Introduction
Yellow fever is a mosquito-borne viral illness found in tropical and subtropical areas in South America and Africa. Transmission is primarily via Aedes and Haemagogus species of mosquito. It can present with varying clinical features ranging from a self-limited, mild febrile illness to severe hemorrhage and liver disease. The “yellow” comes from jaundice that affects some patients with severe disease. The disease is diagnosed by history travel to an endemic area, exposure to infected mosquitoes, vaccination history, symptoms, and laboratory findings. Most cases are self-limited and resemble many other common viral infections. Of those who develop severe disease mortality can approach 50%. Unlike many other mosquito-transmitted viruses, infected humans are not dead-end hosts and may infect mosquitoes during periods of viremia and spread the virus. There is no specific antiviral therapy, but there is an effective vaccine recommended for travelers to endemic areas. Other than vaccination, prevention of mosquito bites is the best way to avoid contracting the virus.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The virus is an RNA virus of the genus Flavivirus, closely related to the viruses that cause West Nile, St. Louis, and Japanese encephalitis. Tree-hole breeding mosquitoes, such as Aedes aegypti and Haemagogous species, transmit yellow fever during the rainy season. The yellow fever virus has three distinct transmission cycles: jungle, intermediate, and urban. The jungle cycle involves transmission between non-human primates (monkeys) and mosquitoes. Humans are infected through infected mosquito bites while visiting or working in the jungle. The intermediate cycle occurs in the African savannah and involves humans who live or work in jungle border areas. Transmission may be between monkeys and humans or humans via mosquito vectors. The urban cycle involves a viremic human who contracted the virus in either the jungle or intermediate cycle who then returns to an urban area. Humans develop significant viremia to infect mosquitoes, which can then transmit the virus to other humans in urban areas. Person to person or primate to human transmission has not been reported without the involvement of a mosquito vector. [4][5]
Epidemiology
Vaccination has decreased worldwide epidemics of yellow fever, but the infection has reemerged in many parts of Africa and South America. No one is immune from yellow fever, and it occurs in people of all ages and races. The highest mortality rates are reported in infants and the elderly, who often have depressed immune systems. yellow fever is very rare in the United States. Most cases are diagnosed in unvaccinated travelers to sub-Saharan Africa or South America. While most people develop a self-limited infection, those who develop severe disease.[6]
Pathophysiology
The incubation period is 3 to 6 days. Once acquired, the virus quickly spreads to multiple organs in the body. The liver is the most important organ affected by yellow fever. It produces profound jaundice due to liver damage. The kidneys also undergo similar pathological alterations and can lead to acute renal failure. When the upper gastrointestinal (GI) tract is involved, the gastric acid mixed with blood produces what is known as black vomit. Central nervous system (CNS) features include cerebral edema and hemorrhage. Encephalopathy is also a common feature of yellow fever.[7][8]
History and Physical
The diagnosis requires a thorough travel history and record of immunization. Patients may present with headache, malaise, jaundice, and myalgias with severe back pain commonly reported.
The incubation period is 3-7 days, with most individuals having mild flu like illness. About 15% of cases have severe symptoms including chills, low back pain, headache, and fever.
There is a period of remission which may last 24-48 hours. This may be followed by a return of symptoms and marked intoxication. During this stage, the hepatorenal disease is common and carries a high mortality.
