
 Anatomy, Bony Pelvis and Lower Limb, Foot Muscles
Anatomy, Bony Pelvis and Lower Limb, Foot Muscles
Introduction
There are 29 muscles associated with the human foot: 10 originate outside the foot but cross the ankle joint to act on the foot, and 19 are intrinsic foot muscles. The foot is crucial to human locomotion and postural stability, and the muscles associated with the foot are therefore involved principally in this function. The muscles are aided by the plantar fascia, shaping the posture, shape, and strength of the foot and providing the ability to transmit muscle tension not only toward the ground but also toward the whole body system.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Compartments of the Foot
The foot muscles are divided into nine compartments encompassed by fascia, although past studies on the exact divisions of the foot have varied considerably.[1][2]
The medial compartment contains the abductor hallucis, flexor hallicus brevis, and flexor hallucis longus tendon. The lateral compartment contains the abductor digiti minimi and the flexor digiti minimi. The superficial central compartment contains the flexor digitorum brevis, the four lumbricals, and the flexor digitorum longus tendons. The deep central (calcaneal) compartment, which communicates with the deep posterior compartment of the lower leg, contains the quadratus plantae and the posterior tibial neurovascular bundle. The adductor compartment contains the adductor hallucis muscle.
There are four interosseous compartments; the first is between the first and second metatarsals and includes the first dorsal interosseous muscle. The second is between the second and third metatarsal and includes both the dorsal and plantar interosseous muscles. The two compartments between the third and fourth, as well as the fourth and fifth metatarsals, also include the dorsal and plantar interosseous muscles.[3][4][5][6]
The muscles are perhaps more easily described as either extrinsic (originating outside the foot) or intrinsic (originating within the foot).[7][8][9] The intrinsic muscles of the foot are further divided into dorsal and plantar groups, and there are four layers of the plantar muscles.
Extrinsic Muscles of the Foot
Peroneus Longus
- The peroneus longus is one of the three muscles that span the lateral leg - peroneus may also be interchanged with fibular, referring to the lateral bone of the lower leg running deep to the peroneal muscles.
- Origin: The peroneus longus muscle originates on the head of the fibula and the upper half of the fibular shaft. This muscle crosses the ankle joint, courses deep into the foot, and passes into a groove of the cuboid bone.
- Insertion: The peroneus longus muscle inserts on the posterolateral aspect of the medial cuneiform bone and the lateral portion of the base of the first metatarsal.
- Action: The peroneus longus acts to evert the foot, plantarflex the ankle, and add support to the transverse arch of the foot.
- Blood Supply: Anterior tibial artery
- Innervation: Superficial peroneal nerve
Peroneus Brevis
- The peroneus brevis is another of the three muscles spanning the lateral leg and may also be called fibularis brevis, referring to the fibula.
- Origin: The peroneus brevis originates on the inferior two-thirds of the lateral fibula and ultimately courses posteriorly to the lateral malleolus of the fibula.
- Insertion: The peroneus brevis inserts on the styloid process of the fifth metatarsal.
- Action: The primary action of the peroneus brevis is eversion of the foot and plantarflexion of the ankle.
- Blood Supply: Peroneal artery
- Innervation: Superficial peroneal nerve
Peroneus Tertius
- The peroneus tertius is the third and final muscle of the lateral peroneus or fibular muscles.
- Origin: The peroneus tertius originates from the middle fibular shaft.
- Insertion: The peroneus tertius inserts on the dorsal surface of the fifth metatarsal.
- Action: The primary action of the peroneus tertius is dorsiflexion, eversion, and abduction of the foot.
- Blood Supply: Anterior tibial artery
- Innervation: Deep peroneal nerve
Anterior Tibialis
- The anterior tibialis is the most prominent muscle in the anterior leg and is often visible during dorsiflexion of the foot.
- Origin: The anterior tibialis originates from the lateral condyle of the tibia and the proximal half to two-thirds of the tibial shaft.
- Insertion: Insertion of the anterior tibialis occurs after passing under the extensor retinaculum and is on the medial and plantar surfaces of the medial cuneiform and base of the first metatarsal.
- Action: The primary action of the anterior tibialis is dorsiflexion of the ankle and inversion of the hindfoot.
- Blood Supply: Anterior tibial artery
- Innervation: Deep peroneal nerve
Posterior Tibialis
- Origin: The posterior tibialis originates from the superior two-thirds of the medial posterior surface of the tibia.
- Insertion: The tendon of the posterior tibialis courses distally, bifurcating at the calcaneonavicular ligament, to insert on the tuberosity of the navicular bone (superficial slip) and the plantar surfaces of the second, third, and fourth metatarsals (deep slip).
