Introduction
The following seven bones form the orbit:
- Sphenoid
- Frontal
- Zygomatic
- Ethmoid
- Lacrimal
- Maxilla
- Palatine
The orbit is a pear shape, with the optic nerve at the stem, and holds approximately 30 cc volume. The entrance to the globe anteriorly is approximately 35 mm high and 45 mm wide. The depth from orbital rim to the orbital apex measures 40 to 45 mm in adults. The maximum width is 1 cm behind the anterior orbital margin. Both race and gender can affect the measurements of the bony orbit. The orbital cavity contains the globe, nerves, vessels, lacrimal gland, extraocular muscles, tendons, and the trochlea as well as fat and other connective tissue. An increase in the volume of the extraocular structures within the orbit can cause proptosis, which is protrusion of the globe and/or displacement (deviation) of the globe from its normal position.
The orbital margin is the anterior opening of the globe and has a quadrilateral spine formed by several of the bones that make up the orbit. The roof of the orbit is formed by the orbital plate of the frontal bone and the lesser wing of the sphenoid. The fossa of the lacrimal gland lies anterolaterally, behind the zygomatic process of the frontal bone.
Walls of the Orbit
The orbital roof consists of two parts of two bones, the orbital plate frontal bone and the lesser wing of the sphenoid bone. The fossa of the lacrimal gland is in the orbital roof, and it lies anteriorly and laterally behind the zygomatic process of the frontal bone. The trochlear fossa is medial and about 4 mm from the orbital margin. This is where the pulley of the superior oblique is attached.
The medial orbital wall consists of four bones, the frontal process of the maxillary bone: the lacrimal bone, the orbital plate of the ethmoid bone, and the lesser wing of the sphenoid bone. The largest part of the medial wall is from the ethmoid bone. The frontal process of the lacrimal fossa and the bony nasolacrimal canal are continuous and extend into the inferior meatus of the nasal cavity. The medial wall of the ethmoid bone is actually very thin and is called the lamina papyracea.
The floor of the orbit consists of three bones: the maxillary bone, the palatine bone, and the orbital plate of the zygomatic bone. This part of the orbit is also the roof of the maxillary sinus. There is an infraorbital groove along the floor and it travels into a canal anteriorly where it eventually exits as the infraorbital foramen. This is the structure that lies below the orbital margin of the maxillary bone. Along the floor of the orbit is the origin of the inferior oblique muscle. This is the only extraocular muscle that does not originate at the apex of the orbit.
Lateral Orbital Wall
The lateral orbital wall is formed by two bones: the zygomatic bone and the greater wing of the sphenoid. This is the strongest of the walls of the orbit. There is a lateral orbital tubercle, which is an elevation of the orbital margin of the zygomatic bone and is an attachment for many important structures. These are the ligament of the lateral rectus muscle, the suspensory ligament of the eyeball (Lockwood ligament), lateral palpebral ligament, aponeurosis of the levator palpebrae superioris muscle, and the Whitnall ligament.
Orbital Foramina, Fissures, and Ducts
Several openings in the bones of the orbit have anatomic and clinical applications.
The optic nerve, the ophthalmic artery, and choroid plexus sympathetic fibers come from the middle cranial fossa and travel into the orbit via the optic foramen. The optic foramen passes through the lesser wing of the sphenoid bone and travels inferiorly, anteriorly, and laterally as it enters the orbit.
The supraorbital foramen is on the superior margin of the orbit and contains blood vessels and the supraorbital nerve.
The anterior ethmoidal foramen is in the frontoethmoidal suture, while the posterior ethmoidal foramen is located at the junction of the orbit's roof and medial wall. These two foramina transmit the anterior ethmoidal vessels and nerve and the posterior ethmoidal vessels and nerve, respectively.
The nasolacrimal duct drains tears from the eye into the inferior meatus of the nose.
The infraorbital canal comes from the infraorbital groove. This contains the infraorbital nerve, which is the maxillary division of CN V.