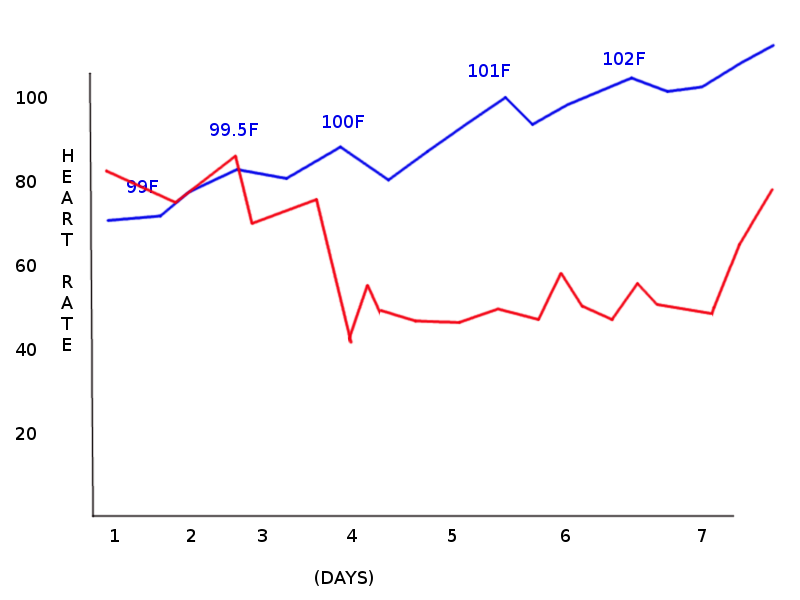
A physical exam may reveal the Faget sign or pulse fever dissociation, facial flushing, and conjunctival injection. During the most toxic phase, patients develop jaundice, dark urine, and vomiting. Bleeding may occur from mucous membranes and in the gastrointestinal tract. Symptoms may mimic those of malaria, leptospirosis, viral hepatitis, other hemorrhagic fevers, dengue, and other flavivirus infections.
Evaluation
Rapid detection methods include the detection of yellow fever antigen using monoclonal enzyme immunoassay in serum specimens and detection of viral genome sequences using polymerase chain reaction (PCR) assay. Yellow fever can be diagnosed using ELISA and serology titers of antibodies. Other investigations depend on what organ is involved. If there is evidence of altered mentation, a lumbar puncture and a CT scan are performed. Blood work may reveal leukopenia with elevated transaminase levels. Neutropenia is common during the first week of the infection.
If the liver is involved, the coagulation profile may be abnormal. Elevation in creatinine, hypoglycemia and metabolic acidosis are strongly associated with a very poor prognosis.
Most yellow fever specific testing can be done at the CDC, but reports will be sent to the state health department. When sending blood samples directly to the CDC, the health department should be informed.[3]
A chest x-ray is done in patients with respiratory distress because of the pulmonary edema. ECG may identify prolonged QT and PR intervals. Arrhythmias are common when the myocardium is affected.
Treatment / Management
Yellow fever is a reportable infection. Once the virus is contracted, symptoms develop after 3 to 6 days. There is no specific treatment, but severe cases require aggressive supportive care and hydration. Patients should be managed in the intensive care unit (ICU) and closely monitored for disseminated intravascular coagulation (DIC), hemorrhage, kidney, and liver dysfunction. Coagulopathy is managed with fresh frozen plasma, and renal failure may require dialysis. Even though yellow fever is not transmitted from person to person, isolation of the individual should be undertaken until the diagnosis is confirmed. Universal precautions are required when looking after patients with yellow fever although person-person transmission of the virus is unlikely. Infected patients should avoid mosquitoes, as they may transmit the virus to mosquitoes, which can serve as vectors for infection other patients.
Since there is no effective treatment or vaccine, prevention is critical. This is best accomplished by avoiding mosquito bites entirely. Even very short periods outdoors can lead to exposure to mosquito bites, so people should wear proper protective clothing. This protection includes long sleeves, long pants, socks, and closed-toe shoes. Pant legs can be tucked into socks to prevent bites to exposed ankles. Transmission is common during the warmer months, and mosquitoes may bite through very thin clothing, so treating clothing with repellents containing permethrin, DEET, oil of lemon eucalyptus, or other EPA-registered insect repellants will reduce this risk. Permethrin should not be applied directly to the skin, but when applied to clothing, it provides protection even after the clothing is washed. Transmission is most frequent when mosquitoes feed, between dawn and dusk, so outdoor activities during this period should be avoided. However, one of the mosquitos responsible for transmitting the virus, Aedes Aegypty, feeds during the daytime; so there is no safe time during the day for a traveler without repellent and wearing protective clothing. Travelers should sleep in air-conditioned spaces or use mosquito nets or screens to prevent bites during sleep. Standing water is a breeding ground for mosquitoes, so flower pots, buckets, and other containers should be drained. Children’s wading pools should be emptied and stored on their sides, and tire swings should have holes drilled into the bottom to allow trapped water to drain.
