Introduction
The large intestine is the portion of the digestive tract where water is absorbed from indigestible contents. The large intestine includes the cecum, appendix, entire colon, rectum, and anal canal. It begins at the terminal ileum with the cecum. Unlike the small intestine, it has a shorter length but a much larger lumen. It is distinguished further from the small intestine by the presence of omental appendices, haustra, and teniae coli.[1][2][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The key functions of the colon include the following:
- Water and nutrient absorption
- Vitamin absorption
- Feces compaction
- Potassium and chloride secretion
- Moving waste material toward the rectum
The cecum is the proximal blind pouch of the ascending colon, lying at the level of the ileocecal junction. The terminal ileum opens into the cecum on the medial wall, and the ileocecal valve guards this opening. The appendix is a thin cylindrical organ with a blind attachment to the cecum. The base of the appendix lies on the posteromedial wall of the cecum about 1 to 2 centimeters below the ileocecal junction. The tip of the appendix frequently floats in the peritoneal cavity and is most commonly located in a retrocecal position. It has a short triangular mesentery called the mesoappendix.
The cecum is continuous with the second part of the large intestine: the ascending colon. The ascending colon runs superiorly on the right side of the abdomen from the right iliac fossa to the right lobe of the liver. At this point, it makes a left turn at the right colic flexure (hepatic flexure). Ascending colon is a retroperitoneal organ and has paracolic gutters on either side. The transverse colon is the third, most mobile, and longest part of the large intestine. It is found between the right and left colic flexures. The left colic flexure is less mobile than the right and is attached to the diaphragm through the phrenocolic ligament. The transverse colon is attached to a mesentery, the transverse mesocolon, which has its root along the inferior border of the pancreas. The transverse colon continues as the descending colon. The two are demarcated at the splenic flexure. The descending colon is a retroperitoneal organ and related to paracolic gutters on either side. It terminates into the sigmoid colon, which is the fifth part of the large intestine. The sigmoid colon links the descending colon to the rectum. The sigmoid colon is an S-shaped loop of varying length and becomes the rectum at the level of S3.
The rectum occupies the concavity of the sacrococcygeal curvature. It is fixed, primarily retroperitoneal, and subperitoneal in location. It transitions to the anal canal at the level of the puborectal sling, which is formed by the fibers of the levator ani muscles. The rectum has an expanded middle segment called the ampulla. The rectum is anteriorly related to the rectovesical pouch, prostate, bladder, urethra, and seminal vesicles in males. In females, the rectum has an anterior relationship to the recto-uterine pouch, cervix, uterus, and vagina.
Embryology
Embryologically, the colon develops from the midgut (cecum to the distal transverse colon), the hindgut (distal transverse colon to the dentate line in the anorectum), and the proctodeum (below the dentate line). Derivatives of the midgut receive blood supply from the SMA, while the IMA supplies derivatives of the hindgut.
Blood Supply and Lymphatics
The superior mesenteric artery (SMA) and the inferior mesenteric artery (IMA) provide blood supply to the colon. Communication between these two vessels happens via the marginal artery, which runs parallel to the length of the entire colon. The branches supplying specific portions of the bowel are as follows:
- The cecum is supplied by the ileocolic artery, which is a terminal branch of the SMA. The ileocolic artery gives rise to the appendicular artery to supply the appendix.
- The ascending colon and the right colic flexure are supplied by the ileocolic and right colic arteries, both branches of the SMA.
- The arterial supply to the transverse colon is mostly from the middle colic artery, which is a branch of SMA. It may also receive blood supply from the anastomotic arcades between the right and left colic arteries, which collectively form the marginal artery.
- The descending and sigmoid colon receive their blood supply from the left colic and sigmoid arteries, which are branches of the IMA. The transition of blood supply at the left colic flexure from the SMA to the IMA indicates the embryological transition from the midgut to hindgut that occurs at this point, respectively.
- The rectum and anal canal are supplied by the superior rectal artery, which is a continuation of the IMA. They also receive supply from branches of the internal iliac arteries, the middle and inferior rectal arteries. Further, the inferior rectal artery is a branch of the internal pudendal artery.[4][5]
Venous drainage usually accompanies arterial colonic supply. Ultimately, the inferior mesenteric vein (IMV) drains into the splenic vein, while the superior mesenteric vein (SMV) joins the splenic vein to form the hepatic portal vein. Lymphatics of the large intestine drain into the lymph nodes associated with the main vessels that supply them.[6]
Nerves
The midgut-derived ascending colon and proximal two-thirds of the transverse colon receive parasympathetic, sympathetic, and sensory nerve supply from the superior mesenteric plexus.
