 Anatomy, Shoulder and Upper Limb, Hand Ulnar Bursa
Anatomy, Shoulder and Upper Limb, Hand Ulnar Bursa
Introduction
Bursae are sac-like structures lined with synovial fluid. They are found in friction-prone locations in the musculoskeletal system, such as bony prominences and areas surrounding tendons and ligaments. They ensure smooth movement by creating a physiologic cushion between adjacent tissues and structures.[1] The term bursae is Latin for "moneybags."
The synovial tendon sheath is a bursa that surrounds tendons as they pass through anatomic spaces. The ulnar bursa is the synovial tendon sheath enclosing the tendons of the medial 4 fingers' flexors as they pass through the carpal tunnel (see Image. Hand Bursae). It possesses 3 distinct invaginations that surround the structures of the carpal tunnel [2]:
- Deep layer: between the carpal bones and the flexor digitorum profundus tendons
- Intermediate layer: between the flexor digitorum profundus tendons and flexor digitorum superficialis tendons
- Superficial layer: superficial to the flexor digitorum superficialis tendons
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Like other bursae, the ulnar bursa typically remains collapsed but is held apart by a thin layer of synovial fluid. The ulnar reduces friction between the flexor digitorum profundus and flexor digitorum superficialis tendons as they pass deep to the flexor retinaculum and median nerve in the carpal tunnel. They insert on the hand metacarpals.
The ulnar bursa has 3 communicating invaginations at the carpal tunnel. The most superficial is located between the transverse carpal ligament and the flexor digitorum superficialis tendons. The middle and deep invaginations are situated superficial and deep to the flexor digitorum profundus tendons, respectively. The ulnar bursa encases the flexor digitorum profundus tendons of the 2nd to 4th metacarpals until the midpalmar region only. In the 5th digit, it continues distally to the phalanges and often communicates with the 5th digit's flexor tendon sheath.[3]
Embryology
Early wrist joint development has been the subject of intensive study, but there is no clear consensus about its origin and that of the ulnar bursa. However, evidence shows that the wrist joint's synovial membranes develop from the intermediate layer interzonal mesenchyme around the 13th week of gestation.[4]
Blood Supply and Lymphatics
Small branches of both the radial and ulnar arteries supply the ulnar bursa's segment overlying the carpal region. The superficial and deep palmar branches supply the ulnar bursa's more distal parts.[5] Regardless of their proximity to arteries, bursae are structurally not well-vascularized.[1]
Hand and forearm lymphatic vessels ascend near the basilic and cephalic veins before draining to the cubital lymph nodes at the medial humeral epicondyle. Superficial lymphatic vessels near the cephalic vein drain into the apical axillary and deltopectoral lymph nodes. Deep lymphatic vessels accompany deep veins and drain into the humeral axillary lymph nodes, which drain into the subclavian lymphatic trunk.[6]
Nerves
The ulnar nerve innervates the ulnar bursa.
Muscles
The ulnar bursa encases the flexor digitorum profundus and the flexor digitorum superficialis tendons near the carpal tunnel level.
