Introduction
The aortic valve is a semilunar valve with three leaflets, which lies at the junction of left ventricle and aorta. It allows unidirectional blood flow from the left ventricle to the aorta and the rest of the body. Because of the highly complex and sophisticated cellular and molecular functions, the thin valve leaflet can withstand extreme mechanical and hemodynamic forces with every cardiac cycle.[1] Various factors including age and congenital defects can compromise the normal valvular function leading to a wide variety of complications.[2]
Although bicuspid aortic valves (BAV) are the most common congenital abnormality, congenital valve defects can range from aortic atresia (missing or incomplete closure of aortic valves) to a sub or supra-valvular stenosis. BAV is reported to have an incidence of 1 to 2% with a male predominance. Lack of microfibrillar proteins during valvulogenesis has been reported to affect the leaflet development where two leaflets are fused to form one large leaflet. It frequently correlates with aortic abnormalities such as aortic dilation (root, ascending and arch) and coarctation of the aorta.[3] The bicuspid aortic valve leaflets can undergo accelerated calcific degeneration because of abnormal hemodynamic forces.
Congenital abnormalities including BAV can lead to various valvular complications including aortic stenosis and aortic regurgitation leading to an increased risk to infective endocarditis, which has a reported incidence of 12 to 39% in BAV.[3] Unless severe, BAV generally remains asymptomatic until the age of 50 to 60 years.
Aortic stenosis (AS) is a narrowing of the valve aperture reducing the aortic valve area. Increased resistance to blood flow and transvalvular pressure gradient causes increased left ventricle workload causing hypertrophy. Its prevalence increases with age and can be as high as 4.6% in people greater than age 75 years. Being the most common valvular disease in Europe and America, estimates are that 3.5 million people in England alone will have AS by the year 2020.[4] Calcific degeneration leading to stiffening and restriction motion of valve leaflet is the most common cause of AS. Disruption of endothelium lining on the aortic side caused by increased mechanical stress seem to be the inciting event. Posterior leaflets are reported to be affected the most.[5] Rheumatic fever causing inflammation of the leaflets is still the leading cause of AS in developing countries.
AS can be asymptomatic or can cause symptoms of syncope, angina and heart failure.[6] Severe AS is fatal with a 50% mortality at 2 years.[7] As per The American College of Cardiology/American Heart Association (ACC/AHA) guidelines, AS is graded severe when the orifice area is less than 1.0 cm, the mean gradient is greater than 40 mmHg or the jet velocity is greater than 4 m/s. Prognosis is poor in symptomatic or severe cases unless the valve is replaced. Up to 30% of patients aged > 75 do not undergo surgical valve replacement either because of technical reasons; this may include porcelain aorta, general frailty, refusal to undergo surgery, and serious comorbid conditions.[8] The operative death risk for surgical aortic valve replacement (SAVR) is as high as 10% in patients with LV dysfunction, chronic renal disease, and advanced age.[9] Trans-catheter aortic valve replacement and trans-catheter aortic valve implantation (TAVR/TAVI) have emerged as a more feasible and less risky option for patients not suitable for surgery.
Aortic regurgitation (AR) is the backflow of blood from the aorta to the left ventricle when the valve leaflets fail to coapt. Common causes include congenital defects, calcific degeneration, infective endocarditis, rheumatic fever, and trauma.[10][11][12][13] Ventricular hypertrophy in chronic cases accommodates increased volume to maintain the normal stroke volume and end-diastolic pressure; hence, chronic AR can be asymptomatic for decades.[14] In contrast, with acute cases of AR, ventricles do not have enough time to undergo the needed changes such as hypertrophy to accommodate increased volumes. Because of decreased stroke volume, the heart rate increases to maintain cardiac output but is insufficient to meet the demand resulting in increased left atrial pressure, pulmonary edema and cardiogenic shock.
On physical examination, AR murmur is blowing, high-pitched, diastolic, and decrescendo, beginning soon after the aortic component of S (A); it is loudest at the 3rd or 4th left parasternal intercostal space. It also has associations with various other murmurs including:
- “Mid-systolic murmur” because of rapid ejection of an overload of blood from the left ventricle,
- “Austin Flint” murmur is mid-to-late diastolic murmur due to partial closure of mitral valve during ventricular systole because of regurgitant flow from aortic valve,
- “Cole-Cecil” is a diastolic murmur due to the fusion of an aortic murmur with the S3 because of simultaneous filling of the left ventricle from left atrium and AR
History of Valvular Surgery
Dr. Theodore Tuffier, in 1912, used his finger to free the fused leaflets of a stenosed aortic valve.[15] Before the advent of cardiopulmonary bypass (CPB), mitral valve repair involved commissurotomy through access from the left atrial chamber. Thomas Homes Sellors performed first pulmonary valvulotomy in 1948 by using a tenotomy knife.[16] Charles Hufnagel developed the first artificial valve based on a reciprocating ball and cage. It was used to prevent backflow of blood into the ventricles due to aortic insufficiency.[17] CPB machine revolutionized the valve replacement in the anatomical position. Dr. Dwight Harken and his colleagues performed the first successful aortic valve replacement. Later that year, Drs. Albert Starr and Lowell Edwards performed mitral valve replacement.[18] Bioprosthetic valves are closer in function to natural valves but have a limited life expectancy, whereas, Mechanical valves are more durable but require anticoagulation. The choice of valves, among other factors, depends upon the patient’s age and well-being.
