 Anatomy, Shoulder and Upper Limb, Forearm Triangular Fibrocartilage Complex
Anatomy, Shoulder and Upper Limb, Forearm Triangular Fibrocartilage Complex
Introduction
The triangular fibrocartilage complex (TFCC) is a significant structure in the ulnar side of the wrist. Serving as the primary stabilizer of the distal radius ulnar joint (DRUJ), it also acts as a load-bearing structure. It divides into two parts, a relatively avascular central cartilaginous portion, and a peripheral highly vascular ligamentous part. It arises from the radius and inserts on the distal ulna and ulnar carpus. It can often be a cause of ulnar sided wrist pain, with injury classified as traumatic or degenerative.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
This complex (TFCC) includes the triangular fibrocartilage disc proper (TFC), a meniscus homolog (MH), radioulnar ligaments (RUL), the ulnar collateral ligament (UCL) and the sheath of the extensor carpi ulnaris (ECU).[1]
Triangular Fibrocartilage Disc Proper
Being its main component, the horizontal triangular fibrocartilage disc proper is a disc-shaped fibrocartilaginous structure that extends from the sigmoid notch of the radius to the ulnar styloid. It is a single band in its radial attachment, which separates into a proximal and distal lamina. It is called the triangular ligament. The ligamentum subcruentum is a fibrovascular structure that separates these two laminae. While the proximal lamina attaches to the styloid fovea, the distal lamina connects to the ulna styloid at its distal portion.[2]
The triangular fibrocartilage disc proper has a biconcave shape, thinner in its center, and while it does not show fenestrations in the early decades of life, these will appear later.[3]
Radioulnar ligaments
Two thick ligamentous structures border the triangular fibrocartilage disc proper in its dorsal and volar aspect. These are the dorsal and volar radioulnar ligaments (RUL).[1] While they attach directly to the radius bone, the triangular fibrocartilage disc proper attaches into hyaline cartilage.[4] This hyaline attachment is weaker than the opposite bony attachment to the ulna.
Reinforcement of the radioulnar ligaments is by fibers attaching to the lunate; the ulnolunate ligament, triquetrum, ulnotriquetral ligament, and the hamate and base of the fifth metacarpal as the ulnar collateral ligament. The ulnar collateral ligament is superficial to the meniscal homolog and of limited importance.[2]
Meniscal Homologue
As opposed to the triangular fibrocartilage disc proper, it is primally constituted of fibrous tissue. It spans from the tip and lateral side of the ulnar styloid to the ulnar aspect of the triquetrum and base of the five metacarpal.[5] It becomes almost indistinguishable from the lateral ulnar collateral ligament and dorsal extensor carpi ulnaris tendon. It creates a smooth arc that fills the distal ulnocarpal gap creating a small synovial space between itself and the triangular fibrocartilage disc proper, the pre-styloid recess.[2]
Extensor Carpi Ulnaris Tendon
The extensor carpi ulnaris tendon sheath runs in an ulnar groove and appears to be an essential stabilizer of the ulnar side of the TFCC.[3] There are suggestions that the TFCC is a vital pulley component to the extensor carpi ulnaris and that TFCC injury can lead to abnormal loading.[6]