Physiologic Variants
The ulnar bursa typically originates at the pronator quadratus level and continues distally, terminating 1 to 3 cm proximal to the flexor tendon sheaths of digits 2-4. However, studies reveal that the ulnar bursa may communicate with the flexor tendon sheaths of digits 2, 3, and 4, with prevalence rates of 5.1%, 4%, and 3.5%, respectively.[7] Communication with the 5th digit's flexor tendon sheath is much more common, occurring in 50% to 80% of cases.[3]
Radial and ulnar bursa communication has also been reported, and the prevalence rate can reach up to 50%. The radial bursa encases the flexor pollicis longus tendon. An intermediate bursa can bridge it with the ulnar bursa at a site posterior to the 2nd digit's deep flexor tendon or between the 2nd digit's superficial and deep flexor tendons.[8]
Surgical Considerations
Due to its location, the ulnar bursa is frequently encountered during carpal tunnel release operations. Carpal tunnel releases are the most common hand and wrist surgeries in the United States, with more than 400,000 procedures performed annually.[9]
The ulnar bursa's parietal surface adheres to the flexor retinaculum, so the synovial sheath is often incised during flexor retinaculum incision. A study found that ulnar bursa incision during flexor retinaculum release does not significantly diminish grip strength. On the other hand, ulnar bursa preservation made median nerve visualization more difficult during the operation.[10]
The ulnar bursa is vulnerable to the spread of infection from communicating flexor tendon sheaths. Management is by prompt irrigation and debridement and intravenous antibiotic administration.[11]
Clinical Significance
Carpal tunnel syndrome is a common disorder caused by median nerve irritation [12]. The pathophysiology is often idiopathic, though many cases are thought to originate from fibrous hypertrophy or ulnar bursa expansion adjacent to the nerve.[13] Fibrous hypertrophy is often secondary to repetitive wrist flexion. Meanwhile, conditions that increase synovial fluid volume, such as pregnancy, hypothyroidism, and congestive heart failure, cause median nerve compression by enlarging the ulnar bursa.[14]
Bursitis, or painful bursa swelling from noxious stimuli, occurs commonly in areas with bony protuberances like the subacromial and trochanteric bursae. Occasionally, it can affect the ulnar bursa.[1]
Septic ulnar bursitis often results from the spread of pyogenic flexor tenosynovitis, which originates from the digital flexor tendon sheaths communicating with the ulnar bursa. The 5th digit is most frequently involved, though any anomalous connections may also cause this condition.[14] Septic bursitis complicating invasive hand and wrist procedures is mainly associated with Staphylococcus aureus infection.[1]
Other Issues
Hand and Wrist Infections
The hand and wrist are two of the most commonly injured body structures. Hand injuries should be taken seriously because even seemingly trivial lesions can easily become infected, especially in the immunocompromised.
Bacteria may be introduced into the hand by animal or human bites and contaminated water. The infection can spread over multiple compartments, leading to potentially fatal necrotizing injuries.[15]
A paronychia or felon can spread infection to the distal interphalangeal joint. Inflammatory swelling in the area can compromise circulation and diminish the body's ability to fight the infection. Uncontrolled infection can then spread from the distal interphalangeal joint to the tendon sheaths and deep palmar spaces.[15]
Infections like necrotizing fasciitis can spread easily from the skin to the subcutaneous tissues and fascial planes. Cellulitis may lead to painful necrosis of the skin.[15]
Deep Hand Infections
Deep hand infections typically affect the flexor tendon sheaths.[16] These conditions usually arise from open deep hand space drainage procedures that make uncovered structures vulnerable to infection spread nearby.
The deep fascial spaces include the following:
- Dorsal subaponeurotic space
- Interdigital spaces
- Deep retroflexor space of Parona
- Thenar space
- Hypothenar space
Long flexor tendon tenosynovitis of the hand often accompanies ulnar bursa synovitis. Infections affecting the retroflexor space of Parona may lead to carpal tunnel syndrome. Common causes of ulnar bursitis are rheumatoid arthritis, suppurative infections, and pigmented villonodular synovitis.[17]
Rheumatoid arthritis (RA) is a systemic inflammatory disease that causes joint destruction and bone damage. Magnetic resonance imaging (MRI) and ultrasound (US) analysis can help in the early detection of this condition.[17]
Tuberculosis may also cause infection-related ulnar bursa synovitis and tenosynovitis, which are common in third-world countries. Rice bodies are common findings. Antitubercular therapy is an important part of the management.[17][18][19]
Pigmented villonodular synovitis is a benign giant cell tumor affecting the synovial sheaths. The most commonly involved sites are the intercarpal, radiocarpal, radioulnar, and carpometacarpal joints and the carpal and ulnar tunnels.[17]
Deep space infections must be treated immediately with drainage, wound debridement, and intravenous antibiotic administration. Endovascular synovectomy of the digital flexor tendon sheaths is a therapeutic approach that produces minimal tissue damage and scarring. However, it is contraindicated in pigmented villanodular synovitis.