Mechanical heart valves are known to last for approximately 25 years. Seventy different mechanical heart valves have been developed since 1960.[19] Ball and cage, bi-leaflet, and tilting disc are the common ones. Modification of the ball valve by Dr. Albert Starr and Lowell Edwards entailed developing a cage made of lucite with a silicone elastomer ball. The cage material was later changed to stainless steel and then cobalt-chromium alloys. The Starr-Edward valve also has a Teflon sewing ring, which enabled suturing into mitral and later into the aortic position.[20]
Increased thrombogenicity has been a significant issue, for which valves underwent several modifications such as measures to reduce metal contact by covering the struts with cloth and using Silastic shields. Other issues included hemolysis due to excessive rubbing of the ball against the sewing ring and occlusion of coronary ostia because of high profile. Despite these issues, these valves showed the feasibility of prosthetic valve enabling Starr-Edwards to draw design criteria. Basic points included that the valves should be chemically inert, biocompatible, a-traumatic to blood, and non-thrombogenic.[21]
In 1965, Kay-Shiley’s non-rotating disc valve replaced the ball with a single disc but demonstrated poor hemodynamics and hemolysis and was discontinued. Bjork-Shiley in 1969 developed a tilting-disc valve, which overcame the problems with the single-disc valve. Free rotation of disc between metal struts allows it to open by tilting at a 60-degree angle. Bjork-Shiley replaced the flat with the convexo-concave disc to create a larger orifice in 1975 but were the object of a recall due to fracture of welded struts.[22]
Medtronic Hall valve developed by Dr. Karl Hall and Robert Kaster is the most common tilting disc valve. Perforation in the middle of the disc served as a guide and an improved tilting angle.[23] In 1977, St Jude Medical developed Bi-leaflet valve, which comprised two semi-circular flaps with hinges close to the center of the orifice. Stagnation of blood flow leading to thrombus formation around the hinge region was a problem with the bi-leaflet valve.[15] A newly developed valve resolved this issue with a valve in which the continuous 360-degree rotation around the central axis of the valve ensured an even distribution of blood flow and prevent thrombus formation.[16]
Predisposition for thrombosis, embolism, need for lifelong anticoagulation therapy are drawbacks of mechanical valves.
Bioprosthetic valves can either be an allograft (cadaver or Ross procedure) or, a xenograft (native or pericardium). The Ross procedure involves replacing the diseased aortic valve with the patient’s own pulmonary valve (autograft) and replace the pulmonary valve with aortic or pulmonary allograft. The pulmonary autograft grows with the patient and does not induce an immunologic response. The most common xenografts are porcine aortic valves and bovine pericardial valves.
Lonescu-Shiley developed xenograft valves by using bovine pericardium on a titanium stent in 1971 but was later withdrawn in 1987 due to structural failure including abrasive tears because of fabric-tissue interface and leaflet calcification. Carpentier-Edwards bovine pericardial valve overcame those issues by making some structural modifications, like stitching pericardium to the inside of the fabric and using flexible stent posts.
Although biological valves have better hemodynamics compared to mechanical valves, they have a shorter lifespan because of calcification, which stiffens the valve leaflets.
Tissues engineering, a field in regenerative medicine restores and maintains the function of living tissues. Skin graft for burn victims is an example. Tissue engineered heart valves (TEHV) are perceived to be non-thrombogenic, and infection resistant. With advancement in material science and culturing techniques, there is the possibility of a TEHV valve that is capable of growing, remodeling and repairing itself as the patients grow.
Polymeric valves have been around for over 50 years, but because the earlier versions were prone to calcification and degradation, they were not widely used and instead only used in bridge devices like artificial hearts and left ventricular assist devices. Besides the advantage that they can be produced in various shapes and sizes,[17] they are known to combine the durability of mechanical valves and the hydrodynamic function of bioprosthetic valves.[18] The earliest polymeric valve implanted in a 44-year-old female in 1958 at the mitral position was a polyurethane design with Teflon chordae tendinae.[18][24] Polyurethane valves have been found to have better hemodynamics compared to bioprosthetic valves and a lower incidence of thrombogenicity than mechanical valves. With advances in material sciences, the future of polymeric valves seems promising.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The heart has four chambers (right atrium, right ventricle, left atrium, and left ventricle) and four valves (tricuspid, pulmonary, mitral, and aortic valves). Valves between the atriums and ventricles (tricuspid and mitral) are called “atrioventricular” valve and valves between arteries and ventricles (aortic and pulmonary) are called “arterioventricular” valves. The aortic and pulmonary valves are also called semilunar valves because of their half-moon-like shape. Atrioventricular valves are considered to be the active structures because their attachment to the heart muscle through papillary muscles and fibrous cords makes them respond to myocardial contractions. Semilunar valves historically were considered functioning passively in response to blood flow since they do not have a direct attachment of the mobile part of the leaflet to the myocardium.
Although it is partly true, it now is known that valve’s sophisticated design and complex cellular components play an essential role in maintaining normal valve function.[1]
The aortic valve, like other valves, permits the blood flow in one direction, from the left ventricle to aorta. It is reported to open and closes over 100,000 times a day and 3.7 billion times in a lifespan. Aortic valve has three leaflets (movable parts) and three sinuses, which are cavities behind the leaflets. Two of these sinuses have apertures of right and left coronary arteries, hence are called right coronary sinus and left coronary sinus. The third sinus is a blind sac and is called non-coronary or posterior sinus.[1]
Indications
While medical treatment has not shown to prevent or delay the onset of valvular disease,[14] surgical replacement is considered the most effective treatment for AS and AR. Balloon valvotomy serves as a bridge to surgery, but it is not considered an alternative to valve replacement since it only provides temporary relief of symptoms.
AS is classified based on effective orifice area (EOA), the jet velocity, the ejection fraction, and the transvalvular pressure gradient. Two of the most common approaches to determine EOA are Gorlin formula and continuity equation. Doppler echocardiography is used to determine velocity time integral (VTI), which is the smallest cross-sectional area of the stream, to estimate EOA using continuity equation. However, it sometimes overestimates the severity, which can lead to unnecessary intervention.
Due to the growing success of TAVR, ACC/AHA guidelines for the indications of AVR changed in 2014.[25] ACC/AHA now recommends TAVR as the choice of intervention in the following situations:
1) Patients considered to be at prohibitive risk for surgery and a predicted post-TAVR survival longer than 12 months (class I indication, level of evidence B).