- Action: The posterior tibialis is the primary inverter of the foot but also adducts, plantar flexes, and aids in supination of the foot.
- Blood Supply: Sural, peroneal, and posterior tibial arteries
- Innervation: Tibial nerve
Extensor Digitorum Longus
- Origin: The extensor digitorum longus originates from the lateral tibial condyle and continues distally to split into four tendons after the level of the extensor retinaculum.
- Insertion: The tendons insert on the dorsum of the middle and distal phalanges.
- Action: The primary action of the extensor digitorum longus is extension of the second through fifth digits; the muscle assists with dorsiflexion of the ankle.
- Blood Supply: Anterior tibial artery
- Innervation: Deep peroneal nerve
Flexor Digitorum Longus
- Origin: The flexor digitorum longus originates from the posterior surface of the tibia distal to the soleal line.
- Insertion: The muscle continues distally to split into four individual tendons, which insert on the plantar surfaces of the bases of the second through fifth distal phalanges.
- Action: The primary action is flexion of digits two through five; the muscle may aid in plantar flexion of the ankle.
- Blood Supply: Posterior tibial artery
- Innervation: Tibial nerve
Flexor Hallucis Longus
- Origin: The flexor hallucis longus originates from the inferior two-thirds of the posterior fibula.
- Insertion: The muscles insert on the plantar surface of the base of the distal phalanx of the great toe.
- Action: The primary action of the muscle is flexion of the great toe, but it may minimally supinate and plantarflex the ankle.
- Blood Supply: Peroneal and posterior tibial artery
- Innervation: Tibial nerve
Gastrocnemius
- The gastrocnemius is the most superficial calf muscle.
- Origin: The gastrocnemius muscle has two heads, one of which originates from each femoral condyle.
- Insertion: The gastrocnemius merges with the soleus to form the thick Achilles tendon, which inserts on the calcaneus.
- Action: The action of the gastrocnemius is plantarflexion of the ankle.
- Blood Supply: Sural branch of the popliteal artery
- Innervation: Tibial nerve
Soleus
- The soleus is the deep muscle of the posterior leg and makes up the bulk of the calf.
- Origin: The soleus originates from the upper quarter of the posterior fibula and the middle third of the posterior tibial shaft.
- Insertion: The soleus eventually joins the gastrocnemius to become the Achilles tendon and inserts into the calcaneus.
- Action: The action of the soleus is plantarflexion of the ankle.
- Blood Supply: Posterior tibial, peroneal, and sural arteries
- Innervation: Tibial nerve
Dorsal intrinsic Muscles of the Foot
Extensor Digitorum Brevis
- Origin: The extensor digitorum brevis originates from the dorsal surface of the calcaneus.
- Insertion: The muscles insert on the base of the proximal phalanx of digits two through four.
- Action: The extensor digitorum brevis acts to extend the second, third, and fourth digits.
- Blood Supply: Dorsalis pedis
- Innervation: Deep peroneal nerve
Dorsal Interosseous
- The three dorsal interossei muscles exist between digits two through five - the two adjacent muscles form a central tendon and act to abduct the metatarsal-phalangeal joints. Innervation comes from the lateral plantar nerve.
Extensor Hallucis Brevis
- Origin: The extensor hallucis brevis originates from the dorsal surface of the calcaneus.
- Insertion: The muscle inserts at the base of the proximal phalanx of the great toe.
- Action: The extensor hallicus brevis extends the great toe.
- Blood Supply: Dorsalis pedis
- Innervation: Deep peroneal nerve
Plantar intrinsic Muscles of the Foot
1st Layer
Abductor Hallucis
- Origin: Calcaneal tuberosity
- Insertion: Base of the great toe and the proximal phalanx
- Action: Abduction of the great toe
- Blood Supply: Medial plantar artery
- Innervation: Medial plantar nerve
Flexor Digitorum Brevis
- Origin: Calcaneal tuberosity
- Insertion: The middle phalanx of digits two through five
- Action: Flexion of the second through fifth digits
- Blood Supply: Medial plantar artery
- Innervation: Medial plantar nerve
Abductor Digiti Minimi
- Origin: Calcaneal tuberosity
- Insertion: Base of the fifth metatarsal
- Action: Abduction of the fifth digit
- Blood Supply: Lateral plantar artery
- Innervation: Lateral plantar nerve
2nd Layer
Quadratus Plantae
- Origin: Plantar surface of the calcaneus
- Insertion: Flexor digitorum longus tendon
- Action: Aids in flexion of the distal phalanges
- Blood Supply: Lateral plantar artery
- Innervation: Lateral plantar nerve
Lumbricals
- There are four muscles referred to as lumbricals in the foot.