There is a safe and highly effective live-attenuated vaccine available to prevent yellow fever. A single dose confers lifelong immunity and is effective within 30 days for 99% of patients. Patients with relative contraindications to live attenuated vaccine who plan to travel to endemic areas should review the recommendations for vaccination prior to travel.[9][10][11]
Differential Diagnosis
The differential diagnosis of yellow fever is broad and makes a careful travel history important. It includes:
- Viral hemorrhagic fevers
- Viral hepatitis
- Malaria
- Lassa fever
- Ebola virus
- Typhoid fever
- Dengue fever
- Disseminated Intravascular Coagulation
- Louse-borne relapsing fever
- West Nile virus encephalitis
- Japanese encephalitis
- Herpes simplex encephalitis
- Eastern and Western equine encephalitis
- Venezuelan Equine encephalitis
- Enterovirus meningitis
- Mycoplasma meningitis
- Cytomegalovirus infection in immunocompromised host
- Tuberculous meningitis
- Nipah virus infection
- Rocky Mountain spotted fever
- Fungal meningitis
- Leptospirosis
- Neurocysticercosis
- Amebic meningoencephalitis
Prognosis
Most cases are subclinical or mildly symptomatic with an excellent prognosis. About 15% of symptomatic patients will develop severe disease. Most will recover, but after a bout of yellow fever, full recovery may take weeks or months. In most cases, there is a reversal of the liver and renal dysfunction. Death occurs in 30% to 50% of patients with severe disease. All travelers to endemic areas should be vaccinated if they are candidates for the live attenuated vaccine.
Death often occurs within 2 weeks during the toxic phase of the infection. Unvaccinated travelers to endemic areas are at high risk for developing symptomatic disease compared to the natives, who have acquired immunity. Rare cases of neurologic and viscerotropic disease have been reported following vaccination.
Complications
- Multiorgan failure
- ARDS
- Sepsis
- Respiratory failure
- Myocarditis
- Encephalitis
- Hemorrhage
- DIC
Pearls and Other Issues
Continuous medical education can be obtained through the CDC website regarding yellow fever and yellow fever vaccine.
Enhancing Healthcare Team Outcomes
Yellow fever is endemic in many parts of the world. The key to this infection is prevention. While the acute infection is managed by an interprofessional group of healthcare professionals, prevention is best done by a coordinated effort of educating patients by the primary care provider, infectious disease nurse, and pharmacist. All travelers to endemic regions should be educated about the vaccine, which confers lifelong immunity. Rarely some individuals may require a booster dose after ten years before traveling to an endemic area. Further, all laboratory workers who regularly handle yellow fever containing blood samples should have their neutralizing antibody titers measured every ten years to determine if they need a booster shot. The pharmacist and nurse should also educate the traveler on wearing long-sleeved garments, sleeping under a net and using DEET containing repellant spray.
Since there is no effective treatment or vaccine, prevention is critical. This is best accomplished by avoiding mosquito bites entirely. Even very short periods outdoors can lead to exposure to mosquito bites, so people should wear proper protective clothing. This protection includes long sleeves, long pants, socks, and closed-toe shoes. Pant legs can be tucked into socks to prevent bites to exposed ankles. Transmission is common during the warmer months, and mosquitoes may bite through very thin clothing, so treating clothing with repellents containing permethrin, DEET, oil of lemon eucalyptus, or other EPA-registered insect repellants will reduce this risk. Permethrin should not be applied directly to the skin, but when applied to clothing, it provides protection even after the clothing is washed. Transmission is most frequent when mosquitoes feed, between dawn and dusk, so outdoor activities during this period should be avoided. However, one of the mosquitos responsible for transmitting the virus, Aedes Aegypty, feeds during the daytime; so there is no safe time during the day for a traveler without repellent and wearing protective clothing. Travelers should sleep in air-conditioned spaces or use mosquito nets or screens to prevent bites during sleep. Standing water is a breeding ground for mosquitoes, so flower pots, buckets, and other containers should be drained. Children’s wading pools should be emptied and stored on their sides, and tire swings should have holes drilled into the bottom to allow trapped water to drain.