2) As an alternative to SAVR in patients considered to be at high risk for surgery (class IIa indication, level of evidence B).
SAVR Versus TAVR
From 2004 to 2008, aortic valve replacement (AVR) had a mortality of 2.8%. Due to porcelain aorta and high surgical risk, 1/3 of the patients with severe AS aged greater than 75 are deemed unsuitable for aortic valve replacement.[8] On the other hand, in neonates and children, AVR has practical implications since with growth they would need frequent replacements, and current mechanical and bioprosthetic valves are just too big. Ross procedure, although successful, has its particular challenges like technical expertise and replacing the healthy pulmonary valve.
Andersen et al. demonstrated the feasibility of TAVR in 1992 using a porcine aortic valve folded into a balloon expandable stent.[26] The primary advantage of TAVR is that the valve can be deployed percutaneously over the native valve without the need for open-heart surgery; this is a huge step forward for patients who have been refused surgery due to high risk. Since approval of TAVR in the United States, the Society of Thoracic Surgeons/ACC Trans-catheter Valve Therapy Registry investigators have reported a procedural success of 92%.[27] Imaging studies like trans-thoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) provide enough information needed for before TTE. However, they can underestimate the aortic valve area due to the ellipsoidal nature of the annulus which can lead to patient-prosthesis mismatch (PPM). Multislice computed tomography among other things like degree of arterial tortuosity and aortic root calcification has shown to more accurately predict the annulus size.[28]
In patients with systolic dysfunction, TAVR has shown to normalize ventricular-arterial coupling, decrease LV hypertrophy and restore normal LV function.[29][30] In one-third of severe AS cases elevated left-sided filling pressures lead to severe pulmonary hypertension. Sustained reduction in pulmonary hypertension has been noted in patients who underwent TAVR.[31] Trans-catheter Endovascular Implantation of VALves (REVIVAL) trial studied TTE in 95 patients before and after newly designed valve implantation, which revealed that mean valve area achieved by TAVR was comparable to what was achieved by SAVR.[32] Although there was a slight progression of aortic regurgitation at 1 year, reports show that patients have an improvement in LV structure and function.[33]
Sequelae of TAVR
Major complications associated with TAVR are para-valvular leaks, stent migration, conduction disturbances, and stroke.[34]
Para-valvular leakage (PVL) or LVOT obstruction can occur due to stent migration or rotation if the calcific nodules on the native valves are not sufficient to anchor the stent.[35][36] It correlates with increased mortality.[37][38] Annulus-prosthesis size mismatch can also cause PVL.[39] Balloon post-dilation is done after TAVR to reduce PVL, but it has its downsides like over dilation can lead to poor leaflet opposition, cerebral vascular events, and even rupture of the aortic annulus.[40][41] Making sure that the balloon diameter is not bigger than the maximum diameter of the aortic valve can prevent this concern.[39] A new valve design valve with a sealing skirt at the lower position is shown to decrease the rate of para-valvular regurgitation[62, 63]. Increased procedural experience and technique along with better case selection has been shown to decrease PVL rates in PARTNER continued-access registry.[42]
Two large randomized trails compared TAVR and SAVR in high-risk patients and revealed that TAVR is associated with a stroke rate from 4 to 5%, which is highest amongst percutaneous cardiac interventions. FDA requires all TAVR patients to have a follow-up CT to look for signs of leaflet immobility since reduced leaflet motion has been shown to associate with an increased incidence of strokes and transient ischemic attacks.
Direct, or near direct, contact of the bioprosthetic valve and coronary ostium can lead to coronary obstruction, which correlates with a high mortality rate.[43] In native valve TAVR, the risk is < 1%, but it goes up 3 to 4 fold in valve-in-valve TAVR.[44] CT and fluoroscopy can be used to detect high-risk cases.[45] Measures like using small diameter prosthesis, under-expansion of a balloon-expandable valve, or active prevention by placing wire and stent in a coronary vessel before valve placement should be considered managing coronary obstruction.[43]
Conduction abnormalities due to compression of atrioventricular (AV) node or His bundle can occur due to oversized valves and if the stent positioning is too deep into the left ventricle outflow tract (LVOT). On the other hand, positioning the valvular prosthesis supra-annularly can increase the risk of coronary ostia occlusion. The need for a permanent pacemaker in PARTNER A Cohort was not significantly different for the patients undergoing TAVR versus SAVR. Siontis and colleagues found that conduction abnormalities were 2.5 times more prevalent with self-expandable valves compared to balloon-expandable valves. They also suggested that male sex, baseline conduction abnormalities, and intra-procedural AV block were predictors of a permanent pacemaker placement after TAVR.[46]
Vascular sequelae are independent predictors of death. Major vascular complications arise after retrograde delivery through the femoral arteries due to the size of trans-catheter valves in a collapsed state. It can lead to dislodging of calcific debris from arteries and can lead to stroke.[34][47] With the new generation Edwards SAPIEN 3 system and CoreValve Evolut R, the expectation is that the rate of vascular complication will continue to decrease.[48][49]
Logistic EuroSCORE and the Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) algorithms are the two most frequently used death-prediction models used for TAVR patients. The trans-apical approach has correlated with a higher mortality rate than the transfemoral route.[50][51] Sequelae of TAVR like cerebral embolism. PVL and vascular sequelae are also well-known predictors of death.
Clinical Significance
Aortic valve replacement is a life-saving procedure. The aortic valve is often affected by either become leaky (aortic insufficiency) or partially blocked (aortic stenosis). Current aortic valve replacement approaches to treat the condition include a sternotomy, minimally invasive cardiac surgery, and transcatheter aortic valve replacement.
Enhancing Healthcare Team Outcomes
Because there are several options today for managing aortic valvular disease, it is important to have an interprofessional team of nurses, cardiologists, and cardiac surgeons assess the patient and make a universal recommendation that includes patient education. The type of treatment recommended usually depends on patient age, comorbidity, personal preferences, surgeon experience, contraindications to anticoagulation, and lifestyle.