The superior orbital fissure lies between the greater and lesser wings of the sphenoid bone. Passing through the superior orbital fissure into the orbit and above the common tendinous ring are the lacrimal nerve of CN V1, the frontal nerve of CN V1, CN IV (trochlear nerve), and the superior ophthalmic vein. Passing through the superior orbital fissure and the common tendinous ring are the superior and inferior divisions of CN III (oculomotor), the nasociliary branch of CN V1, sympathetic roots of the ciliary ganglion, and CN VI (abducens).
The inferior orbital fissure lies on the floor of the orbit. The superior border is the greater wing of the sphenoid, and the maxilla and palatine bone compose the inferior border, with the zygomatic bone laterally. The zygomatic nerve and the infraorbital nerve pass through this fissure as well as some infraorbital vessels.
The infraorbital vessels then travel along the floor of the orbit and pass through infraorbital groove anteriorly.[1][2][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The bones of the orbit hold the globe and periocular structures, serve as origin points for the extraocular muscles and provide the structure for the fascial and connective tissue elements of the orbit.
Embryology
The bones of the orbit develop via both endochondral and intramembranous ossification. The sphenoid and ethmoid bones form mostly via endochondral ossification while the frontal bone is formed by intramembranous ossification.
Blood Supply and Lymphatics
The ophthalmic artery branches from the internal carotid artery and passes through the optic canal, which is inferior to the optic nerve. There is an elevation on the orbital margin of the zygomatic bone. The optic canal is formed by the sphenoid bone in the middle cranial fossa.
Nerves
The optic nerve (CN II) is the nerve responsible for relaying sight information to the brain. The optic nerve travels from the retina, which is the inside of the globe, through the optic foramen.
The ophthalmic nerve is the first division of the trigeminal nerve (CN V) and responsible for conveying sensory information from the globe, upper eyelid, lacrimal gland, conjunctiva, nasal mucosa, frontal sinus, external nose, and scalp. The ophthalmic nerve passes through the superior orbital fissure. Near this point, it divides into more specialized nerves.
The oculomotor (CN III), trochlear (CN IV), and abducent (CN VI) nerves also enter the orbit through the superior orbital fissure. The oculomotor and abducent nerves pass through the tendinous ring, while the trochlear nerve enters the orbit and passes just superior to the tendinous ring to enter the superior oblique muscle.[4][5]
Muscles
Seven extraocular muscles are associated with the bones of the orbit. All but the inferior oblique muscle originate at the orbital apex. The inferior oblique, as noted above, originates at the floor of the orbit in a depression on the orbital floor near the orbital rim. All of the rectus muscles originate at the annulus of Zinn. The superior oblique originates just medial to the optic foramen, between the annulus of Zinn and periorbita. This is the muscle that travels through the trochlea, forming a pulley that allows for intorsion of the globe. All of the extraocular muscles insert on the globe except the levator palpebrae superioris, which broadens anteriorly to become the levator aponeurosis, and is responsible primarily for eyelid elevation.[3]
Physiologic Variants
In some individuals, the supraorbital foramen is instead a supraorbital notch. There are some variations in the anatomy of the orbital bones that occur with aging. In elderly individuals, the bones can become resorbed which can cause variations in the appearance of the eye with age.[6]
Surgical Considerations
The anterior orbit is accessed either using a transcutaneous approach or a transconjunctival approach. Lid creases can be the point of entry for most cutaneous approaches. In these cases, the cornea is usually protected with an eye shield and eye lubricant.[7][8]
Clinical Significance
The bones of the orbit protect the globe of the eye as well as other periocular contents. A fracture to the orbit can involve the contents of the orbit and potentially compress nerves or muscles within the orbit.
When swelling occurs within the orbit, it can cause potential damage to the orbital contents. Intraconal lesions can cause damage to the optic nerve and associated vessels, the central retinal artery, and central retinal vein.