During ulnar bursa endoscopic tenosynovectomy, a 3-4 mm skin incision is made at the ulnar palmar portal through the palmar aponeurosis. The ulnar palmar portal is the viewing portal. The trocar cannula is placed across the metacarpal necks, passing to the first webspace. The thumb is then abducted. An incision is made to create the first web portal at the tip of the trocar. Synovectomy is performed along the long flexor tendons between the thumb and index fingers.[17]
Deep hand infections may also spread to the overlying skin. Cellulitis can arise in the dorsal hand surface where the skin is loosely attached. The bacteria commonly involved in hand infections are gram-positive cocci, particularly Staphylococcus aureus and Streptococcus B-hemolytic A (Pyogenes). Mixed organisms are implicated in others. Gram-negative bacterial infection of the hand is associated with poor immunity.
Compression of the Ulnar Nerve in the Guyon Canal: Ulnar Tunnel Syndrome
Ulnar nerve compression in the Guyon canal can produce ulnar tunnel syndrome. Most cases are idiopathic. Less common causes are ganglion cysts, work-related activities, aneurysms, and arterial thrombosis. The condition can lead to loss of ulnar nerve motor function. Management may be conservative or surgical, depending on the cause, symptom severity, and other factors.[20]
Media
(Click Image to Enlarge)
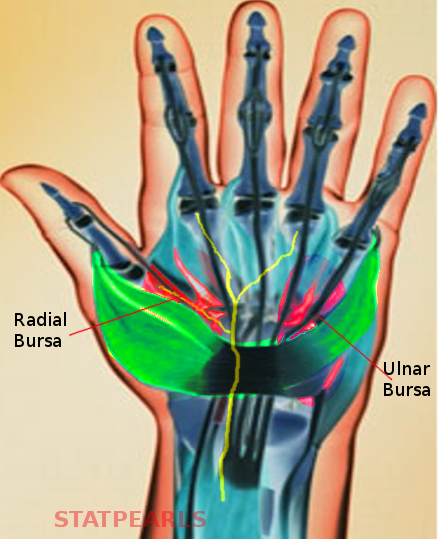
Hand Bursae. Shown in this illustration are the radial bursa and ulnar bursa.
Contributed by S Bhimji, MD
References
Williams CH, Jamal Z, Sternard BT. Bursitis. StatPearls. 2023 Jan:(): [PubMed PMID: 30020712]
Fussey JM, Chin KF, Gogi N, Gella S, Deshmukh SC. An anatomic study of flexor tendon sheaths: a cadaveric study. The Journal of hand surgery, European volume. 2009 Dec:34(6):762-5. doi: 10.1177/1753193409344529. Epub 2009 Oct 12 [PubMed PMID: 19822633]
Aguiar RO, Gasparetto EL, Escuissato DL, Marchiori E, Trudell DJ, Haghighi P, Resnick D. Radial and ulnar bursae of the wrist: cadaveric investigation of regional anatomy with ultrasonographic-guided tenography and MR imaging. Skeletal radiology. 2006 Nov:35(11):828-32 [PubMed PMID: 16688447]
Hita-Contreras F, Martínez-Amat A, Ortiz R, Caba O, Alvarez P, Prados JC, Lomas-Vega R, Aránega A, Sánchez-Montesinos I, Mérida-Velasco JA. Development and morphogenesis of human wrist joint during embryonic and early fetal period. Journal of anatomy. 2012 Jun:220(6):580-90. doi: 10.1111/j.1469-7580.2012.01496.x. Epub 2012 Mar 19 [PubMed PMID: 22428933]
de la Garza O, Lierse W, de los Angeles-García M, Elizondo R, Guzmán S. The arterial blood supply for the synovial tendon sheaths of the hand. Revista de investigacion clinica; organo del Hospital de Enfermedades de la Nutricion. 2008 Jan-Feb:60(1):31-6 [PubMed PMID: 18589585]
Lung BE, Siwiec RM. Anatomy, Shoulder and Upper Limb, Forearm Flexor Carpi Ulnaris Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30252307]
SCHELDRUP EW. Tendon sheath patterns in the hand; an anatomical study based on 367 hand dissections. Surgery, gynecology & obstetrics. 1951 Jul:93(1):16-22 [PubMed PMID: 14855245]