Media
(Click Image to Enlarge)
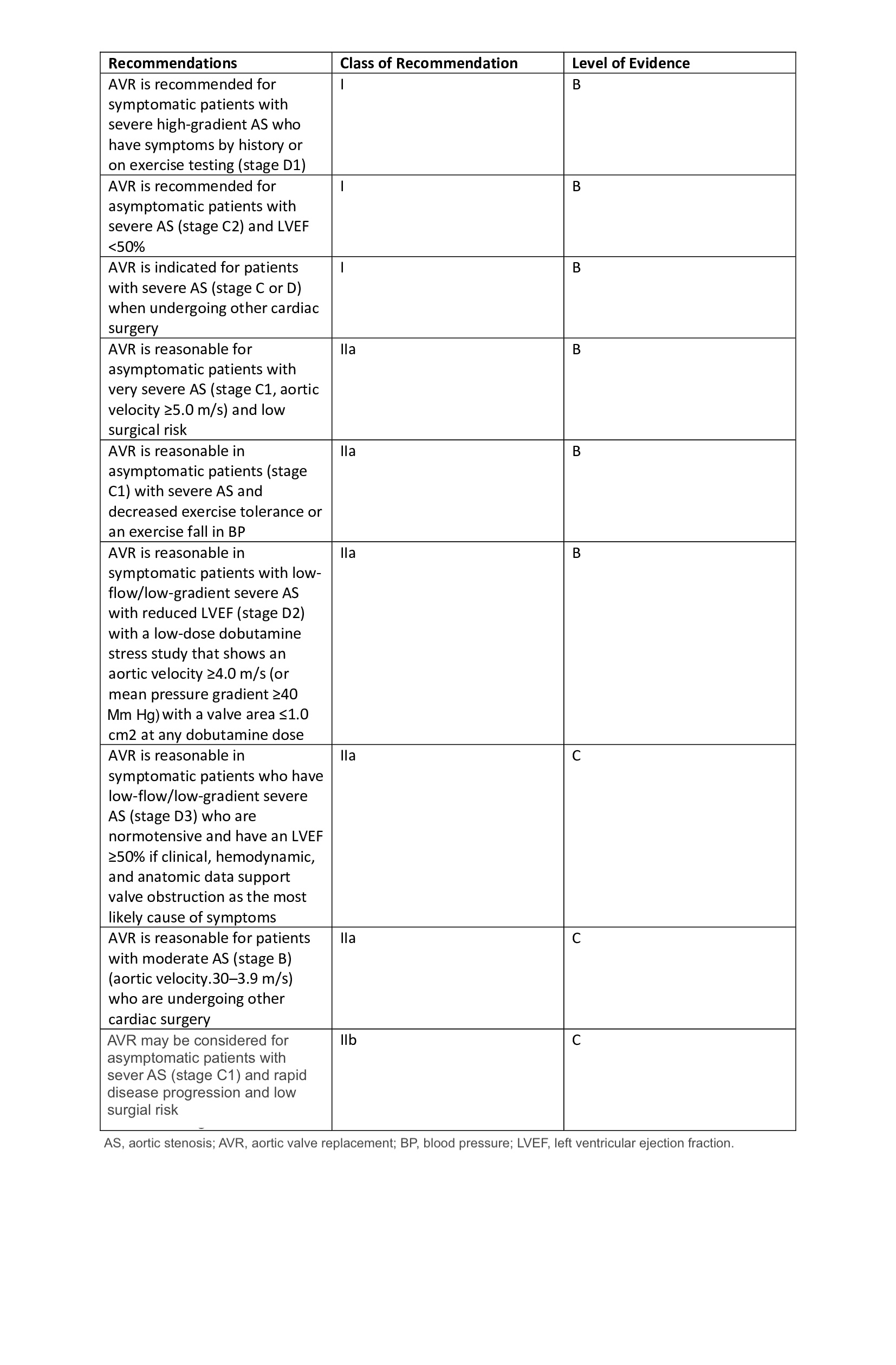
Recommendations for Aortic Valve Replacement.
Contributed by S Harika, MBBS
(Click Image to Enlarge)
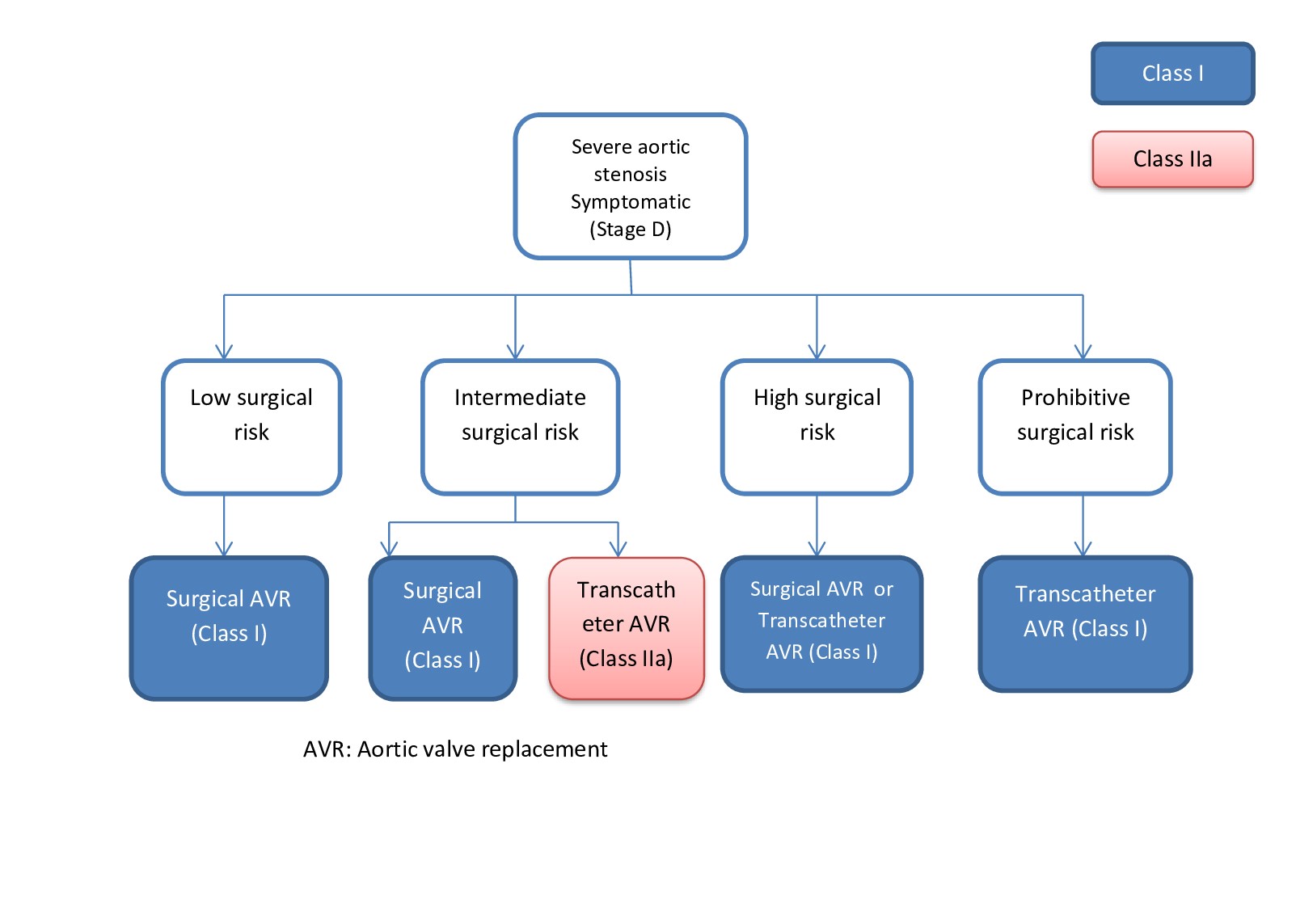
Indications for Aortic Valve Replacement.
Contributed by S Harika Pujari, MD
References
El-Hamamsy I, Balachandran K, Yacoub MH, Stevens LM, Sarathchandra P, Taylor PM, Yoganathan AP, Chester AH. Endothelium-dependent regulation of the mechanical properties of aortic valve cusps. Journal of the American College of Cardiology. 2009 Apr 21:53(16):1448-55. doi: 10.1016/j.jacc.2008.11.056. Epub [PubMed PMID: 19371829]
Level 3 (low-level) evidenceRozeik M, Wheatley D, Gourlay T. The aortic valve: structure, complications and implications for transcatheter aortic valve replacement. Perfusion. 2014 Jul:29(4):285-300 [PubMed PMID: 24570076]
Fedak PW, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002 Aug 20:106(8):900-4 [PubMed PMID: 12186790]
Level 3 (low-level) evidenceIung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European heart journal. 2003 Jul:24(13):1231-43 [PubMed PMID: 12831818]
Level 3 (low-level) evidenceFreeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005 Jun 21:111(24):3316-26 [PubMed PMID: 15967862]
Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, 2006 Writing Committee Members, American College of Cardiology/American Heart Association Task Force. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008 Oct 7:118(15):e523-661. doi: 10.1161/CIRCULATIONAHA.108.190748. Epub 2008 Sep 26 [PubMed PMID: 18820172]
Level 1 (high-level) evidenceVaradarajan P,Kapoor N,Bansal RC,Pai RG, Survival in elderly patients with severe aortic stenosis is dramatically improved by aortic valve replacement: Results from a cohort of 277 patients aged > or =80 years. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2006 Nov; [PubMed PMID: 16950629]
Level 2 (mid-level) evidenceIung B, Cachier A, Baron G, Messika-Zeitoun D, Delahaye F, Tornos P, Gohlke-Bärwolf C, Boersma E, Ravaud P, Vahanian A. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? European heart journal. 2005 Dec:26(24):2714-20 [PubMed PMID: 16141261]
Kvidal P, Bergström R, Malm T, Ståhle E. Long-term follow-up of morbidity and mortality after aortic valve replacement with a mechanical valve prosthesis. European heart journal. 2000 Jul:21(13):1099-111 [PubMed PMID: 10843828]
Level 1 (high-level) evidenceSadee AS, Becker AE, Verheul HA, Bouma B, Hoedemaker G. Aortic valve regurgitation and the congenitally bicuspid aortic valve: a clinico-pathological correlation. British heart journal. 1992 Jun:67(6):439-41 [PubMed PMID: 1622690]
Wise JR Jr, Cleland WP, Hallidie-Smith KA, Bentall HH, Goodwin JF, Oakley CM. Urgent aortic-valve replacement for acute aortic regurgitation due to infective endocarditis. Lancet (London, England). 1971 Jul 17:2(7716):115-21 [PubMed PMID: 4104458]
Shibayama K, Watanabe H, Murai T, Sasaki S, Tabata M, Fukui T, Umemura J, Takanashi S, Sumiyoshi T. Aortic regurgitation caused by cusp bending of aortic valve leaflet. Journal of echocardiography. 2012 Mar:10(1):21-3. doi: 10.1007/s12574-011-0105-x. Epub 2012 Jan 5 [PubMed PMID: 27277925]
Kai H, Koyanagi S, Takeshita A. Aortic valve prolapse with aortic regurgitation assessed by Doppler color-flow echocardiography. American heart journal. 1992 Nov:124(5):1297-304 [PubMed PMID: 1442499]
Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Journal of the American College of Cardiology. 2008 Sep 23:52(13):e1-142. doi: 10.1016/j.jacc.2008.05.007. Epub [PubMed PMID: 18848134]