Function
TFCC serves three crucial roles. Most importantly, it stabilizes the distal radius ulnar joint. It also cushions the ulnar carpus, being responsible for 20% of axial wrist load. And it acts as a stabilizer of the ulnar carpus.[1]
While there is consensus that the dorsal and volar radioulnar ligaments primarily maintain distal radius ulnar joint stability, there is conflicting evidence as to which provides stability during pronation and supination.[7][8][9] During pronation and supination, there is the movement of the radius around the ulna. While the radial portion of the TFCC maintains is rigid, the ulnar TFCC and ligaments (extensor carpi ulnaris and ulnar collateral ligament) show dynamic changes that contribute to maintaining distal radius ulnar joint stability.[3]
Embryology
TFCC is closely related to wrist and carpal development. A thick mesenchymal organization at the TFCC site begins to form at week 8. This organization is complete by week 14.[10]
Blood Supply and Lymphatics
Three branches supply the TFCC. The ulnar artery itself via small dorsal and volar radiocarpal branches and the palmar and dorsal branches of the anterior interosseous artery, a branch of the ulnar artery.[11]
Blood supply originates from the surrounding joint tissues and variably penetrates the TFCC. Although there are different degrees of vascular penetration observed, the inner portion of the triangular fibrocartilage disc proper is considered avascular. The blood supply is limited to its peripheral zone and resembles the knee meniscus vasculature pattern.[12]
Physiologic Variants
Central fenestrations in the triangular fibrocartilage disc proper may be present from the third decade of life and, unless bidirectional, are to be considered physiological. Bidirectional defects lead to communication between distal radioulnar and the radiocarpal compartment.[3]
Ulnar variance affects TFCC thickness. Ulnar variance is the relative length of the distal articular surfaces of the radius and the ulna. It can be neutral (same length), positive (ulna longer over 2 mm), or negative (ulna shorter).[13] Positive variance is inversely associated with TFCC thickness. It also correlates with Kienbock disease and ulna-lunate impaction syndrome.[14]
Surgical Considerations
While non-operative management is to be considered initially in stable injuries, surgical intervention should be a consideration in cases of instability and persistent pain of the distal radial-ulnar joint. Reports indicate positive outcomes in most patients following surgical management.[15]
Clinical Significance
The TFCC undergoes progressive degenerative changes from the third decade of life. These changes more frequently occur in the ulnar portion of the triangular fibrocartilage disc proper. These are due to reduced cellularity, loss of elastic fibers, and erosion, which culminate in degeneration and fenestrations of the central part of the disc.[16]
