Introduction
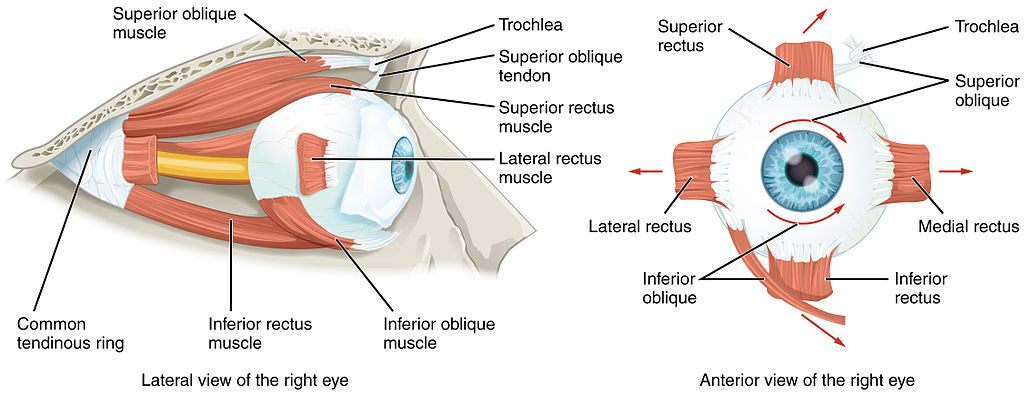
There are 7 extraocular muscles. There are 4 rectus muscles, 2 oblique muscles, and the standalone levator palpebrae superioris. The 4 rectus muscles are the medial rectus, lateral rectus, superior rectus, and inferior rectus. The oblique muscles are the superior and inferior obliques. The levator palpebrae superioris is primarily responsible for eyelid elevation (see Image. The Extraocular Muscles of the Orbit).[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
With the head facing straight and the eyes facing straight ahead, the eyes are said to be in primary gaze. From this position, an action from an extraocular muscle produces a secondary or tertiary action. Although the globe can be moved about 50 degrees from the primary position, usually during normal eye movement, only 15 degrees of extraocular muscle movement occurs before head movement begins. The rectus and oblique muscles are involved in the different gaze positions of the eye.
Each rectus and oblique muscle has a functional insertion point at the closest point where the muscle first contacts the globe. This point forms a tangential line from the globe to the muscle origin, known as the arc of contact. The common site of origin for the rectus muscles in the Annulus of Zinn is located at the orbital apex. The levator palpebrae superioris does not contact the globe directly but elevates the eyelid.[1]
Embryology
The mesenchyme of the head, including the orbit and its structures, are primarily embryologic derivatives of mesoderm and neural crest cells. The extraocular muscles originate from the mesoderm, but the satellite and connective tissue of the muscle arise from neural crest cells. Most of the orbit's remaining connective tissue is also derived from neural crest cells.[2][3]
Blood Supply and Lymphatics
The primary blood supply for the extraocular muscles is the muscular branches of the ophthalmic artery, the lacrimal artery, and the infraorbital artery. The ophthalmic artery has 2 muscular branches, which are the superior and inferior muscular branches. The lateral rectus receives blood from a branch of the lacrimal artery, and the other rectus muscles receive blood via 2 anterior ciliary arteries that communicate with a structure called the anterior circle of the ciliary body.
Venous drainage is similar to the arterial system and empties into the superior and inferior orbital veins. Usually, there are a total of 4 vortex veins, and these are found at the lateral and medial sides of the superior and inferior rectus muscles. These vortex veins drain into the orbital venous system.[4]
Nerves
Cranial nerve III is divided into upper and lower divisions, with the upper division innervating the superior rectus and the levator palpebrae superioris and the lower division innervating the medial rectus, inferior rectus, and inferior oblique. The superior oblique is innervated by cranial nerve IV (trochlear), while the lateral rectus is innervated by cranial nerve VI (abducens).[5]
Muscles
Each rectus muscle originates posteriorly at the Annulus of Zinn and courses anteriorly along the orbital walls until it reaches its insertion point. These muscles are inserted on the globe at varying distances from the limbus, and the curved line drawn along the insertion points makes a spiral known as the spiral of Tillaux. Starting at the medial aspect of the globe, the medial rectus inserts at 5.5 mm from the limbus, the inferior rectus inserts at 6.5 mm from the limbus, the lateral rectus inserts at 6.9 mm from the limbus, and the superior rectus at 7.7 mm from the limbus.