Level 1 (high-level) evidenceEllis JT, Healy TM, Fontaine AA, Saxena R, Yoganathan AP. Velocity measurements and flow patterns within the hinge region of a Medtronic Parallel bileaflet mechanical valve with clear housing. The Journal of heart valve disease. 1996 Nov:5(6):591-9 [PubMed PMID: 8953436]
Nazarov VM, Zheleznev SI, Bogachev-Prokophiev AV, Afanasyev AV, Nemchenko EV, Jeltovskiy YV, Lavinyukov SO. CardiaMed mechanical valve: mid-term results of a multicenter clinical trial. Asian cardiovascular & thoracic annals. 2014 Jan:22(1):9-17. doi: 10.1177/0218492312464035. Epub 2013 Jul 9 [PubMed PMID: 24585637]
Level 1 (high-level) evidenceGhanbari H, Viatge H, Kidane AG, Burriesci G, Tavakoli M, Seifalian AM. Polymeric heart valves: new materials, emerging hopes. Trends in biotechnology. 2009 Jun:27(6):359-67. doi: 10.1016/j.tibtech.2009.03.002. Epub 2009 May 4 [PubMed PMID: 19406497]
Wheatley DJ, Raco L, Bernacca GM, Sim I, Belcher PR, Boyd JS. Polyurethane: material for the next generation of heart valve prostheses? European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2000 Apr:17(4):440-8 [PubMed PMID: 10773568]
Level 3 (low-level) evidenceVitale N, De Feo M, De Siena P, Cappabianca G, Onorati F, Gregorio R, Branzoli S, de Luca L, Schinosa T, Viganò M, Scardone M, Cotrufo M. Tilting-disc versus bileaflet mechanical prostheses in the aortic position: a multicenter evaluation. The Journal of heart valve disease. 2004 May:13 Suppl 1():S27-34 [PubMed PMID: 15224997]
STARR A, EDWARDS ML. Mitral replacement: clinical experience with a ball-valve prosthesis. Annals of surgery. 1961 Oct:154(4):726-40 [PubMed PMID: 13916361]
Chaikof EL. The development of prosthetic heart valves--lessons in form and function. The New England journal of medicine. 2007 Oct 4:357(14):1368-71 [PubMed PMID: 17914037]
Blot WJ, Ibrahim MA, Ivey TD, Acheson DE, Brookmeyer R, Weyman A, Defauw J, Smith JK, Harrison D. Twenty-five-year experience with the Björk-Shiley convexoconcave heart valve: a continuing clinical concern. Circulation. 2005 May 31:111(21):2850-7 [PubMed PMID: 15927993]
Zilla P, Brink J, Human P, Bezuidenhout D. Prosthetic heart valves: catering for the few. Biomaterials. 2008 Feb:29(4):385-406 [PubMed PMID: 17950840]
Level 3 (low-level) evidenceBraunwald NS. It will work: the first successful mitral valve replacement. The Annals of thoracic surgery. 1989 Sep:48(3 Suppl):S1-3 [PubMed PMID: 2673090]
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD, ACC/AHA Task Force Members. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Jun 10:129(23):e521-643. doi: 10.1161/CIR.0000000000000031. Epub 2014 Mar 3 [PubMed PMID: 24589853]
Level 1 (high-level) evidenceAndersen HR, Knudsen LL, Hasenkam JM. Transluminal implantation of artificial heart valves. Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs. European heart journal. 1992 May:13(5):704-8 [PubMed PMID: 1618213]
Level 3 (low-level) evidenceMack MJ, Brennan JM, Brindis R, Carroll J, Edwards F, Grover F, Shahian D, Tuzcu EM, Peterson ED, Rumsfeld JS, Hewitt K, Shewan C, Michaels J, Christensen B, Christian A, O'Brien S, Holmes D, STS/ACC TVT Registry. Outcomes following transcatheter aortic valve replacement in the United States. JAMA. 2013 Nov 20:310(19):2069-77. doi: 10.1001/jama.2013.282043. Epub [PubMed PMID: 24240934]
Level 2 (mid-level) evidenceBloomfield GS, Gillam LD, Hahn RT, Kapadia S, Leipsic J, Lerakis S, Tuzcu M, Douglas PS. A practical guide to multimodality imaging of transcatheter aortic valve replacement. JACC. Cardiovascular imaging. 2012 Apr:5(4):441-55. doi: 10.1016/j.jcmg.2011.12.013. Epub [PubMed PMID: 22498335]
