Introduction
The brain's white matter (WM) constitutes a network of nerve fibers that allows the exchange of information and communication between different areas of the gray matter (GM). WM lies beneath the GM in the brain and superficial to GM in the spinal cord and has evolved more than GM and occupies almost half of the brain.[1] The size of white matter varies depending on the extent of central GM in different regions of spinal cord cross-sections. In particular, the GM to WM ratio grows from the cervical region to the lumbar region as the WM decreases when it proceeds towards the terminal portion of the spinal cord.
The WM contains neural networks formed by bundles of axons to mediate essential connectivity between different key motor and cognitive cortical regions. The white matter comprises myelinated and unmyelinated axons and glial cells, including myelin-producing oligodendrocytes, microglia, astrocytes, and oligodendrocyte progenitor cells. Myelin acts as electrical insulation for axons, is responsible for rapid saltatory impulse propagation, and protects the nerve fibers from injury.[2] Myelin has a water content of about 40%. The remaining dry mass (60%) is mainly composed of proteins (15% to 30%) and lipids (70% to 85%), with phospholipids, cholesterol, galactolipids, and plasmalogens in a molar ratio of 2:2:1:1, respectively.[3]
WM lesions or leukoaraiosis encompasses small vessel vascular brain diseases and non-vascular conditions. Any process leading to a change in chemical composition, damage, or ischemia of myelinated fibers can present as white matter lesions on magnetic resonance imaging (MRI), representing the gold standard for lesion investigation. WM hyperintensity (WMH) is quite a descriptive expression used on MRI. These lesions are best seen as hyperintensities on T2 weighted and FLAIR (fluid-attenuated inversion recovery) sequences of MRI. FLAIR sequences are particularly important in assessing white matter lesions near the ventricular margin by nullifying the cerebrospinal fluid signal.
While the WMHs are well-described on MRI, the lesions were first illustrated based on brain computed tomography (CT). In 1985, Hachinski 1985 described "leukoaraiosis" as "diminished density of white matter that is seen on brain computed tomography."[4] Concerning small vessel vascular brain processes, white matter lesions are commonly present in MRI of asymptomatic elderly individuals, typically located in periventricular (PV-WMH) and deep subcortical regions (DS-WMH). For instance, white matter lesions are frequently detected in people with untreated chronic hypertension. The volume of white matter lesions increases with age from small punctate lesions to large confluent lesions. Nevertheless, although white matter lesions were initially considered a normal, age-related finding, recent investigations proved that large areas of disease in the brain's WM must be considered neuroimaging markers of brain frailty. Of note, various longitudinal studies described white matter lesions as a predictor for future risk of stroke, cognitive decline, depression, disability, and mortality in the general population.[5][6] The clinical significance of the lesions is confirmed by the results of a meta-analysis that demonstrated a 3-fold increased risk of dementia and stroke and a doubled risk of death in people with white matter lesions.[7] For instance, ischemic microvascular disease, a vascular cause of white matter lesions, may cause about 45% of dementia cases and 20% of strokes. Again, white matter lesions are associated with poor post-stroke outcomes and increased risk of parenchymal hematoma following mechanical thrombectomy.[8][9]
Apart from white matter lesions secondary to small vessel disease, these lesions are also common features of demyelinating inflammatory disorders, leukodystrophies, and degenerative disorders. Clinical aspects, prognosis, and management vary according to the distribution and spread of the WM damage. Therefore, this group of lesions and diseases includes very different clinical conditions regarding etiology, pathogenesis, pathological features, clinical presentations, imaging, and therapy.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of white matter lesions is heterogeneous. Based on etiology, they can be divided into vascular and non-vascular causes.
Vascular Causes of White Matter Lesions
- Microvascular ischemic disease or small vessel disease
- Atherosclerosis
- Migraine
- Amyloid angiopathy
- Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy
- Vasculitis
- Susac syndrome
Non-Vascular Causes for White Matter Lesions
- Inflammatory: Multiple sclerosis, acute disseminated encephalomyelitis, and neuromyelitis optica spectrum disorders
- Infectious: Human immunodeficiency virus encephalopathy, progressive multifocal leukoencephalopathy, neuroborreliosis, herpes simplex virus, cytomegalovirus encephalitis, neurosyphilis, central nervous system cryptococcal infection, Whipple disease, Lyme encephalopathy, subacute sclerosing panencephalitis.
