetcuti P, Phelan PD. Respiratory morbidity after repair of oesophageal atresia and tracheo-oesophageal fistula. Archives of disease in childhood. 1993 Feb:68(2):167-70 [PubMed PMID: 8481036]
Chetcuti P, Phelan PD, Greenwood R. Lung function abnormalities in repaired oesophageal atresia and tracheo-oesophageal fistula. Thorax. 1992 Dec:47(12):1030-4 [PubMed PMID: 1494766]
Antoniou D, Soutis M, Christopoulos-Geroulanos G. Anastomotic strictures following esophageal atresia repair: a 20-year experience with endoscopic balloon dilatation. Journal of pediatric gastroenterology and nutrition. 2010 Oct:51(4):464-7. doi: 10.1097/MPG.0b013e3181d682ac. Epub [PubMed PMID: 20562719]
Level 2 (mid-level) evidencede Lagausie P. GER in oesophageal atresia: surgical options. Journal of pediatric gastroenterology and nutrition. 2011 May:52 Suppl 1():S27-8. doi: 10.1097/MPG.0b013e3182133155. Epub [PubMed PMID: 21499041]
Somppi E, Tammela O, Ruuska T, Rahnasto J, Laitinen J, Turjanmaa V, Järnberg J. Outcome of patients operated on for esophageal atresia: 30 years' experience. Journal of pediatric surgery. 1998 Sep:33(9):1341-6 [PubMed PMID: 9766349]
LeSouëf PN, Myers NA, Landau LI. Etiologic factors in long-term respiratory function abnormalities following esophageal atresia repair. Journal of pediatric surgery. 1987 Oct:22(10):918-22 [PubMed PMID: 3681622]
Jaureguizar E, Vazquez J, Murcia J, Diez Pardo JA. Morbid musculoskeletal sequelae of thoracotomy for tracheoesophageal fistula. Journal of pediatric surgery. 1985 Oct:20(5):511-4 [PubMed PMID: 4057018]
Cherup LL, Siewers RD, Futrell JW. Breast and pectoral muscle maldevelopment after anterolateral and posterolateral thoracotomies in children. The Annals of thoracic surgery. 1986 May:41(5):492-7 [PubMed PMID: 3707242]
Level 2 (mid-level) evidenceBianchi A, Sowande O, Alizai NK, Rampersad B. Aesthetics and lateral thoracotomy in the neonate. Journal of pediatric surgery. 1998 Dec:33(12):1798-800 [PubMed PMID: 9869054]
Level 3 (low-level) evidenceConnor MJ, Springford LR, Kapetanakis VV, Giuliani S. Esophageal atresia and transitional care--step 1: a systematic review and meta-analysis of the literature to define the prevalence of chronic long-term problems. American journal of surgery. 2015 Apr:209(4):747-59. doi: 10.1016/j.amjsurg.2014.09.019. Epub 2014 Dec 4 [PubMed PMID: 25605033]
Level 1 (high-level) evidenceJayasekera CS, Desmond PV, Holmes JA, Kitson M, Taylor AC. Cluster of 4 cases of esophageal squamous cell cancer developing in adults with surgically corrected esophageal atresia--time for screening to start. Journal of pediatric surgery. 2012 Apr:47(4):646-51. doi: 10.1016/j.jpedsurg.2011.09.065. Epub [PubMed PMID: 22498376]
Level 2 (mid-level) evidenceFEARON B. The endoscopic management of congenital atresia of the esophagus with or without tracheo-esophageal fistula and of congenital tracheo-esophageal fistula without atresia of the esophagus. The Annals of otology, rhinology, and laryngology. 1959 Dec:68():1047-68 [PubMed PMID: 13821822]
DeBoer EM, Prager JD, Ruiz AG, Jensen EL, Deterding RR, Friedlander JA, Soden J. Multidisciplinary care of children with repaired esophageal atresia and tracheoesophageal fistula. Pediatric pulmonology. 2016 Jun:51(6):576-81. doi: 10.1002/ppul.23330. Epub 2015 Sep 30 [PubMed PMID: 26422584]