Poulin F, Carasso S, Horlick EM, Rakowski H, Lim KD, Finn H, Feindel CM, Greutmann M, Osten MD, Cusimano RJ, Woo A. Recovery of left ventricular mechanics after transcatheter aortic valve implantation: effects of baseline ventricular function and postprocedural aortic regurgitation. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2014 Nov:27(11):1133-42. doi: 10.1016/j.echo.2014.07.001. Epub 2014 Aug 7 [PubMed PMID: 25125314]
Level 2 (mid-level) evidenceDi Bello V, Giannini C, De Carlo M, Delle Donne MG, Nardi C, Palagi C, Cucco C, Dini FL, Guarracino F, Marzilli M, Petronio AS. Acute improvement in arterial-ventricular coupling after transcatheter aortic valve implantation (CoreValve) in patients with symptomatic aortic stenosis. The international journal of cardiovascular imaging. 2012 Jan:28(1):79-87. doi: 10.1007/s10554-010-9772-3. Epub 2011 Jan 8 [PubMed PMID: 21222040]
Ben-Dor I, Goldstein SA, Pichard AD, Satler LF, Maluenda G, Li Y, Syed AI, Gonzalez MA, Gaglia MA Jr, Wakabayashi K, Delhaye C, Belle L, Wang Z, Collins SD, Torguson R, Okubagzi P, Aderotoye A, Xue Z, Suddath WO, Kent KM, Epstein SE, Lindsay J, Waksman R. Clinical profile, prognostic implication, and response to treatment of pulmonary hypertension in patients with severe aortic stenosis. The American journal of cardiology. 2011 Apr 1:107(7):1046-51. doi: 10.1016/j.amjcard.2010.11.031. Epub 2011 Feb 4 [PubMed PMID: 21296325]
Level 2 (mid-level) evidenceKodali SK, O'Neill WW, Moses JW, Williams M, Smith CR, Tuzcu M, Svensson LG, Kapadia S, Hanzel G, Kirtane AJ, Leon MB. Early and late (one year) outcomes following transcatheter aortic valve implantation in patients with severe aortic stenosis (from the United States REVIVAL trial). The American journal of cardiology. 2011 Apr 1:107(7):1058-64. doi: 10.1016/j.amjcard.2010.11.034. Epub [PubMed PMID: 21419887]
Yared K, Garcia-Camarero T, Fernandez-Friera L, Llano M, Durst R, Reddy AA, O'Neill WW, Picard MH. Impact of aortic regurgitation after transcatheter aortic valve implantation: results from the REVIVAL trial. JACC. Cardiovascular imaging. 2012 May:5(5):469-77. doi: 10.1016/j.jcmg.2012.02.008. Epub [PubMed PMID: 22595154]
Toggweiler S, Gurvitch R, Leipsic J, Wood DA, Willson AB, Binder RK, Cheung A, Ye J, Webb JG. Percutaneous aortic valve replacement: vascular outcomes with a fully percutaneous procedure. Journal of the American College of Cardiology. 2012 Jan 10:59(2):113-8. doi: 10.1016/j.jacc.2011.08.069. Epub [PubMed PMID: 22222073]
Pang PY, Chiam PT, Chua YL, Sin YK. A survivor of late prosthesis migration and rotation following percutaneous transcatheter aortic valve implantation. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2012 May:41(5):1195-6. doi: 10.1093/ejcts/ezr195. Epub 2012 Jan 6 [PubMed PMID: 22228843]
Level 3 (low-level) evidenceLauten A, Hamadanchi A, Doenst T, Figulla HR. Late migration of balloon-expandable transcatheter aortic valve. European heart journal. 2013 Aug:34(32):2509. doi: 10.1093/eurheartj/eht204. Epub 2013 Jun 11 [PubMed PMID: 23761393]
Level 3 (low-level) evidenceTamburino C, Capodanno D, Ramondo A, Petronio AS, Ettori F, Santoro G, Klugmann S, Bedogni F, Maisano F, Marzocchi A, Poli A, Antoniucci D, Napodano M, De Carlo M, Fiorina C, Ussia GP. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011 Jan 25:123(3):299-308. doi: 10.1161/CIRCULATIONAHA.110.946533. Epub 2011 Jan 10 [PubMed PMID: 21220731]