- Toxic: Chronic alcohol abuse, carbon monoxide intoxication, inhalation of toluene, heroin, and cocaine, methotrexate-related leukoencephalopathy.
- Metabolic: Vitamin B12 deficiency, copper deficiency, acute intermittent porphyria, hepatic encephalopathy, Hashimoto encephalopathy.
- Neoplastic: Glial tumors, central nervous system, lymphoma
- Traumatic: Radiotherapy, post-concussion (traumatic axonal injury)
- Genetic:
- Lysosomal storage diseases: Metachromatic leukodystrophy, Krabbe disease, Fabry disease, gangliosidosis, mucopolysaccharidosis
- Peroxisomal disorders: X-linked adrenoleukodystrophy, Zellweger syndrome, Refsum disease
- Mitochondrial disorders: Myoclonic epilepsy with ragged red fibers, mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes, Leigh disease, Kearns-Sayre disease
- Aminoacidopathies and organic acidopathies: Canavan disease, glutaric aciduria, urea cycle disorders
- Unknown etiology: Alexander disease, Vander Knapp encephalopathy
- Others: Vanishing white matter disease, myotonic dystrophy
Another nosographic approach distinguishes primary white matter lesions, derived from an unknown etiology, from secondary ones; these latter are due to a great variety of known etiologies.
Epidemiology
The prevalence of age-related vascular white matter lesions in the general population is approximately 10% to 20% at 60 years and approaches 100% in those older than 90 years.[10] Studies have reported that white matter lesions are common in Japanese, Chinese, Caucasian, African-American, and Caribbean Black populations.[11] Multiple sclerosis (MS) represents the most common inflammatory neurological condition in young adults. Again, it has been estimated that MS disease affects approximately 2,500,000 people worldwide. In the US, the rate is 57 to 78 cases per 100,000 people in the southern states and 100 to 140 cases in the northern states.[12] The prevalence of neuromyelitis optica spectrum disorder (NMOSD) is approximately 1 in 100,000 in the White population and up to 10 per 100,000 in Black populations. In East Asians, the prevalence of NMOSD is about 3.5 per 100,000 population.[13]
Progressive multifocal leukoencephalopathy (PML) is present in 1% to 4% of patients with acquired immunodeficiency syndrome. PML is also a rare yet severe complication of immunosuppression, such as in organ transplant patients. Furthermore, gliomas account for up to 35% of CNS tumors in adolescents and young adults.[14] The incidence of white matter lesions secondary to heritable WM disorder or leukodystrophy is approximately 1 per 8000 live births.[15] However, for acquired WM disorders in children, it is estimated to be 1.66 per 100,000 children.[16]
Pathophysiology
Cerebrovascular risk factors such as age, hypertension, diabetes mellitus, hyperlipidemia, hyperhomocysteinemia, and hypersensitive C-reactive protein are well-known risk factors for vascular white matter lesions.[11] Genetic factors also play an essential role in developing white matter lesions, as many genetic loci have been identified, and twin studies have suggested 55% to 80% heritability.[17][18]
Pathophysiology for developing vascular white matter lesions in older patients is thought to be secondary to chronically reduced blood flow by arteriosclerosis, lipohyalinosis, or fibrinoid necrosis of small vessels. Incomplete infarction secondary to persistent hypoxia leads to altered cerebral autoregulation, promoting the transcription of many inflammatory genes, leading to the breakdown of the blood-brain barrier and entry of pro-inflammatory proteins into the brain parenchyma and vessel wall. This breakdown will lead to demyelination, axonal loss, vacuolation, and reduced glial density. Results from some studies also suggest the role of venous collagen deposition in the pathogenesis of ischemic white matter lesions.[19]
The different distribution of the lesions could be linked to different pathogenetic mechanisms. Periventricular-white matter hyperintensity (PV-WMH) is featured by gliosis, loosening of the WM, and loss around convoluted venules in perivascular spaces. In contrast, the primary characteristics of deep subcortical-white matter hypersensitivity (DS-WMH) are demyelination, gliosis, and augmented tissue loss as the lesions become serious. By summarizing, the pathological characteristics of white matter lesions may encompass myelin rarefaction, reactive gliosis, axonal loss, infarction, venular collagenosis, and arteriosclerotic small vessel alterations. Moreover, blood-brain barrier impairment plays a pivotal role in the genesis of WM damage, and a different pattern involves PV-WMH and DS-WMH.[20]
In white matter lesions secondary to non-vascular diseases like MS, demyelination is caused by autoimmune inflammation-mediated primarily by T cells against myelin proteins.[21] While the cause of MS is still unknown, it probably presupposes a combination of genetic susceptibility and nongenetic factors such as viral infection and low vitamin D levels. This combination results in an autoimmune disorder that leads to myelin loss, destruction of oligodendrocytes, and reactive astrogliosis. However, the axon is usually undamaged; in some patients, it is aggressively destroyed.[22]
NMOSD is a group of inflammatory disorders of the CNS featuring severe immune-mediated demyelination and axonal damage, mainly involving optic nerves and the spinal cord. Although these disorders were studied as a variant of MS, they have distinct pathophysiology. The autoimmune pathogenesis for NMOSD involves immunoglobulin G autoantibody against the aquaporin-4 water channel [23] or the myelin oligodendrocyte glycoprotein. No antibodies are pertinent in a subset of NMOSD (double-seronegative disease).