It is very unlikely that yellow fever will be eradicated anytime soon. The mosquitoes also transmit the sylvatic form via nonhuman primates. Additionally, deforestation and urbanization have reintroduced the virus into the cities. Plus, there is a limited amount of resources available. [12][13](Level V)
Outcomes
Yellow fever can be self-limited or in some cases be life-threatening. Data indicate that about 10-25% of patients will develop severe symptoms that include jaundice, fever, renal and liver failure. The case fatality rates are slightly lower in West Africa compared to South America. However, the ultimate mortality depends on the virulence of the infecting strain and patient susceptibility. Overall, about 3-70% of patients die after contracting yellow fever; the higher mortality is usually in patients with liver and renal damage. Deaths tend to occur within the first 10 days of the toxic phase. Both infants and the elderly are more likely to die than other individuals. Individuals who are unvaccinated usually develop more severe disease than natives. Finally, there are rare cases of post-vaccination neurological deficits and viscerotropic disease leading to death.[14][15] (Level V)
Media
(Click Image to Enlarge)
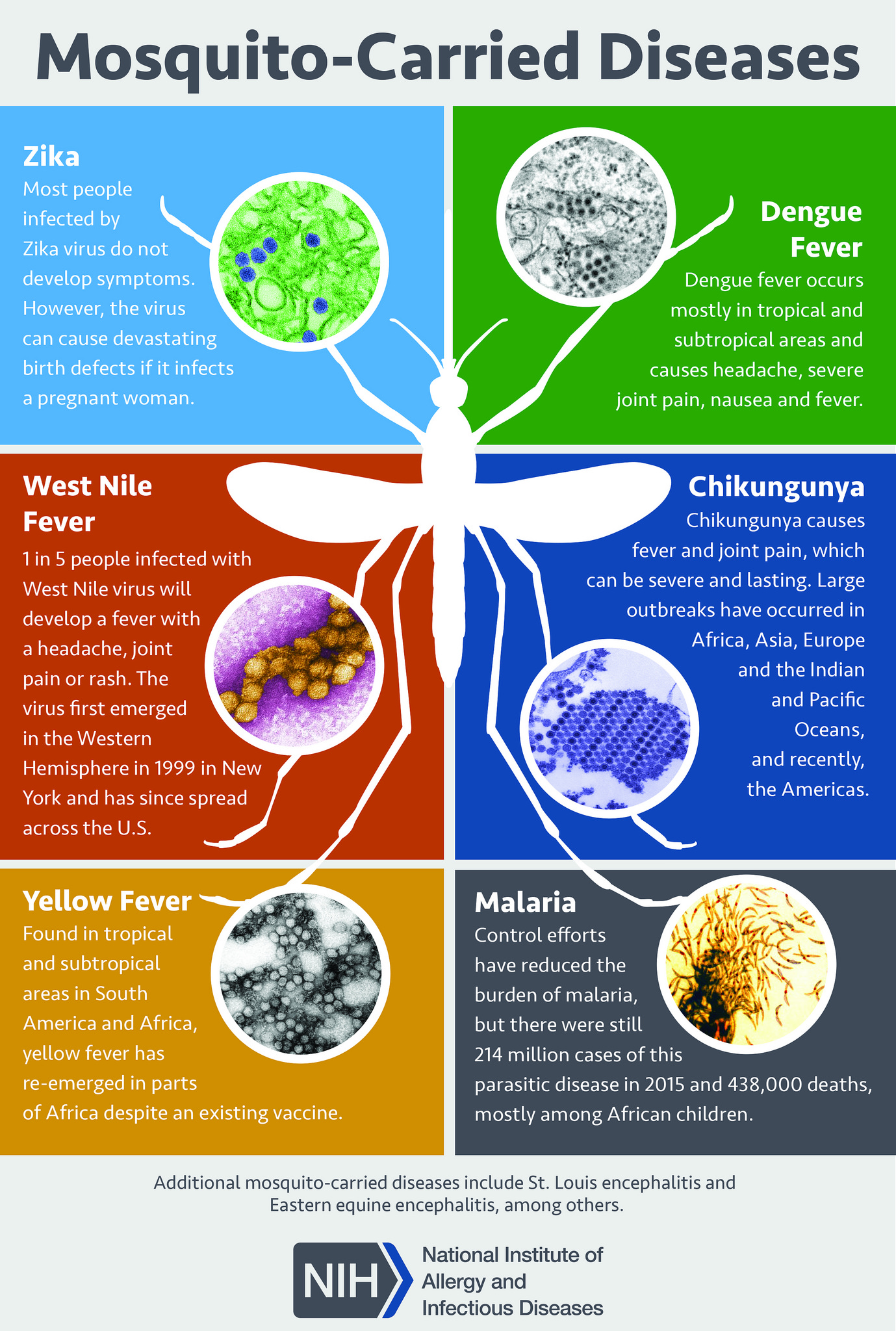
Mosquito-Borne Diseases. Mosquitoes are carriers of various diseases, including Zika, dengue fever, West Nile fever, chikungunya, yellow fever, and malaria.
National Institute of Allergy and Infectious Diseases, National Institutes of Health
(Click Image to Enlarge)

Aedes species mosquito Image courtesy of S Bhimji MD
(Click Image to Enlarge)
Faget sign Image courtesy Statpearls
References
Chen LH, Kozarsky PE, Visser LG. What's Old Is New Again: The Re-emergence of Yellow Fever in Brazil and Vaccine Shortages. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019 May 2:68(10):1761-1762. doi: 10.1093/cid/ciy777. Epub [PubMed PMID: 30204852]
Sanna A, Andrieu A, Carvalho L, Mayence C, Tabard P, Hachouf M, Cazaux CM, Enfissi A, Rousset D, Kallel H. Yellow fever cases in French Guiana, evidence of an active circulation in the Guiana Shield, 2017 and 2018. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2018 Sep:23(36):. doi: 10.2807/1560-7917.ES.2018.23.36.1800471. Epub [PubMed PMID: 30205871]