The hindgut-derived structures, which include the distal one-third of the transverse colon, descending, and sigmoid colon, receive parasympathetic, sympathetic, and sensory nerve innervation from the inferior mesenteric plexus.
Surgical Considerations
The appendix, transverse colon, and sigmoid colon are intraperitoneal organs. The cecum also is located intraperitoneally, but it lacks a mesentery. The cecum is an intraperitoneal organ, however, as it is covered on all sides by peritoneum. The ascending colon, descending colon, rectum, and anal canal are retroperitoneal structures.
Multiple surgical approaches are possible for colonic resection. These include a right hemicolectomy, extended right hemicolectomy, left hemicolectomy, extended left hemicolectomy, abdominoperineal resection. Simple excision with primary anastomosis is also an option. Side-to-side and side-to-end anastomoses are preferable to transanal anastomoses due to decreased incidence of anastomotic leakage.[7] The choice of operation depends on the location and extent of the colonic pathology. In cases where an anastomosis is not possible, an ostomy can still allow passage of stool past the skin barrier into an ostomy bag.[8][9][10]
Colonic ischemia or ischemic colitis is a dangerous complication following aortic surgery, as well as any perioperative hypotension. This condition typically presents with abdominal pain and bloody diarrhea in the post-surgical period. Care is necessary to optimize fluids in the perioperative period to prevent ischemic colitis.[11][12]
Clinical Significance
The marginal artery of Drummond is a large collateral vessel that supplies the splenic flexure of the colon and is of importance when there is occlusion of one of the major vessels supplying blood to the colon. Several disorders can affect the colon, including diverticular disease, colon cancer, bowel obstruction, lower gastrointestinal (GI) bleeding from polyps and AV malformations, strictures, and peristalsis.
Colonic perforation can be a rare cause of retroperitoneal abscess if the perforated portion of the colon is either the ascending or descending colon.[13]
Media
(Click Image to Enlarge)
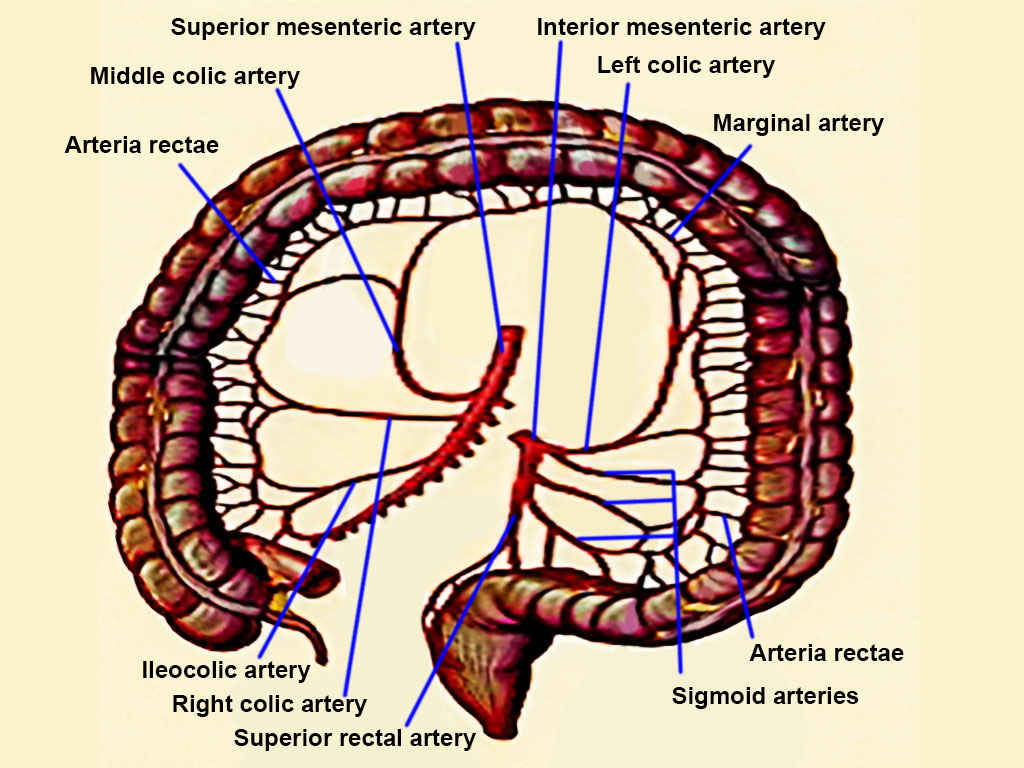
Colon Arteries. Colon arteries include superior mesenteric, inferior mesenteric, left colic, marginal, arteria rectae, sigmoid, superior rectal, right colic, ileocolic, and middle colic.