Resnick D. Roentgenographic anatomy of the tendon sheaths of the hand and wrist: tenography. The American journal of roentgenology, radium therapy, and nuclear medicine. 1975 May:124(1):44-51 [PubMed PMID: 1147163]
Fnais N, Gomes T, Mahoney J, Alissa S, Mamdani M. Temporal trend of carpal tunnel release surgery: a population-based time series analysis. PloS one. 2014:9(5):e97499. doi: 10.1371/journal.pone.0097499. Epub 2014 May 14 [PubMed PMID: 24828486]
Forward DP, Singh AK, Lawrence TM, Sithole JS, Davis TR, Oni JA. Preservation of the ulnar bursa within the carpal tunnel: does it improve the outcome of carpal tunnel surgery? A randomized, controlled trial. The Journal of bone and joint surgery. American volume. 2006 Nov:88(11):2432-8 [PubMed PMID: 17079401]
Level 1 (high-level) evidencePatel DB, Emmanuel NB, Stevanovic MV, Matcuk GR Jr, Gottsegen CJ, Forrester DM, White EA. Hand infections: anatomy, types and spread of infection, imaging findings, and treatment options. Radiographics : a review publication of the Radiological Society of North America, Inc. 2014 Nov-Dec:34(7):1968-86. doi: 10.1148/rg.347130101. Epub [PubMed PMID: 25384296]
Sevy JO, Varacallo M. Carpal Tunnel Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 28846321]
Tang A, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Carpal Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 30571003]
Aboonq MS. Pathophysiology of carpal tunnel syndrome. Neurosciences (Riyadh, Saudi Arabia). 2015 Jan:20(1):4-9 [PubMed PMID: 25630774]
Malizos KN, Papadopoulou ZK, Ziogkou AN, Rigopoulos N, Athanaselis ED, Varitimidis SE, Dailiana ZC. Infections of Deep Hand and Wrist Compartments. Microorganisms. 2020 Jun 3:8(6):. doi: 10.3390/microorganisms8060838. Epub 2020 Jun 3 [PubMed PMID: 32503146]
Lui TH, Lee CH. Little Finger Flexor Tendoscopy, Endoscopy of the Ulnar Bursa and Midpalmar Space. Arthroscopy techniques. 2018 Aug:7(8):e817-e822. doi: 10.1016/j.eats.2018.04.002. Epub 2018 Jul 9 [PubMed PMID: 30167359]
Lui TH, Lee JCY. Endoscopic Synovectomy of the Ulnar Bursa of the Palm of the Hand. Arthroscopy techniques. 2018 Dec:7(12):e1257-e1261. doi: 10.1016/j.eats.2018.08.012. Epub 2018 Nov 5 [PubMed PMID: 30591871]
Al Lahham S, Aljassem G, Asnaf A, Omari RY, Alyazji Z, Sada R. A Rare Presentation of Hand TB Extending to the Space of Parona. Plastic and reconstructive surgery. Global open. 2022 Mar:10(3):e4156. doi: 10.1097/GOX.0000000000004156. Epub 2022 Mar 17 [PubMed PMID: 35317454]
Lee CH, Tandon A. Focal hand lesions: review and radiological approach. Insights into imaging. 2014 Jun:5(3):301-19. doi: 10.1007/s13244-014-0334-4. Epub 2014 May 17 [PubMed PMID: 24838840]
Hammarstedt JE, Duethman NC, Dennison DG. Pigmented Villonodular Synovitis as an Atypical Cause of Deep Motor Branch Neuropathy. Journal of orthopaedic case reports. 2021 Apr:11(4):80-84. doi: 10.13107/jocr.2021.v11.i04.2162. Epub [PubMed PMID: 34327172]
Level 3 (low-level) evidence