The abducens nerve is commonly affected when the intracranial pressure increases because its course bends sharply on the petrous part of the temporal bone.[9]
Media
(Click Image to Enlarge)
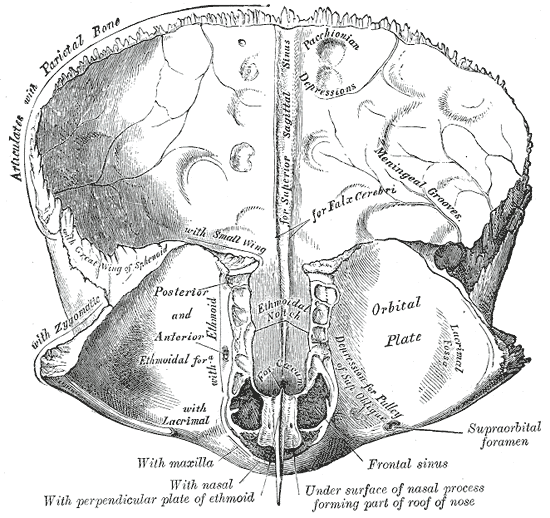
Frontal bone; Inner surface, Posterior and Anterior Ethmoidal foramen, Orbital plate
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
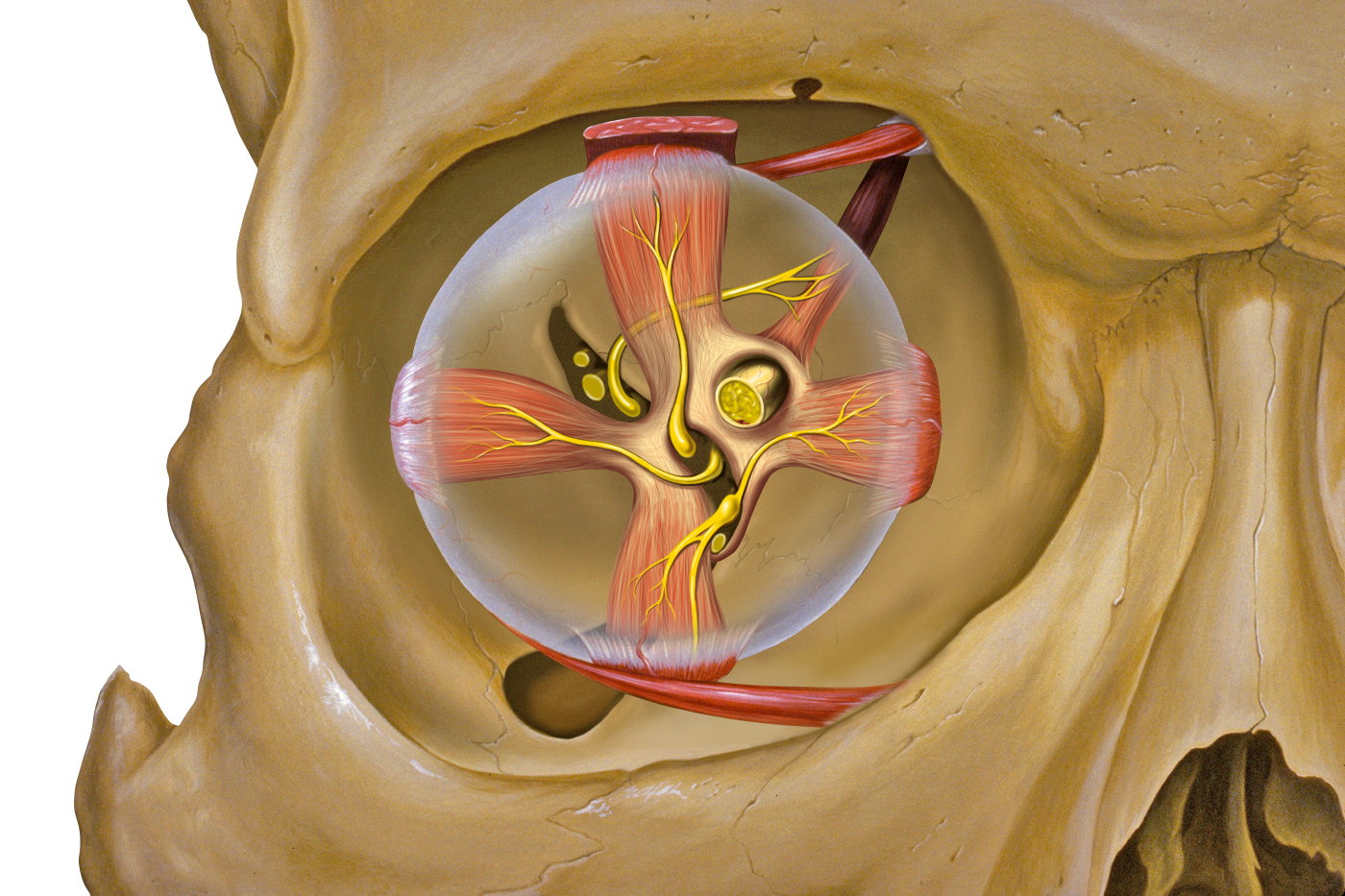
The bones of the orbit and associated extraocular muscles and nerves. Patrick J. Lynch, medical illustrator, Creative Commons Attribution 2.5 License 2006
References
Voirol JR, Vilensky JA. The normal and variant clinical anatomy of the sensory supply of the orbit. Clinical anatomy (New York, N.Y.). 2014 Mar:27(2):169-75. doi: 10.1002/ca.22328. Epub 2014 Jan 16 [PubMed PMID: 24430947]
Maslehaty H, Schultheiss S, Scholz M, Petridis AK. Surgical Anatomy of the Orbit in Human Cadavers-An Endoscopic Pictorial Documentation. Journal of neurological surgery. Part B, Skull base. 2018 Apr:79(2):173-176. doi: 10.1055/s-0037-1606294. Epub 2017 Aug 28 [PubMed PMID: 29868323]
Chastain JB, Sindwani R. Anatomy of the orbit, lacrimal apparatus, and lateral nasal wall. Otolaryngologic clinics of North America. 2006 Oct:39(5):855-64, v-vi [PubMed PMID: 16982251]
