Introduction
Osteoporotic compression fractures are the most common fragility fractures seen today. Osteoporotic individuals may suffer a vertebral compression fracture as a result of seemingly insignificant trauma, for example, sitting down abruptly. In younger individuals, a higher-energy, axial loading force would be needed to compress the cancellous bone of the vertebral body. Non-osteoporotic lumbar compression fractures are typically seen in car accidents and fall or jump from a height. Infectious and malignant processes that weaken vertebrae can also lead to an eventual compression fracture.[1]
These can cause significant physical limitations, including back pain, and functional disability.[2] Compression fractures are prone to progression over time and may facilitate the compression of adjacent vertebrae due to compensatory increases in axial load. Due to the high prevalence of this injury, there is a large socioeconomic burden associated with the disease and there has been significant controversy regarding optimal treatment. Vertebroplasty (VP) and kyphoplasty (KP) are two percutaneous interventional procedures used to treat symptomatic, nonhealing fragility fractures of the spine by injecting polymethyl methacrylate (PMMA) into the vertebral body thereby providing structural support. These procedures have come under controversy due to the lack of significant improvement in randomized control trials. In a randomized, double-blinded, placebo-controlled trial in patients with painful osteoporotic compression fractures were randomized to undergo vertebroplasty or a sham procedure. They found no beneficial effects of vertebroplasty compared to the sham procedure.[3] Also, the VP has an increased rate of PMMA extravasation compared to KP. Therefore, VP has been replaced with KP as the main surgical procedure addressing osteoporotic compression fractures.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Bone mineral density tends to decrease with age following peak bone mass, leading to osteoporotic bone. Osteoporotic bone is of normal quality but decreased in quantity. The cancellous bone has decreased trabecular quantity and thin cortical bone, leading to a decreased load to failure capacity and more prone to fracture. Vertebral compression fractures (VCFs) are the result of axial force overcoming bony integrity. VCFs are defined as a loss of about 20% or at least 4 mm of anterior, middle, or posterior vertebral height.[4] The thoracolumbar spine (T12-L2) is the most frequently affected site (60-75%), followed by the lower lumbar region (L2-L5).[2]
Compression fractures characteristically involve the anterior column of the spine which is comprised of the anterior two-thirds of the vertebral body, the anterior two-thirds of the intervertebral disc, and the anterior longitudinal ligament. Unlike vertebral burst or Chance fractures, a compression fracture does not compromise the posterior tension band.[5] The posterior tension band is characterized by muscles, ligaments, processes, and pedicles that maintain spinal stability.[5] Therefore, compression fractures are deemed stable fractures.
Posterior tension band components include:
- Posterior ligamentous complex: Supraspinous and interspinous ligaments, ligamentum flavum
- Musculature: Longissimus, iliocostalis, spinalis, semispinalis, rotatores, intertransversarii, multifidus
- Bone: Transverse and spinous processes, pedicles, facets
Indications
The standard treatment options for vertebral compression fracture consist of conservative therapies involving analgesics, external orthosis, physical therapy, and bed rest. The majority of patients can be treated with observation and a gradual return to activity. Symptoms typically resolved within 4-6 weeks. Surgical intervention is indicated for certain patients who suffer from significant pain and morbidity after this time period.[1]
In recently published AAOS (American Academy of Orthopedic Surgeon) guidelines for osteoporotic compression fractures, they recommend strongly against the use of vertebroplasty.[6] However, kyphoplasty remains a viable option for the treatment of these injuries.
Contraindications
An absolute contraindication to vertebroplasty and kyphoplasty is an asymptomatic compression fracture. Often found incidentally on chest x-rays, healed compression fractures will not benefit from intervention. The procedure should not be performed if there are ongoing local or systemic infectious processes such as osteomyelitis or discitis. Relative contraindications include fracture extension into the posterior vertebral body wall that can risk cement extravasation into the spinal canal, and severe compression fractures/deformity.[1]
Equipment
VP/KP is best performed using high-quality fluoroscopy to confirm the needle placement. This is best accomplished with the use of C-arm fluoroscopy. This procedure can be performed with one C-arm transitioning between anteroposterior AP and lateral images, or with two C-arms, one positioned for AP, and the other for lateral images. The two C-arm technique alleviates the need to constantly change the C-arm position. A list of types of equipment is given below[1]:
- Fluoroscopy
- Spinal needle
- Spinal needle stylets, with diamond-shaped multi-bevel and single-bevel
- Polymethacrylate (PMMA) cement
- +/- Kyphoplasty balloon catheter (See Technique for details)
Personnel
Vertebroplasty and kyphoplasty are performed primarily by interventional radiologists, interventional pain management physicians, and neurosurgical/orthopedic spine specialists. Intraoperative personnel may also include a fluoroscopy technician, nurse, and a company representative. If general sedation is implemented, an anesthesiologist is also present.