Level 3 (low-level) evidenceLeong WY. New diagnostic tools for yellow fever. Journal of travel medicine. 2018 Jan 1:25(1):. doi: 10.1093/jtm/tay079. Epub [PubMed PMID: 30184173]
Javelle E, Gautret P, Raoult D. Towards the risk of yellow fever transmission in Europe. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2019 Jan:25(1):10-12. doi: 10.1016/j.cmi.2018.08.015. Epub 2018 Aug 28 [PubMed PMID: 30170135]
Kaul RB, Evans MV, Murdock CC, Drake JM. Spatio-temporal spillover risk of yellow fever in Brazil. Parasites & vectors. 2018 Aug 29:11(1):488. doi: 10.1186/s13071-018-3063-6. Epub 2018 Aug 29 [PubMed PMID: 30157908]
Chippaux JP, Chippaux A. Yellow fever in Africa and the Americas: a historical and epidemiological perspective. The journal of venomous animals and toxins including tropical diseases. 2018:24():20. doi: 10.1186/s40409-018-0162-y. Epub 2018 Aug 25 [PubMed PMID: 30158957]
Level 2 (mid-level) evidenceBarrett ADT. The reemergence of yellow fever. Science (New York, N.Y.). 2018 Aug 31:361(6405):847-848. doi: 10.1126/science.aau8225. Epub 2018 Aug 23 [PubMed PMID: 30139914]
Faria NR, Kraemer MUG, Hill SC, Goes de Jesus J, Aguiar RS, Iani FCM, Xavier J, Quick J, du Plessis L, Dellicour S, Thézé J, Carvalho RDO, Baele G, Wu CH, Silveira PP, Arruda MB, Pereira MA, Pereira GC, Lourenço J, Obolski U, Abade L, Vasylyeva TI, Giovanetti M, Yi D, Weiss DJ, Wint GRW, Shearer FM, Funk S, Nikolay B, Fonseca V, Adelino TER, Oliveira MAA, Silva MVF, Sacchetto L, Figueiredo PO, Rezende IM, Mello EM, Said RFC, Santos DA, Ferraz ML, Brito MG, Santana LF, Menezes MT, Brindeiro RM, Tanuri A, Dos Santos FCP, Cunha MS, Nogueira JS, Rocco IM, da Costa AC, Komninakis SCV, Azevedo V, Chieppe AO, Araujo ESM, Mendonça MCL, Dos Santos CC, Dos Santos CD, Mares-Guia AM, Nogueira RMR, Sequeira PC, Abreu RG, Garcia MHO, Abreu AL, Okumoto O, Kroon EG, de Albuquerque CFC, Lewandowski K, Pullan ST, Carroll M, de Oliveira T, Sabino EC, Souza RP, Suchard MA, Lemey P, Trindade GS, Drumond BP, Filippis AMB, Loman NJ, Cauchemez S, Alcantara LCJ, Pybus OG. Genomic and epidemiological monitoring of yellow fever virus transmission potential. Science (New York, N.Y.). 2018 Aug 31:361(6405):894-899. doi: 10.1126/science.aat7115. Epub 2018 Aug 23 [PubMed PMID: 30139911]