The exact mechanism of the pathophysiology of acute disseminated encephalomyelitis is still unknown. However, it has been related to inflammation initiated by infection or vaccination in genetically susceptible individuals, causing demyelination. Progressive multifocal leukoencephalopathy is a central demyelinating disease caused by reactivation (usually occurs at CD4 count less than 200/cm) of latent JC polyomavirus (or John Cunningham virus or human polyomavirus 2) in oligodendrocytes in patients with human immunodeficiency virus. Leukodystrophy causes white matter lesions secondary to substrate accumulation due to enzymatic defects causing demyelination.
Traumatic axonal injury refers to severe axonal mechanical damage due to a rotational acceleration of the brain. Although its pathophysiology is complicated, the injury damage is firstly due to a mechanical break involving axonal microtubules. This stretch induces axonal damage through undulations, breaks, and direct membrane mechanoporation with calcium influx. This mechanism leads to the activation of several injurious pathways, including caspase-mediated proteolysis and cytokine-mediated microglia recruitment with impairment of axonal transport and the aggregation of transported proteins in varicose swellings.[24]
History and Physical
Clinical presentation can vary from asymptomatic to patients with disabling disease as per the white matter lesions etiology. Older patients with small punctate cerebral vascular white matter lesions are usually asymptomatic, but they progress to large confluent lesions and can present with subtle functional decline, cognitive impairment, dementia, urinary incontinence, gait and balance impairment, and neuropsychiatric disorders. Within the group of vascular WM diseases, the distribution of lesions varies greatly, and consequently, the clinical aspects. For instance, in small vessel disease, the WMHs are mainly found in basal ganglia and frontotemporal and periventricular WM; these may induce cognitive impairment, loss of balance or coordination, vision loss, and dizziness. Severe headaches can be present in different types of white matter lesions.
Patients with non-vascular etiology of white matter lesions like MS can have heterogeneous presentations, including fatigue, unilateral visual blurring, sensory changes, motor abnormality, urinary incontinence, speech and swallowing difficulties, pain, anxiety, depression, numbness and tingling, and cognitive dysfunction. Nevertheless, the clinical scenario and evolution of the disease vary from patient to patient. Some patients deteriorate rapidly, while in others, an alternation between relapses and remissions is observed.
Clinical aspects of NMOSD include acute attacks of bilateral optic neuritis with significant visual loss or transverse myelitis, inducing limb weakness, sensory loss, and bladder dysfunction. Other symptoms can consist of episodes of intractable nausea, vomiting, hiccups, excessive daytime somnolence or narcolepsy, and seizures. Commonly relapsing courses and variable degrees of recovery occur within weeks to months.[25]
Children with white matter lesions presenting with progressive symptoms of declining developmental milestones, cognitive impairment, and motor abnormalities should be suspected of leukodystrophy. However, patients in their first or second decade with white matter lesions secondary to acute disseminated encephalomyelitis present with acute onset and rapidly progressive symptoms of fever, headache, vomiting, confusion, or altered sensorium. Although migraine was associated with structural changes in the brain WM, these lesions are generally not linked to any neurological issues, as well as an increased risk of cognitive decline.[26]
Evaluation
Evaluating patients presenting with white matter lesions depends on the patient's age, clinical scenario, and pattern of white matter lesions on MRI, which are common manifestations of cerebral small vessel disease and are associated with vascular risk factors. These patients should be screened for vascular risk factors by routine laboratory tests, including a complete metabolic panel, lipid profile, and HbA1c. Also, it is worthwhile to quantify white matter lesions to monitor their progress with time in these patients. Various grading scales like the Fazekas scale and age-related white matter changes rating scale can be used to assess the extent and progression of white matter lesions (see Image. Fazekas Grade 3 White Matter Lesions).[27][28][29]
Patients with non-vascular white matter lesions require further evaluation to identify the etiology of the lesions. Cerebral spinal fluid analysis is helpful in cases of suspected MS (oligoclonal bands), Acute disseminated encephalomyelitis (ADEM; lymphocytic pleocytosis with raised proteins), and infectious demyelination (antiviral antibodies). MR spectroscopy can help in the etiological diagnosis of white matter lesions to differentiate lesions based on different metabolite peaks.