Preparation
Vertebroplasty and kyphoplasty are considered a procedure with moderate bleeding risk (Category 2) according to the Society of Interventional Radiology (SIR) Standards of Practice Consensus Guidelines. INR and complete blood count (CBC) should be attained pre-procedure. Recommendations are as follows:
- INR corrected to less than 1.5
- Transfuse for platelets less than 50,000
- ASA: No need to hold
- Clopidogrel: Hold 5 days pre-procedure
- Low molecular weight heparin (LMWH): Hold one dose pre-procedure
Antibiotic prophylaxis is achieved with the administration of 1 gram of intravenous (IV) cefazolin, 1 hour pre-procedure (first-line). Once the patient is intubated, the patient is then placed in the prone position on a well-padded radiolucent table. Proper positioning of the fluoroscopic C-arm is crucial. The affected vertebral level is isolated and proper views are obtained before the start of the procedure and the C-arm position is noted so it can be replicated after surgical preparation. On the (AP) image, you want to view the vertebral body in a direct AP position with the endplates parallel to the X-ray beam, and the spinous process centered between the pedicles.[7] The pedicles are then marked with a marking pen. The surgical area is prepped and draped in a sterile fashion using the maximum surgical barrier technique. Preprocedural prophylactic antibiotics are given before the start of the procedure.
Technique or Treatment
VP and kyphoplasty procedure setup and technique are extremely similar, the only difference being that kyphoplasty creates a cavity in the vertebral body by balloon expansion. In the thoracic and lumbar spine, VP is performed using a transpedicular or parapedicular approach.[7] Using a radiolucent instrument, the incision is marked over the pedicle under fluoroscopic guidance. A small stab incision is made over the entry point, location is confirmed by AP X-ray before an incision is made. The VP hollow needle is then inserted and under AP intermittent fluoroscopic guidance the entry point is confirmed before inserting. The starting point is usually along the superior lateral edge of the pedicle with variable angulation depending on the pedicle level being accessed.[8] The medial and inferior walls of the pedicle must be clearly visualized in order to decrease injury to nerve roots and the spinal cord.[9] A mallet can be used to gently tap the device into the starting point, being careful not to cross the medial pedicle wall. If the trajectory is appropriated on the AP view, the C-arm is then transitioned to the lateral view to confirm proper pedicle placement and superior/inferior trajectory in the vertebral body. If the trajectory is appropriate, the C-arm is transitioned back to the AP view, and the VP device further advanced, being careful not to cross the medial pedicle wall. This is continued until the VP device has passed through the pedicle and is in the posterior vertebral body, which is confirmed on the lateral image. Once the posterior vertebral body has been accessed you can now advance the VP device more medial and distal with. The tip of the needle should be placed in the anterior to the middle third of the vertebral body as close to the midline as possible.[1] The final needle position should be confirmed by fluoroscopy before bone cement injection. If performing kyphoplasty, at this point the balloon catheter is then inserted and inflated using visual volume and pressure controls to create a cavity. Inflation is stopped when the pressure above 200-250 psi is obtained when the balloon contacts the cortical surface or expands beyond the border of the vertebral body, or if the height of the vertebrae is restored. The balloon is then deflated and removed. Once the cement is mixed, it is not injected until it reaches the consistency of a paste, this is done in order to prevent leakage in severely osteoporotic bone.[10] The goal is to deliver the cement at a controlled pace, and evenly in the vertebral body while avoiding extra-vertebral extravasation. Multiple AP and lateral images are utilized to confirm cement injection into the vertebral body and to confirm there is no extra-vertebral extravasation, this will appear as a radiopaque substance that is distinctly differentiated from surrounding bone. As cement is injected, the needle is slowly pulled back to allow for even distribution throughout the vertebral body. Cement injection is discontinued once it has reached the posterior vertebral body. When removing the needle, in order to avoid a cement tail, a stylet is used to clear the needle of residual cement.
Complications
Complications occur in about 50% of the patients who undergo vertebroplasty, but about 95% of them are clinically asymptomatic.[11] A list of common complications is listed below.
- Infection and bleeding: Universally recognized risks of any interventional procedure.
- Radiculopathy or neurological deficit: If the spinal needle violates the inferior or medial wall of the pedicle during entry, there is a significant risk of damage to a nerve root or the spinal cord.
- The most common complication associated with vertebroplasty is PMMA leakage into the surrounding tissue, intradiscal, and spinal canal. This is more common for VP because no cavity is created as in kyphoplasty and increased pressure is needed to inject the PMMA.[12]
- Pulmonary embolization: Cement particles introduced into a vein have the potential to embolize to the lungs, however, this is a rare complication
- Spinal stenosis: Cement leakage into the epidural space can essentially cause iatrogenic spinal stenosis, however, this is a rare complication.
Clinical Significance
Acute compression fractures are often painful, immobilizing conditions of elderly individuals. Studies have demonstrated significant pain relief, improved quality of life, decreased dependence on narcotics, and increased mobility in patients who undergo such interventions. In summation, vertebroplasty and kyphoplasty have proven to be an effective treatment modality in patients with painful, acute compression fractures refractory to medical management. A risk/benefit analysis should always be completed before intervening, and an understanding of SIR consensus guidelines assures a higher standard of care.