The superior oblique originates medial to the optic foramen and travels through the trochlea, a pulley at the superonasal portion of the orbital rim. From here, the muscle travels under the superior rectus and inserts slightly posterior to the insertion of the superior rectus. The inferior oblique originates from a depression on the orbital floor near the orbital rim, travels posteriorly and inferiorly, and inserts near the macula.
The levator palpebrae superioris originates from the lesser wing of the sphenoid and courses anteriorly. The body of the muscle travels over the superior rectus toward the eyelid. The Whitnall ligament is formed where the connective tissue from the levator palpebrae superioris connects with similar tissue from the superior rectus. Near this ligament, the levator palpebrae superioris fibers change to become more vertical, and they divide to the aponeurosis anteriorly and the superior tarsal muscle superiorly.[1]
Extraocular muscles have a large ratio of nerve fibers to skeletal muscle fibers. The ratio is 1:3 to 1:5 compared to other skeletal muscles, which are 1:50 to 1:125. Extraocular muscles are a specialized skeletal muscle form with various fiber types, including slow tonic types, which resist fatigue, and saccadic (rapid) muscle fibers.[6][7]
Physiologic Variants
The size of the extraocular muscles and their insertion point on the globe from the limbus and other anatomical measurements may vary widely from one individual to the next. The numbers described in this article reflect average distances.
Occasionally, accessory extraocular muscles originating from the Annulus of Zinn and inserted in various locations have been reported. Both supernumerary and accessory extraocular muscles have been reported.
Congenital differences in extraocular muscles can cause ocular misalignment. See the Clinical Significance section for more details regarding strabismus.[1][8]
Surgical Considerations
The nerves to the rectus muscles and superior oblique muscles insert into the muscles at one-third the distance from the origin to the insertion. This makes damage to these nerves during anterior segment surgery difficult but not impossible. Additionally, instruments that are advanced 26 mm posterior to the rectus muscle insertions can cause injury to the nerve.[9]
Blood vessels may be compromised during surgery of the inferior rectus muscle. The vessels that supply blood to the extraocular muscles also supply nearly all the temporal half of the anterior segment of the eye. Most of the nasal half of the anterior segment circulation is also derived from blood vessels that supply the extraocular muscles. Therefore, care must be taken during surgery of the medial rectus or other extraocular muscles to avoid disrupting this blood supply.[4][10]
Other complications may result from strabismus surgery. Unsatisfactory alignment is the most common complication; additional surgery may be required to correct this. Refractive changes may occur when 2 rectus muscles of 1 eye are operated on, which may resolve over months. Other possible surgical complications include diplopia, perforation of the sclera, and postoperative infections. Although uncommon, serious infections may result after strabismus surgery, including pre-septal or orbital cellulitis and endophthalmitis.[11][12][13]
Clinical Significance
The function of the extraocular muscles can be assessed along with the other extraocular muscles during the clinical exam. The movement of the extraocular muscles can be assessed by having a patient look in 9 directions. Starting with the primary gaze, followed by the secondary positions (up, down, left, and right) and the tertiary positions (up and right, up and left, down and right, down and left). The clinician can test these positions by having the patient follow the clinician's finger and trace a wide letter "H" in the air.
Several methods can be used to further test ocular alignment, including cover-uncover tests, corneal light reflex tests, dissimilar image tests, and dissimilar target tests. Since many patients with extraocular muscle abnormalities are young children, the clinician may need to employ various clever means, such as using toys or other objects to elicit the child's cooperation.
Strabismus, or ocular misalignment, can be caused by abnormalities in binocular vision or abnormalities of neuromuscular control. Weakness, injury, or paralysis of the inferior rectus muscle can also cause strabismus.