Ference EH, Smith SS, Conley D, Chandra RK. Surgical anatomy and variations of the infraorbital nerve. The Laryngoscope. 2015 Jun:125(6):1296-300. doi: 10.1002/lary.25089. Epub 2015 Jan 13 [PubMed PMID: 25992806]
Joo W, Rhoton AL Jr. Microsurgical anatomy of the trochlear nerve. Clinical anatomy (New York, N.Y.). 2015 Oct:28(7):857-64. doi: 10.1002/ca.22602. Epub 2015 Aug 28 [PubMed PMID: 26223856]
Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic plastic surgery. 2012 Aug:36(4):753-60. doi: 10.1007/s00266-012-9904-3. Epub 2012 May 12 [PubMed PMID: 22580543]
Khan AM, Varvares MA. Traditional approaches to the orbit. Otolaryngologic clinics of North America. 2006 Oct:39(5):895-909, vi [PubMed PMID: 16982253]
Turvey TA, Golden BA. Orbital anatomy for the surgeon. Oral and maxillofacial surgery clinics of North America. 2012 Nov:24(4):525-36. doi: 10.1016/j.coms.2012.08.003. Epub [PubMed PMID: 23107426]
Andrews BT, Jackson AS, Nazir N, Hromas A, Sokol JA, Thurston TE. Orbit fractures: Identifying patient factors indicating high risk for ocular and periocular injury. The Laryngoscope. 2016 Feb:126 Suppl 4():S5-11. doi: 10.1002/lary.25805. Epub 2015 Dec 22 [PubMed PMID: 26690301]