Additional tests like serology for autoantibodies in case of suspected vasculitis, anti-myelin oligodendrocyte glycoprotein antibodies in ADEM, and anti-AQP4 antibodies in NMOSD. Also, metabolic and toxicology screens can be helpful in suspected cases. Children with white matter lesions and clinical scenarios for leukodystrophy require genetic testing.[30]
Treatment / Management
White matter lesions in older adults most commonly reflect underlying small vessel ischemic lesions and, more probably, cognitive dysfunction. Proper management may prevent further deterioration by targeting all vascular risk factors.[31] White matter lesions detected incidentally on MRI of older patients require management of vascular risk factors by:(B3)
- Intensively controlling the blood pressure
- Strict diabetes control
- Improving dyslipidemia
- Promoting physical fitness
- Avoiding smoking
- Avoiding alcohol
- Use of antiplatelets
Prophylaxis of migraine with aura can also help decrease the risk of white matter lesions. Using B vitamins to lower homocysteine levels is useful in managing patients with small vessel disease. Managing non-vascular white matter lesions is individualized as per etiology. White matter lesions secondary to MS flares are treated with steroids. However, patients need long-term maintenance therapy with disease-modifying treatment to halt disease progression.
Furthermore, immunosuppression with high-dose intravenous glucocorticoids is used in patients with ADEM. Acyclovir has also been reported to have benefits in some cases. Leukodystrophies do not have a specific treatment; treatment is only supportive and symptomatic. Other white matter lesions caused by specific diseases, such as progressive multifocal leukoencephalopathy (PML), human immunodeficiency virus (HIV), and gliomas, must be treated for those specific causes.
Differential Diagnosis
Pattern recognition of white matter lesions in MRI is crucial as it may make the diagnosis in many conditions.[32]
The differential diagnosis for symmetric white matter lesions can include:
- Bilateral hemispheres: toxic encephalopathy, HIV encephalopathy, autoimmune encephalopathies, and vitamin B12 deficiency
- Periventricular lesions: small vessel disease, HIV encephalopathy, vitamin B12 deficiency, metachromatic leukodystrophy, X-linked adrenoleukodystrophy, and vanishing white matter disease
- Subcortical including arcuate fibers: Alexander disease, Kearns-Sayre syndrome, and cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
- Frontal predominance: Alexander disease and metachromatic leukodystrophy
- Parietal/temporal/occipital lobes: posterior reversible encephalopathy, heroin abuse, and Krabbe disease
- Corpus callosum: Marchifava-Bignami disease, metachromatic leukodystrophy, and Krabbe disease
- Cerebellum: toxic encephalopathy and mitochondriopathies
- Central pons: central pontine myelinolysis
The differential diagnosis for asymmetric white matter lesions:
- Patchy multifocal confluent lesion: MS, autoimmune encephalopathies, and CADASIL
- Parieto-occipital regions: PML
Prognosis
The prognosis of patients with white matter lesions depends on the etiology of the lesions. Patients with age-related white matter lesions are irreversible and progressive. Large and confluent white matter lesions have a poor prognosis and lead to cognitive impairment and global functional decline.[33]
White matter lesions secondary to MS have interpatient variability in prognosis. Severe disabilities are present in 5% of patients within the first 5 years of onset, and 10% to 20% of patients of MS remain unimpaired without therapy after 20 years.[34] NMO and ADEM have a variable prognosis from complete recovery to the development of permanent physical disability, especially in post-measles ADEM.[35] Acute demyelinating disease prognosis depends upon the severity of the initial illness. Patients responding to treatment have a favorable prognosis. However, leukodystrophies have a poor prognosis. Reversible causes, including metabolic and toxic encephalopathies, have a good prognosis.