Kodali S, Pibarot P, Douglas PS, Williams M, Xu K, Thourani V, Rihal CS, Zajarias A, Doshi D, Davidson M, Tuzcu EM, Stewart W, Weissman NJ, Svensson L, Greason K, Maniar H, Mack M, Anwaruddin S, Leon MB, Hahn RT. Paravalvular regurgitation after transcatheter aortic valve replacement with the Edwards sapien valve in the PARTNER trial: characterizing patients and impact on outcomes. European heart journal. 2015 Feb 14:36(7):449-56. doi: 10.1093/eurheartj/ehu384. Epub 2014 Oct 1 [PubMed PMID: 25273886]
Level 1 (high-level) evidenceSinning JM, Vasa-Nicotera M, Chin D, Hammerstingl C, Ghanem A, Bence J, Kovac J, Grube E, Nickenig G, Werner N. Evaluation and management of paravalvular aortic regurgitation after transcatheter aortic valve replacement. Journal of the American College of Cardiology. 2013 Jul 2:62(1):11-20. doi: 10.1016/j.jacc.2013.02.088. Epub 2013 May 1 [PubMed PMID: 23644081]
Level 3 (low-level) evidenceBarbanti M, Yang TH, Rodès Cabau J, Tamburino C, Wood DA, Jilaihawi H, Blanke P, Makkar RR, Latib A, Colombo A, Tarantini G, Raju R, Binder RK, Nguyen G, Freeman M, Ribeiro HB, Kapadia S, Min J, Feuchtner G, Gurtvich R, Alqoofi F, Pelletier M, Ussia GP, Napodano M, de Brito FS Jr, Kodali S, Norgaard BL, Hansson NC, Pache G, Canovas SJ, Zhang H, Leon MB, Webb JG, Leipsic J. Anatomical and procedural features associated with aortic root rupture during balloon-expandable transcatheter aortic valve replacement. Circulation. 2013 Jul 16:128(3):244-53. doi: 10.1161/CIRCULATIONAHA.113.002947. Epub 2013 Jun 7 [PubMed PMID: 23748467]
Level 2 (mid-level) evidenceNombela-Franco L, Rodés-Cabau J, DeLarochellière R, Larose E, Doyle D, Villeneuve J, Bergeron S, Bernier M, Amat-Santos IJ, Mok M, Urena M, Rheault M, Dumesnil J, Côté M, Pibarot P, Dumont E. Predictive factors, efficacy, and safety of balloon post-dilation after transcatheter aortic valve implantation with a balloon-expandable valve. JACC. Cardiovascular interventions. 2012 May:5(5):499-512. doi: 10.1016/j.jcin.2012.02.010. Epub [PubMed PMID: 22625188]
Beohar N, Kirtane AJ, Blackstone E, Waksman R, Holmes D Jr, Minha S, Alli O, Suri RM, Svensson LG, Leon M, Kodali S. Trends in Complications and Outcomes of Patients Undergoing Transfemoral Transcatheter Aortic Valve Replacement: Experience From the PARTNER Continued Access Registry. JACC. Cardiovascular interventions. 2016 Feb 22:9(4):355-363. doi: 10.1016/j.jcin.2015.10.050. Epub 2016 Jan 20 [PubMed PMID: 26803420]
Dvir D, Leipsic J, Blanke P, Ribeiro HB, Kornowski R, Pichard A, Rodés-Cabau J, Wood DA, Stub D, Ben-Dor I, Maluenda G, Makkar RR, Webb JG. Coronary obstruction in transcatheter aortic valve-in-valve implantation: preprocedural evaluation, device selection, protection, and treatment. Circulation. Cardiovascular interventions. 2015 Jan:8(1):. pii: e002079. doi: 10.1161/CIRCINTERVENTIONS.114.002079. Epub [PubMed PMID: 25593122]
Ribeiro HB, Webb JG, Makkar RR, Cohen MG, Kapadia SR, Kodali S, Tamburino C, Barbanti M, Chakravarty T, Jilaihawi H, Paradis JM, de Brito FS Jr, Cánovas SJ, Cheema AN, de Jaegere PP, del Valle R, Chiam PT, Moreno R, Pradas G, Ruel M, Salgado-Fernández J, Sarmento-Leite R, Toeg HD, Velianou JL, Zajarias A, Babaliaros V, Cura F, Dager AE, Manoharan G, Lerakis S, Pichard AD, Radhakrishnan S, Perin MA, Dumont E, Larose E, Pasian SG, Nombela-Franco L, Urena M, Tuzcu EM, Leon MB, Amat-Santos IJ, Leipsic J, Rodés-Cabau J. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. Journal of the American College of Cardiology. 2013 Oct 22:62(17):1552-62. doi: 10.1016/j.jacc.2013.07.040. Epub 2013 Aug 14 [PubMed PMID: 23954337]