Nerve palsies of the cranial nerves, which innervate the extraocular muscles, produce characteristic patterns that must be identified by the clinician.[14][15]
Other Issues
There is a capsule of connective tissue known as the Tenon capsule, an envelope that fuses with the optic sheath posteriorly and meets the intermuscular septum anteriorly. The Tenon capsule helps the globe to stay positioned in orbit along with the extraocular muscles.[16]
Media
(Click Image to Enlarge)
References
Haładaj R, Wysiadecki G, Polguj M, Topol M. Bilateral muscular slips between superior and inferior rectus muscles: case report with discussion on classification of accessory rectus muscles within the orbit. Surgical and radiologic anatomy : SRA. 2018 Jul:40(7):855-862. doi: 10.1007/s00276-018-1976-6. Epub 2018 Jan 24 [PubMed PMID: 29368252]
Level 3 (low-level) evidenceZiermann JM, Diogo R, Noden DM. Neural crest and the patterning of vertebrate craniofacial muscles. Genesis (New York, N.Y. : 2000). 2018 Jun:56(6-7):e23097. doi: 10.1002/dvg.23097. Epub 2018 Apr 16 [PubMed PMID: 29659153]
Tzahor E. Head muscle development. Results and problems in cell differentiation. 2015:56():123-42. doi: 10.1007/978-3-662-44608-9_6. Epub [PubMed PMID: 25344669]
Level 3 (low-level) evidenceTibrewal S, Kekunnaya R. Risk of Anterior Segment Ischemia Following Simultaneous Three Rectus Muscle Surgery: Results from a Single Tertiary Care Centre. Strabismus. 2018 Jun:26(2):77-83. doi: 10.1080/09273972.2018.1450429. Epub 2018 Mar 16 [PubMed PMID: 29547011]
Tsutsumi S, Nakamura M, Tabuchi T, Yasumoto Y, Ito M. An anatomic study of the inferior oblique nerve with high-resolution magnetic resonance imaging. Surgical and radiologic anatomy : SRA. 2013 Jul:35(5):377-83. doi: 10.1007/s00276-012-1040-x. Epub 2012 Nov 6 [PubMed PMID: 23129266]
Demer JL. Compartmentalization of extraocular muscle function. Eye (London, England). 2015 Feb:29(2):157-62. doi: 10.1038/eye.2014.246. Epub 2014 Oct 24 [PubMed PMID: 25341434]
Level 3 (low-level) evidenceJanbaz AH, Lindström M, Liu JX, Pedrosa Domellöf F. Intermediate filaments in the human extraocular muscles. Investigative ophthalmology & visual science. 2014 Jul 15:55(8):5151-9. doi: 10.1167/iovs.14-14316. Epub 2014 Jul 15 [PubMed PMID: 25028355]
Kakizaki H, Zako M, Nakano T, Asamoto K, Miyaishi O, Iwaki M. An anomalous muscle linking superior and inferior rectus muscles in the orbit. Anatomical science international. 2006 Sep:81(3):197-9 [PubMed PMID: 16955671]
Level 3 (low-level) evidenceNonaka Y, Fukushima T, Friedman AH, Kolb LE, Bulsara KR. Surgical management of nonvascular lesions around the oculomotor nerve. World neurosurgery. 2014 May-Jun:81(5-6):798-809. doi: 10.1016/j.wneu.2012.11.067. Epub 2012 Nov 24 [PubMed PMID: 23182737]
Level 3 (low-level) evidencePineles SL, Chang MY, Oltra EL, Pihlblad MS, Davila-Gonzalez JP, Sauer TC, Velez FG. Anterior segment ischemia: etiology, assessment, and management. Eye (London, England). 2018 Feb:32(2):173-178. doi: 10.1038/eye.2017.248. Epub 2017 Nov 17 [PubMed PMID: 29148529]
Patel SB, Reddy N, Hogan RN, Cao JH. A Case of Endophthalmitis After Bilateral Medial Rectus Recession. Journal of pediatric ophthalmology and strabismus. 2017 Jun 29:54():e37-e41. doi: 10.3928/01913913-20170531-07. Epub 2017 Jun 29 [PubMed PMID: 28665442]
Level 3 (low-level) evidenceSubretinal abscess after strabismus surgery: case report and literature review., Patel CC,Goldenberg DT,Trese MT,Walsh MK,OʼMalley ER,, Retinal cases & brief reports, 2011 Winter [PubMed PMID: 25389671]
Level 3 (low-level) evidenceDhrami-Gavazi E, Lee W, Garg A, Garibaldi DC, Leibert M, Kazim M. Bilateral Orbital Abscesses After Strabismus Surgery. Ophthalmic plastic and reconstructive surgery. 2015 Nov-Dec:31(6):e141-2. doi: 10.1097/IOP.0000000000000182. Epub [PubMed PMID: 24896771]
Level 3 (low-level) evidenceNottingham Chaplin PK, Baldonado K, Cotter S, Moore B, Bradford GE. An Eye on Vision: Five Questions About Vision Screening and Eye Health-Part 2. NASN school nurse (Print). 2018 Jul:33(4):210-213. doi: 10.1177/1942602X18779801. Epub 2018 Jun 8 [PubMed PMID: 29883269]
Nottingham Chaplin PK, Baldonado K, Bradford GE, Cotter S, Moore B. An Eye on Vision: Five Questions About Vision Screening and Eye Health. NASN school nurse (Print). 2018 May:33(3):146-149. doi: 10.1177/1942602X18765210. Epub [PubMed PMID: 29658851]
Pivotal role of orbital connective tissues in binocular alignment and strabismus: the Friedenwald lecture., Demer JL,, Investigative ophthalmology & visual science, 2004 Mar [PubMed PMID: 14985282]