Complications
Severe white matter lesions are associated with cognitive impairment, global functional decline, cerebrovascular accident, mood disorders, gait, and balance dysfunction. White matter lesions are also associated with grey matter atrophy and accelerated neurodegeneration.[36] Furthermore, severe, extensive involvement of white matter by non-vascular causes like MS, ADEM, and NMO causes disability.
Deterrence and Patient Education
Patients with vascular risk factors should be identified early and counseled on lifestyle changes and control of comorbid conditions. Self-monitoring of blood pressure and blood sugar, dietary modifications, weight reduction, and improving physical fitness have proven to decrease the progression of white matter lesions.[37] Involvement in cognitively complex leisure activity to improve cognitive reserve has been associated with a protective effect on cognitive functioning and late-life depression in patients with white matter lesions.[38]
Enhancing Healthcare Team Outcomes
As described, white matter lesions have varied clinical presentations, differential diagnoses, and complications. Managing these conditions require extensive collaboration and coordination among a team of professionals, which consists of neurologists, radiologists, internists, ophthalmologists, psychiatrists, neurosurgeons, rheumatologists, microbiologists, pain specialists, nurse specialists, mental health nurses, pharmacists, physical therapists, and nutritionists. Clear and effective communication between these professionals while monitoring the progression and complications of white matter lesions can decrease mortality.
Media
(Click Image to Enlarge)
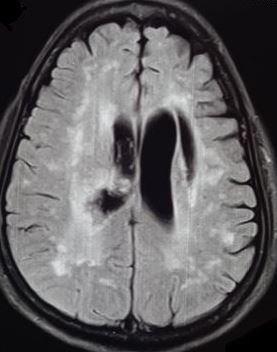
Fazekas Grade 3 White Matter Lesions. Fazekas grade 3 white matter lesions in a case of stroke.
Contributed by S Munakomi, MD
References
Filley CM, Fields RD. White matter and cognition: making the connection. Journal of neurophysiology. 2016 Nov 1:116(5):2093-2104. doi: 10.1152/jn.00221.2016. Epub 2016 Aug 10 [PubMed PMID: 27512019]
Muzio MR, Cascella M. Histology, Axon. StatPearls. 2024 Jan:(): [PubMed PMID: 32119275]
Nave KA, Werner HB. Myelination of the nervous system: mechanisms and functions. Annual review of cell and developmental biology. 2014:30():503-33. doi: 10.1146/annurev-cellbio-100913-013101. Epub [PubMed PMID: 25288117]
Level 3 (low-level) evidenceHachinski VC, Potter P, Merskey H. Leuko-araiosis: an ancient term for a new problem. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 1986 Nov:13(4 Suppl):533-4 [PubMed PMID: 3791068]
Firbank MJ, Teodorczuk A, van der Flier WM, Gouw AA, Wallin A, Erkinjuntti T, Inzitari D, Wahlund LO, Pantoni L, Poggesi A, Pracucci G, Langhorne P, O'Brien JT, LADIS group. Relationship between progression of brain white matter changes and late-life depression: 3-year results from the LADIS study. The British journal of psychiatry : the journal of mental science. 2012 Jul:201(1):40-5. doi: 10.1192/bjp.bp.111.098897. Epub 2012 May 24 [PubMed PMID: 22626634]
Debette S, Beiser A, DeCarli C, Au R, Himali JJ, Kelly-Hayes M, Romero JR, Kase CS, Wolf PA, Seshadri S. Association of MRI markers of vascular brain injury with incident stroke, mild cognitive impairment, dementia, and mortality: the Framingham Offspring Study. Stroke. 2010 Apr:41(4):600-6. doi: 10.1161/STROKEAHA.109.570044. Epub 2010 Feb 18 [PubMed PMID: 20167919]
Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ (Clinical research ed.). 2010 Jul 26:341():c3666. doi: 10.1136/bmj.c3666. Epub 2010 Jul 26 [PubMed PMID: 20660506]
Level 1 (high-level) evidenceKang HJ, Stewart R, Park MS, Bae KY, Kim SW, Kim JM, Shin IS, Cho KH, Yoon JS. White matter hyperintensities and functional outcomes at 2 weeks and 1 year after stroke. Cerebrovascular diseases (Basel, Switzerland). 2013:35(2):138-45. doi: 10.1159/000346604. Epub 2013 Feb 7 [PubMed PMID: 23406918]
Atchaneeyasakul K, Leslie-Mazwi T, Donahue K, Giese AK, Rost NS. White Matter Hyperintensity Volume and Outcome of Mechanical Thrombectomy With Stentriever in Acute Ischemic Stroke. Stroke. 2017 Oct:48(10):2892-2894. doi: 10.1161/STROKEAHA.117.018653. Epub 2017 Sep 8 [PubMed PMID: 28887393]
Smith EE, Saposnik G, Biessels GJ, Doubal FN, Fornage M, Gorelick PB, Greenberg SM, Higashida RT, Kasner SE, Seshadri S, American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Functional Genomics and Translational Biology; and Council on Hypertension. Prevention of Stroke in Patients With Silent Cerebrovascular Disease: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2017 Feb:48(2):e44-e71. doi: 10.1161/STR.0000000000000116. Epub 2016 Dec 15 [PubMed PMID: 27980126]
Zhuang FJ, Chen Y, He WB, Cai ZY. Prevalence of white matter hyperintensities increases with age. Neural regeneration research. 2018 Dec:13(12):2141-2146. doi: 10.4103/1673-5374.241465. Epub [PubMed PMID: 30323144]
GBD 2016 Multiple Sclerosis Collaborators. Global, regional, and national burden of multiple sclerosis 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. Neurology. 2019 Mar:18(3):269-285. doi: 10.1016/S1474-4422(18)30443-5. Epub 2019 Jan 21 [PubMed PMID: 30679040]
Hor JY, Asgari N, Nakashima I, Broadley SA, Leite MI, Kissani N, Jacob A, Marignier R, Weinshenker BG, Paul F, Pittock SJ, Palace J, Wingerchuk DM, Behne JM, Yeaman MR, Fujihara K. Epidemiology of Neuromyelitis Optica Spectrum Disorder and Its Prevalence and Incidence Worldwide. Frontiers in neurology. 2020:11():501. doi: 10.3389/fneur.2020.00501. Epub 2020 Jun 26 [PubMed PMID: 32670177]
Diwanji TP, Engelman A, Snider JW, Mohindra P. Epidemiology, diagnosis, and optimal management of glioma in adolescents and young adults. Adolescent health, medicine and therapeutics. 2017:8():99-113. doi: 10.2147/AHMT.S53391. Epub 2017 Sep 22 [PubMed PMID: 28989289]
Bonkowsky JL, Nelson C, Kingston JL, Filloux FM, Mundorff MB, Srivastava R. The burden of inherited leukodystrophies in children. Neurology. 2010 Aug 24:75(8):718-25. doi: 10.1212/WNL.0b013e3181eee46b. Epub 2010 Jul 21 [PubMed PMID: 20660364]
Level 2 (mid-level) evidenceLanger-Gould A, Zhang JL, Chung J, Yeung Y, Waubant E, Yao J. Incidence of acquired CNS demyelinating syndromes in a multiethnic cohort of children. Neurology. 2011 Sep 20:77(12):1143-8. doi: 10.1212/WNL.0b013e31822facdd. Epub 2011 Aug 24 [PubMed PMID: 21865580]