Level 3 (low-level) evidenceDvir D, Waksman R, Barbash IM, Kodali SK, Svensson LG, Tuzcu EM, Xu K, Minha S, Alu MC, Szeto WY, Thourani VH, Makkar R, Kapadia S, Satler LF, Webb JG, Leon MB, Pichard AD. Outcomes of patients with chronic lung disease and severe aortic stenosis treated with transcatheter versus surgical aortic valve replacement or standard therapy: insights from the PARTNER trial (placement of AoRTic TraNscathetER Valve). Journal of the American College of Cardiology. 2014 Jan 28:63(3):269-79. doi: 10.1016/j.jacc.2013.09.024. Epub 2013 Oct 16 [PubMed PMID: 24140659]
Level 1 (high-level) evidenceSiontis GC, Jüni P, Pilgrim T, Stortecky S, Büllesfeld L, Meier B, Wenaweser P, Windecker S. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: a meta-analysis. Journal of the American College of Cardiology. 2014 Jul 15:64(2):129-40. doi: 10.1016/j.jacc.2014.04.033. Epub [PubMed PMID: 25011716]
Level 1 (high-level) evidenceKahlert P, Knipp SC, Schlamann M, Thielmann M, Al-Rashid F, Weber M, Johansson U, Wendt D, Jakob HG, Forsting M, Sack S, Erbel R, Eggebrecht H. Silent and apparent cerebral ischemia after percutaneous transfemoral aortic valve implantation: a diffusion-weighted magnetic resonance imaging study. Circulation. 2010 Feb 23:121(7):870-8. doi: 10.1161/CIRCULATIONAHA.109.855866. Epub [PubMed PMID: 20177005]
Webb J, Gerosa G, Lefèvre T, Leipsic J, Spence M, Thomas M, Thielmann M, Treede H, Wendler O, Walther T. Multicenter evaluation of a next-generation balloon-expandable transcatheter aortic valve. Journal of the American College of Cardiology. 2014 Dec 2:64(21):2235-43. doi: 10.1016/j.jacc.2014.09.026. Epub 2014 Nov 24 [PubMed PMID: 25456759]
Amat-Santos IJ, Dahou A, Webb J, Dvir D, Dumesnil JG, Allende R, Ribeiro HB, Urena M, Paradis JM, DeLarochellière R, Dumont E, Bergeron S, Thompson CR, Pasian S, Bilodeau S, Leipsic J, Larose E, Pibarot P, Rodés-Cabau J. Comparison of hemodynamic performance of the balloon-expandable SAPIEN 3 versus SAPIEN XT transcatheter valve. The American journal of cardiology. 2014 Oct 1:114(7):1075-82. doi: 10.1016/j.amjcard.2014.07.019. Epub 2014 Jul 17 [PubMed PMID: 25132330]
Level 1 (high-level) evidencePanchal HB, Ladia V, Amin P, Patel P, Veeranki SP, Albalbissi K, Paul T. A meta-analysis of mortality and major adverse cardiovascular and cerebrovascular events in patients undergoing transfemoral versus transapical transcatheter aortic valve implantation using edwards valve for severe aortic stenosis. The American journal of cardiology. 2014 Dec 15:114(12):1882-90. doi: 10.1016/j.amjcard.2014.09.029. Epub 2014 Sep 28 [PubMed PMID: 25438917]
Level 1 (high-level) evidenceUrena M, Webb JG, Eltchaninoff H, Muñoz-García AJ, Bouleti C, Tamburino C, Nombela-Franco L, Nietlispach F, Moris C, Ruel M, Dager AE, Serra V, Cheema AN, Amat-Santos IJ, de Brito FS, Lemos PA, Abizaid A, Sarmento-Leite R, Ribeiro HB, Dumont E, Barbanti M, Durand E, Alonso Briales JH, Himbert D, Vahanian A, Immè S, Garcia E, Maisano F, del Valle R, Benitez LM, García del Blanco B, Gutiérrez H, Perin MA, Siqueira D, Bernardi G, Philippon F, Rodés-Cabau J. Late cardiac death in patients undergoing transcatheter aortic valve replacement: incidence and predictors of advanced heart failure and sudden cardiac death. Journal of the American College of Cardiology. 2015 Feb 10:65(5):437-48. doi: 10.1016/j.jacc.2014.11.027. Epub [PubMed PMID: 25660921]