TFCC injuries can occur in three areas. In the horizontal section, it is at the periphery or its attachments, which can result from trauma or degenerative changes. Trauma is usually associated with a fall on a pronated outstretched forearm, axial load, or distracting injury to the ulnar part of the forearm. Repeated axial loading seems to be associated with degenerative injuries. A classification has been described by Palmer et all. It distinguishes between traumatic (Class 1) and degenerative injuries (Class 2).[1] However, injuries to the TFCC are often complex and involve a pattern not described in the Palmer classification.
Clinically the ‘ulnar fovea sign’ is a useful bedside test for disruption of the DRL and ulnotriquetral ligament injuries. With a sensitivity of 95.2% and specificity of 86.5% in a study of 272 patients.[17]
Imaging of TFCC is best performed with MRI in a neutral forearm position with axial, coronal, and sagittal views. MRI arthrogram appears to be a superior method to identify TFCC injuries.[18] However, the additional steps to perform an arthrogram do not seem to justify an only slightly superior imaging technique.[19]
Although distal radius fractures are not predictive of TFCC injury, an ulnar styloid fracture is predictive of a TFCC injury.[20][21]
Given the lack of blood supply, lesions to its central portion are unlikely to heal. On the other hand, injuries to its vascularized peripheral area may be amenable to surgical repair, as there is a higher chance of healing.[12]
Media
(Click Image to Enlarge)
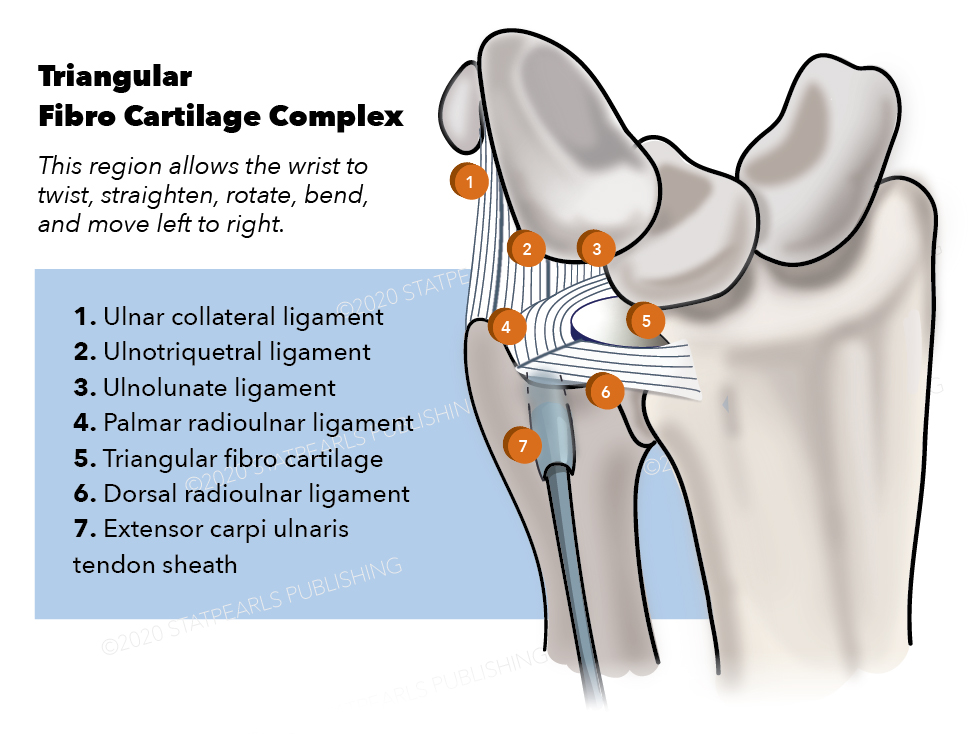
Triangular Fibro Cartilage Complex Contributed by Katherine Humphreys
References
Palmer AK. Triangular fibrocartilage complex lesions: a classification. The Journal of hand surgery. 1989 Jul:14(4):594-606 [PubMed PMID: 2666492]
Skalski MR, White EA, Patel DB, Schein AJ, RiveraMelo H, Matcuk GR Jr. The Traumatized TFCC: An Illustrated Review of the Anatomy and Injury Patterns of the Triangular Fibrocartilage Complex. Current problems in diagnostic radiology. 2016 Jan-Feb:45(1):39-50. doi: 10.1067/j.cpradiol.2015.05.004. Epub 2015 May 28 [PubMed PMID: 26117527]
Nöbauer-Huhmann IM, Pretterklieber M, Erhart J, Bär P, Szomolanyi P, Kronnerwetter C, Lang S, Friedrich KM, Trattnig S. Anatomy and variants of the triangular fibrocartilage complex and its MR appearance at 3 and 7T. Seminars in musculoskeletal radiology. 2012 Apr:16(2):93-103. doi: 10.1055/s-0032-1311761. Epub 2012 May 30 [PubMed PMID: 22648425]
Nakamura T, Takayama S, Horiuchi Y, Yabe Y. Origins and insertions of the triangular fibrocartilage complex: a histological study. Journal of hand surgery (Edinburgh, Scotland). 2001 Oct:26(5):446-54 [PubMed PMID: 11560427]
Nishikawa S, Toh S. Anatomical study of the carpal attachment of the triangular fibrocartilage complex. The Journal of bone and joint surgery. British volume. 2002 Sep:84(7):1062-5 [PubMed PMID: 12358373]
Tang JB, Ryu J, Kish V. The triangular fibrocartilage complex: an important component of the pulley for the ulnar wrist extensor. The Journal of hand surgery. 1998 Nov:23(6):986-91 [PubMed PMID: 9848547]
Linscheid RL. Biomechanics of the distal radioulnar joint. Clinical orthopaedics and related research. 1992 Feb:(275):46-55 [PubMed PMID: 1735232]
af Ekenstam F, Hagert CG. Anatomical studies on the geometry and stability of the distal radio ulnar joint. Scandinavian journal of plastic and reconstructive surgery. 1985:19(1):17-25 [PubMed PMID: 4023639]