Level 2 (mid-level) evidenceFornage M, Debette S, Bis JC, Schmidt H, Ikram MA, Dufouil C, Sigurdsson S, Lumley T, DeStefano AL, Fazekas F, Vrooman HA, Shibata DK, Maillard P, Zijdenbos A, Smith AV, Gudnason H, de Boer R, Cushman M, Mazoyer B, Heiss G, Vernooij MW, Enzinger C, Glazer NL, Beiser A, Knopman DS, Cavalieri M, Niessen WJ, Harris TB, Petrovic K, Lopez OL, Au R, Lambert JC, Hofman A, Gottesman RF, Garcia M, Heckbert SR, Atwood LD, Catellier DJ, Uitterlinden AG, Yang Q, Smith NL, Aspelund T, Romero JR, Rice K, Taylor KD, Nalls MA, Rotter JI, Sharrett R, van Duijn CM, Amouyel P, Wolf PA, Gudnason V, van der Lugt A, Boerwinkle E, Psaty BM, Seshadri S, Tzourio C, Breteler MM, Mosley TH, Schmidt R, Longstreth WT, DeCarli C, Launer LJ. Genome-wide association studies of cerebral white matter lesion burden: the CHARGE consortium. Annals of neurology. 2011 Jun:69(6):928-39. doi: 10.1002/ana.22403. Epub [PubMed PMID: 21681796]
Level 2 (mid-level) evidenceFennema-Notestine C, McEvoy LK, Notestine R, Panizzon MS, Yau WW, Franz CE, Lyons MJ, Eyler LT, Neale MC, Xian H, McKenzie RE, Kremen WS. White matter disease in midlife is heritable, related to hypertension, and shares some genetic influence with systolic blood pressure. NeuroImage. Clinical. 2016:12():737-745 [PubMed PMID: 27790395]
Lin J, Wang D, Lan L, Fan Y. Multiple Factors Involved in the Pathogenesis of White Matter Lesions. BioMed research international. 2017:2017():9372050. doi: 10.1155/2017/9372050. Epub 2017 Feb 21 [PubMed PMID: 28316994]
Wardlaw JM, Valdés Hernández MC, Muñoz-Maniega S. What are white matter hyperintensities made of? Relevance to vascular cognitive impairment. Journal of the American Heart Association. 2015 Jun 23:4(6):001140. doi: 10.1161/JAHA.114.001140. Epub 2015 Jun 23 [PubMed PMID: 26104658]
Huang WJ, Chen WW, Zhang X. Multiple sclerosis: Pathology, diagnosis and treatments. Experimental and therapeutic medicine. 2017 Jun:13(6):3163-3166. doi: 10.3892/etm.2017.4410. Epub 2017 Apr 28 [PubMed PMID: 28588671]
Papadopoulos D, Magliozzi R, Mitsikostas DD, Gorgoulis VG, Nicholas RS. Aging, Cellular Senescence, and Progressive Multiple Sclerosis. Frontiers in cellular neuroscience. 2020:14():178. doi: 10.3389/fncel.2020.00178. Epub 2020 Jun 30 [PubMed PMID: 32694983]
Lennon VA, Wingerchuk DM, Kryzer TJ, Pittock SJ, Lucchinetti CF, Fujihara K, Nakashima I, Weinshenker BG. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet (London, England). 2004 Dec 11-17:364(9451):2106-12 [PubMed PMID: 15589308]
Mohammadian M, Roine T, Hirvonen J, Kurki T, Posti JP, Katila AJ, Takala RSK, Tallus J, Maanpää HR, Frantzén J, Hutchinson PJ, Newcombe VF, Menon DK, Tenovuo O. Alterations in Microstructure and Local Fiber Orientation of White Matter Are Associated with Outcome after Mild Traumatic Brain Injury. Journal of neurotrauma. 2020 Dec 15:37(24):2616-2623. doi: 10.1089/neu.2020.7081. Epub 2020 Aug 17 [PubMed PMID: 32689872]
Lock JH, Newman NJ, Biousse V, Peragallo JH. Update on pediatric optic neuritis. Current opinion in ophthalmology. 2019 Nov:30(6):418-425. doi: 10.1097/ICU.0000000000000607. Epub [PubMed PMID: 31433309]
Guidetti D, Rota E, Morelli N, Immovilli P. Migraine and stroke: "vascular" comorbidity. Frontiers in neurology. 2014:5():193. doi: 10.3389/fneur.2014.00193. Epub 2014 Oct 8 [PubMed PMID: 25339937]
Kim TW, Kim YH, Kim KH, Chang WH. White matter hyperintensities and cognitive dysfunction in patients with infratentorial stroke. Annals of rehabilitation medicine. 2014 Oct:38(5):620-7. doi: 10.5535/arm.2014.38.5.620. Epub 2014 Oct 30 [PubMed PMID: 25379491]
van Straaten EC, Fazekas F, Rostrup E, Scheltens P, Schmidt R, Pantoni L, Inzitari D, Waldemar G, Erkinjuntti T, Mäntylä R, Wahlund LO, Barkhof F, LADIS Group. Impact of white matter hyperintensities scoring method on correlations with clinical data: the LADIS study. Stroke. 2006 Mar:37(3):836-40 [PubMed PMID: 16439704]