Contributed by T Silappathikaram
References
Chaudhry SR, Liman MNP, Peterson DC. Anatomy, Abdomen and Pelvis: Stomach. StatPearls. 2024 Jan:(): [PubMed PMID: 29493959]
Dumont F, Da Re C, Goéré D, Honoré C, Elias D. Options and outcome for reconstruction after extended left hemicolectomy. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2013 Jun:15(6):747-54. doi: 10.1111/codi.12136. Epub [PubMed PMID: 23398679]
Level 2 (mid-level) evidenceSmereczyński A, Kołaczyk K. Pitfalls in ultrasound imaging of the stomach and the intestines. Journal of ultrasonography. 2018:18(74):207-211. doi: 10.15557/JoU.2018.0031. Epub [PubMed PMID: 30451403]
Bruzzi M, M'harzi L, Poghosyan T, Ben Abdallah I, Papadimitriou A, Ragot E, El Batti S, Balaya V, Taieb J, Chevallier JM, Douard R. Arterial vascularization of the right colon with implications for surgery. Surgical and radiologic anatomy : SRA. 2020 Apr:42(4):429-435. doi: 10.1007/s00276-019-02359-9. Epub 2019 Oct 21 [PubMed PMID: 31637473]
GRIFFITHS JD. Surgical anatomy of the blood supply of the distal colon. Annals of the Royal College of Surgeons of England. 1956 Oct:19(4):241-56 [PubMed PMID: 13363265]
Harkins JM, Ahmad B. Anatomy, Abdomen and Pelvis, Portal Venous System (Hepatic Portal System). StatPearls. 2024 Jan:(): [PubMed PMID: 32119476]
Macina S, Imperatore M, Feleppa C, Sucameli F, Talamo G, Falco E, Berti S. Side-to-Side Anastomosis In Left Hemicolectomy, Why and When: A Single-Center Experience. Surgical technology international. 2019 May 15:34():183-186 [PubMed PMID: 30574685]
Strey CW, Wullstein C, Adamina M, Agha A, Aselmann H, Becker T, Grützmann R, Kneist W, Maak M, Mann B, Moesta KT, Runkel N, Schafmayer C, Türler A, Wedel T, Benz S. Laparoscopic right hemicolectomy with CME: standardization using the "critical view" concept. Surgical endoscopy. 2018 Dec:32(12):5021-5030. doi: 10.1007/s00464-018-6267-0. Epub 2018 Oct 15 [PubMed PMID: 30324463]
Gravante G, Elshaer M, Parker R, Mogekwu AC, Drake B, Aboelkassem A, Rahman EU, Sorge R, Alhammali T, Gardiner K, Al-Hamali S, Rashed M, Kelkar A, Agarwal R, El-Rabaa S. Extended right hemicolectomy and left hemicolectomy for colorectal cancers between the distal transverse and proximal descending colon. Annals of the Royal College of Surgeons of England. 2016 May:98(5):303-7. doi: 10.1308/rcsann.2016.0112. Epub 2016 Mar 29 [PubMed PMID: 27023638]
Tiberi A, Pesi B, Giudici F, Zambonin D, Nelli T, Cupellini C, Ficari F, Cianchi F, Scaringi S. Laparoscopic ileo-colic resection and right hemicolectomy for Crohn's disease and colon cancer: a preliminary comparative study on post-operative outcome. Updates in surgery. 2020 Sep:72(3):821-826. doi: 10.1007/s13304-020-00769-8. Epub 2020 Apr 18 [PubMed PMID: 32306278]
Level 2 (mid-level) evidenceDovzhanskiy DI, Hakimi M, Bischoff MS, Wieker CM, Hackert T, Böckler D. [Colonic ischemia after open and endovascular aortic surgery : Epidemiology, Risk Factors, Diagnosis And Therapy]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2020 Feb:91(2):169-178. doi: 10.1007/s00104-020-01113-x. Epub [PubMed PMID: 32002560]
Amini A, Nagalli S. Bowel Ischemia. StatPearls. 2024 Jan:(): [PubMed PMID: 32119414]
Ruscelli P, Renzi C, Polistena A, Sanguinetti A, Avenia N, Popivanov G, Cirocchi R, Lancia M, Gioia S, Tabola R. Clinical signs of retroperitoneal abscess from colonic perforation: Two case reports and literature review. Medicine. 2018 Nov:97(45):e13176. doi: 10.1097/MD.0000000000013176. Epub [PubMed PMID: 30407351]
Level 3 (low-level) evidence