Schuind F, An KN, Berglund L, Rey R, Cooney WP 3rd, Linscheid RL, Chao EY. The distal radioulnar ligaments: a biomechanical study. The Journal of hand surgery. 1991 Nov:16(6):1106-14 [PubMed PMID: 1748757]
Hita-Contreras F, Martínez-Amat A, Ortiz R, Caba O, Alvarez P, Prados JC, Lomas-Vega R, Aránega A, Sánchez-Montesinos I, Mérida-Velasco JA. Development and morphogenesis of human wrist joint during embryonic and early fetal period. Journal of anatomy. 2012 Jun:220(6):580-90. doi: 10.1111/j.1469-7580.2012.01496.x. Epub 2012 Mar 19 [PubMed PMID: 22428933]
Thiru RG, Ferlic DC, Clayton ML, McClure DC. Arterial anatomy of the triangular fibrocartilage of the wrist and its surgical significance. The Journal of hand surgery. 1986 Mar:11(2):258-63 [PubMed PMID: 3958460]
Bednar MS, Arnoczky SP, Weiland AJ. The microvasculature of the triangular fibrocartilage complex: its clinical significance. The Journal of hand surgery. 1991 Nov:16(6):1101-5 [PubMed PMID: 1748756]
Cerezal L, del Piñal F, Abascal F, García-Valtuille R, Pereda T, Canga A. Imaging findings in ulnar-sided wrist impaction syndromes. Radiographics : a review publication of the Radiological Society of North America, Inc. 2002 Jan-Feb:22(1):105-21 [PubMed PMID: 11796902]
Palmer AK, Glisson RR, Werner FW. Relationship between ulnar variance and triangular fibrocartilage complex thickness. The Journal of hand surgery. 1984 Sep:9(5):681-2 [PubMed PMID: 6491211]
Dunn JC, Polmear MM, Nesti LJ. Surgical Repair of Acute TFCC Injury. Hand (New York, N.Y.). 2020 Sep:15(5):674-678. doi: 10.1177/1558944719828007. Epub 2019 Feb 14 [PubMed PMID: 30762446]
Mikić ZD. Age changes in the triangular fibrocartilage of the wrist joint. Journal of anatomy. 1978 Jun:126(Pt 2):367-84 [PubMed PMID: 670069]
Tay SC, Tomita K, Berger RA. The "ulnar fovea sign" for defining ulnar wrist pain: an analysis of sensitivity and specificity. The Journal of hand surgery. 2007 Apr:32(4):438-44 [PubMed PMID: 17398352]
Magee T. Comparison of 3-T MRI and arthroscopy of intrinsic wrist ligament and TFCC tears. AJR. American journal of roentgenology. 2009 Jan:192(1):80-5. doi: 10.2214/AJR.08.1089. Epub [PubMed PMID: 19098183]
Boer BC, Vestering M, van Raak SM, van Kooten EO, Huis In 't Veld R, Vochteloo AJH. MR arthrography is slightly more accurate than conventional MRI in detecting TFCC lesions of the wrist. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2018 Dec:28(8):1549-1553. doi: 10.1007/s00590-018-2215-x. Epub 2018 Apr 26 [PubMed PMID: 29700613]
Kasapinova K, Kamiloski V. The correlation of initial radiographic characteristics of distal radius fractures and injuries of the triangular fibrocartilage complex. The Journal of hand surgery, European volume. 2016 Jun:41(5):516-20. doi: 10.1177/1753193415624669. Epub 2016 Jan 12 [PubMed PMID: 26763270]
Roulet S, Ardouin L, Bellemère P, Leroy M. Scapholunate, lunotriquetral and TFCC ligament injuries associated with intraarticular distal radius fractures: Arthroscopic assessment and correlation with fracture types. Hand surgery & rehabilitation. 2020 Apr:39(2):102-106. doi: 10.1016/j.hansur.2019.11.009. Epub 2019 Dec 23 [PubMed PMID: 31874275]