Enhancing Healthcare Team Outcomes
Only patients with acute compression fractures should be considered for vertebroplasty and kyphoplasty. It is the responsibility of the primary care physician and interventionalist to verify the acuity of the fracture using diagnostic imaging. Careful consideration of bleeding risk helps prevent potentially life-threatening spinal hematoma or hemorrhage. Careful post-procedure, clinician and nursing follow up are recommended to ensure that the desired analgesic effect has been achieved. Interventionalists, rehabilitation specialists, and physical therapists all play an integral role in helping patients return to their daily activities and previous quality of life. Nursing must evaluate for postoperative infection and other complications.
Media
(Click Image to Enlarge)
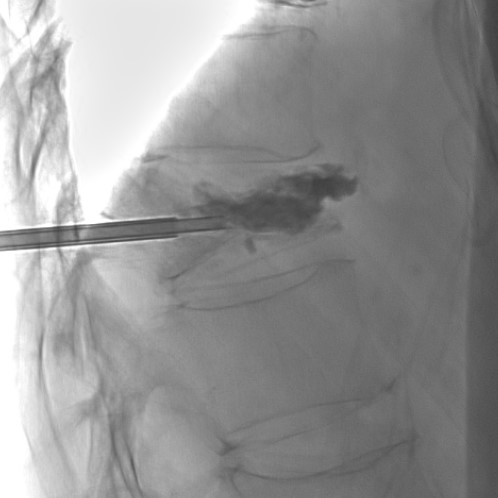
fluoroscopic image, cement injection during percutaneous kyphoplasty contributed by Mohamad Jaber, MD
References
Jay B,Ahn SH, Vertebroplasty. Seminars in interventional radiology. 2013 Sep [PubMed PMID: 24436552]
Hoyt D,Urits I,Orhurhu V,Orhurhu MS,Callan J,Powell J,Manchikanti L,Kaye AD,Kaye RJ,Viswanath O, Current Concepts in the Management of Vertebral Compression Fractures. Current pain and headache reports. 2020 Mar 20 [PubMed PMID: 32198571]
Buchbinder R,Osborne RH,Ebeling PR,Wark JD,Mitchell P,Wriedt C,Graves S,Staples MP,Murphy B, A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. The New England journal of medicine. 2009 Aug 6 [PubMed PMID: 19657121]
Level 1 (high-level) evidenceDewar C, Diagnosis and treatment of vertebral compression fractures. Radiologic technology. 2015 Jan-Feb [PubMed PMID: 25739109]
Pizones J,Zúñiga L,Sánchez-Mariscal F,Alvarez P,Gómez-Rice A,Izquierdo E, MRI study of post-traumatic incompetence of posterior ligamentous complex: importance of the supraspinous ligament. Prospective study of 74 traumatic fractures. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2012 Nov [PubMed PMID: 22722921]
Genev IK,Tobin MK,Zaidi SP,Khan SR,Amirouche FML,Mehta AI, Spinal Compression Fracture Management: A Review of Current Treatment Strategies and Possible Future Avenues. Global spine journal. 2017 Feb [PubMed PMID: 28451512]
Beall DP,Braswell JJ,Martin HD,Stapp AM,Puckett TA,Stechison MT, Technical strategies and anatomic considerations for parapedicular access to thoracic and lumbar vertebral bodies. Skeletal radiology. 2007 Jan [PubMed PMID: 17013657]
Level 2 (mid-level) evidenceStockton R,Albano J,Lentz J,Ganz M,Grewal K,Katsigiorgis G, A comparison of lumbar transverse pedicle angles between ethnic groups: a retrospective review. BMC musculoskeletal disorders. 2019 Mar 18 [PubMed PMID: 30885189]
Level 2 (mid-level) evidencePark SY,Modi HN,Suh SW,Hong JY,Noh W,Yang JH, Epidural cement leakage through pedicle violation after balloon kyphoplasty causing paraparesis in osteoporotic vertebral compression fractures - a report of two cases. Journal of orthopaedic surgery and research. 2010 Aug 6 [PubMed PMID: 20691094]
Level 3 (low-level) evidenceZhan Y,Jiang J,Liao H,Tan H,Yang K, Risk Factors for Cement Leakage After Vertebroplasty or Kyphoplasty: A Meta-Analysis of Published Evidence. World neurosurgery. 2017 May [PubMed PMID: 28192270]
Level 1 (high-level) evidenceSaracen A,Kotwica Z, Complications of percutaneous vertebroplasty: An analysis of 1100 procedures performed in 616 patients. Medicine. 2016 Jun [PubMed PMID: 27310966]
Xiao H,Yang J,Feng X,Chen P,Li Y,Huang C,Liang Y,Chen H, Comparing complications of vertebroplasty and kyphoplasty for treating osteoporotic vertebral compression fractures: a meta-analysis of the randomized and non-randomized controlled studies. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2015 Jul [PubMed PMID: 24989933]
Level 2 (mid-level) evidence