Level 2 (mid-level) evidenceLee H, Halverson S, Ezinwa N. Mosquito-Borne Diseases. Primary care. 2018 Sep:45(3):393-407. doi: 10.1016/j.pop.2018.05.001. Epub [PubMed PMID: 30115330]
Callender DM. Management and control of yellow fever virus: Brazilian outbreak January-April, 2018. Global public health. 2019 Mar:14(3):445-455. doi: 10.1080/17441692.2018.1512144. Epub 2018 Aug 18 [PubMed PMID: 30122143]
Peyraud N, Quéré M, Duc G, Chèvre C, Wanteu T, Reache S, Dumont T, Nesbitt R, Dahl E, Gignoux E, Albela M, Righetti A, Bottineau MC, Cabrol JC, Sarafini M, Nzalapan S, Lechevalier P, Rambaud C, Rull M. A post-conflict vaccination campaign, Central African Republic. Bulletin of the World Health Organization. 2018 Aug 1:96(8):540-547. doi: 10.2471/BLT.17.204321. Epub 2018 Jun 20 [PubMed PMID: 30104794]
Konan YL, Coulibaly ZI, Allali KB, Tétchi SM, Koné AB, Coulibaly D, Ekra KD, Doannio JM, Oudéhouri-Koudou P. [Management of the yellow fever epidemic in 2010 in Séguéla (Côte d'Ivoire): value of multidisciplinary investigation]. Sante publique (Vandoeuvre-les-Nancy, France). 2014 Nov-Dec:26(6):859-67 [PubMed PMID: 25629680]
Level 3 (low-level) evidenceBassolé A. [In Burkina Faso: general mobilization in favor of the "vaccination commando"]. Hygie. 1986 Mar:5(1):31-4 [PubMed PMID: 3699829]
Zahouli JBZ, Koudou BG, Müller P, Malone D, Tano Y, Utzinger J. Urbanization is a main driver for the larval ecology of Aedes mosquitoes in arbovirus-endemic settings in south-eastern Côte d'Ivoire. PLoS neglected tropical diseases. 2017 Jul:11(7):e0005751. doi: 10.1371/journal.pntd.0005751. Epub 2017 Jul 13 [PubMed PMID: 28704434]
Barte H, Horvath TH, Rutherford GW. Yellow fever vaccine for patients with HIV infection. The Cochrane database of systematic reviews. 2014 Jan 23:(1):CD010929. doi: 10.1002/14651858.CD010929.pub2. Epub 2014 Jan 23 [PubMed PMID: 24453061]
Level 2 (mid-level) evidence