Andere A, Jindal G, Molino J, Collins S, Merck D, Burton T, Stretz C, Yaghi S, Sacchetti DC, Jamal SE, Reznik ME, Furie K, Cutting S. Volumetric White Matter Hyperintensity Ranges Correspond to Fazekas Scores on Brain MRI. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2022 Apr:31(4):106333. doi: 10.1016/j.jstrokecerebrovasdis.2022.106333. Epub 2022 Feb 11 [PubMed PMID: 35158149]
Parikh S, Bernard G, Leventer RJ, van der Knaap MS, van Hove J, Pizzino A, McNeill NH, Helman G, Simons C, Schmidt JL, Rizzo WB, Patterson MC, Taft RJ, Vanderver A, GLIA Consortium. A clinical approach to the diagnosis of patients with leukodystrophies and genetic leukoencephelopathies. Molecular genetics and metabolism. 2015 Apr:114(4):501-515. doi: 10.1016/j.ymgme.2014.12.434. Epub 2014 Dec 29 [PubMed PMID: 25655951]
Filley CM. Cognitive Dysfunction in White Matter Disorders: New Perspectives in Treatment and Recovery. The Journal of neuropsychiatry and clinical neurosciences. 2021 Fall:33(4):349-355. doi: 10.1176/appi.neuropsych.21030080. Epub 2021 Aug 3 [PubMed PMID: 34340526]
Level 3 (low-level) evidenceWildner P, Stasiołek M, Matysiak M. Differential diagnosis of multiple sclerosis and other inflammatory CNS diseases. Multiple sclerosis and related disorders. 2020 Jan:37():101452. doi: 10.1016/j.msard.2019.101452. Epub 2019 Oct 15 [PubMed PMID: 31670010]
Hasan TF, Barrett KM, Brott TG, Badi MK, Lesser ER, Hodge DO, Meschia JF. Severity of White Matter Hyperintensities and Effects on All-Cause Mortality in the Mayo Clinic Florida Familial Cerebrovascular Diseases Registry. Mayo Clinic proceedings. 2019 Mar:94(3):408-416. doi: 10.1016/j.mayocp.2018.10.024. Epub [PubMed PMID: 30832790]
Scalfari A, Neuhaus A, Degenhardt A, Rice GP, Muraro PA, Daumer M, Ebers GC. The natural history of multiple sclerosis: a geographically based study 10: relapses and long-term disability. Brain : a journal of neurology. 2010 Jul:133(Pt 7):1914-29. doi: 10.1093/brain/awq118. Epub 2010 Jun 9 [PubMed PMID: 20534650]
Alexander M, Murthy JM. Acute disseminated encephalomyelitis: Treatment guidelines. Annals of Indian Academy of Neurology. 2011 Jul:14(Suppl 1):S60-4. doi: 10.4103/0972-2327.83095. Epub [PubMed PMID: 21847331]
Habes M, Erus G, Toledo JB, Zhang T, Bryan N, Launer LJ, Rosseel Y, Janowitz D, Doshi J, Van der Auwera S, von Sarnowski B, Hegenscheid K, Hosten N, Homuth G, Völzke H, Schminke U, Hoffmann W, Grabe HJ, Davatzikos C. White matter hyperintensities and imaging patterns of brain ageing in the general population. Brain : a journal of neurology. 2016 Apr:139(Pt 4):1164-79. doi: 10.1093/brain/aww008. Epub 2016 Feb 24 [PubMed PMID: 26912649]
Sexton CE, Betts JF, Demnitz N, Dawes H, Ebmeier KP, Johansen-Berg H. A systematic review of MRI studies examining the relationship between physical fitness and activity and the white matter of the ageing brain. NeuroImage. 2016 May 1:131():81-90. doi: 10.1016/j.neuroimage.2015.09.071. Epub 2015 Oct 16 [PubMed PMID: 26477656]
Level 1 (high-level) evidenceLin C, Huang CM, Fan YT, Liu HL, Chen YL, Aizenstein HJ, Lee TM, Lee SH. Cognitive Reserve Moderates Effects of White Matter Hyperintensity on Depressive Symptoms and Cognitive Function in Late-Life Depression. Frontiers in psychiatry. 2020:11():249. doi: 10.3389/fpsyt.2020.00249. Epub 2020 Apr 8 [PubMed PMID: 32322221]