- Origin: Flexor digitorum longus tendon
- Insertion: Extensor digitorum longus tendon
- Action: Flexion of the metatarsophalangeal joints and extension of the interphalangeal joints
- Blood Supply: Medial and lateral plantar arteries
- Innervation: Medial and lateral plantar nerve
3rd Layer
Flexor Hallucis Brevis
- Origin: The cuboid and the lateral cuneiform
- Insertion: Proximal phalanx of the great toe, by two tendons at the medial and lateral surfaces
- Action: Flexion of the great toe
- Blood Supply: Medial plantar artery
- Innervation: Medial plantar nerve
Oblique and Transverse Head of Adductor Hallucis
- The adductor hallucis has two heads, an oblique hea, and a transverse head.
- Origin: The oblique head originates at the proximal ends of the metatarsals two through four, and the transverse head originates via MTP ligaments of digits three through five
- Insertion: inserts at the proximal phalanx of the great toe
- Action: The primary action is to adduction of the great toe
- Blood Supply: First plantar metatarsal artery
- Innervation: Deep branch of lateral plantar
Flexor Digiti Minimi Brevis
- Origin: Base of the fifth metatarsal
- Insertion: Proximal phalanx of the fifth metatarsal
- Action: The primary action is flexion of the fifth digit
- Blood Supply: Lateral Plantar artery
- Innervation: Lateral plantar nerve
4th Layer
Plantar Interosseous
- The are three plantar interossei
- Origin: Medial aspect of the individual metatarsals of digits three through five
- Insertion: The proximal phalanges of digits three through five
- Action: The primary action of the plantar interossei is adduction and abduction of the digits. They also assist the lumbricals in the extension of the interphalangeal joints.
- Blood Supply: Plantar metatarsal artery
- Innervation: Lateral plantar nerve
Embryology
During gestation, the limbs appear at the fourth post-ovulatory week, approximately embryonic stage 13 (3 to 6 mm long).[10] Each limb develops in a proximal to distal direction, and the foot appears at about 4.5 weeks (embryonic stage 15). The cartilaginous skeleton and the muscles become visible in a few days, and soon after, the fingers can be observed (embryonic stage 18 to 19). The skeletal elements first appear as mesodermal condensations, which then condense in a definite order; ossification occurs in the form of a periosteal collar in the tubular bones. Vascular invasion of the tarsal bones occurs during the fetal period, while endochondral ossification does not begin in some tarsal bones until after birth.
The limbs develop from the proliferation of the mesoderm of the somatopleure in the lateral region of the body, which forms outgrowths in correspondence with the lumbar tract (third through fifth lumbar somites) for the hind limbs.[11]
Blood Supply and Lymphatics
The blood supply to the foot begins primarily with the popliteal artery. The popliteal artery branches off the large superficial femoral artery, giving rise to the three main branches supplying the lower leg and foot. The three branches from proximal to distal are the anterior tibial artery, peroneal artery, and posterior tibial artery. The anterior tibial artery continues distally to supply the anterior and dorsal portions of the foot. Once the anterior tibial artery passes under the extensor retinaculum, it becomes the dorsalis pedis. This artery is commonly palpated for a pedal pulse. The dorsalis pedis continues under the extensor hallucis longus and passes between it and the extensor digitorum longus.
The dorsalis pedis has three lateral branches: the proximal and distal tarsal arteries and the arcuate artery. The two medial branches of the dorsalis pedis are the medial tarsal arteries. The arcuate artery branches at the level of the first tarsal-metatarsal joint and courses over metatarsals two through four to give rise to the second, third, and fourth dorsal metatarsal arteries. The first dorsal metatarsal artery branches directly off the dorsalis pedis. The metatarsal branches supply the dorsal interosseous muscles of the foot. The peroneal artery supplies the lateral leg muscles and the posterior foot. Finally, the posterior tibial artery supplies the posterior and lateral leg as well as the plantar surface of the foot.[5]
The venous system of the lower limbs is composed of deep veins (which run between the muscles) and superficial veins (which constitute a complex network just below the skin). The two systems are joined by transfascial valved communications that constitute a real system, that of the perforating veins. The perforating veins favor the outflow of blood that flows in the system superficially (about 10%) towards the deep system.
In the sole, there is a sort of sponge consisting of a complicated intertwining of superficial and deep veins, which, at each step, are emptied by compression on the ground. Thanks to this mechanism, the blood is pushed over the ankle up to the calf.
The venous system originates in the microcirculation from the arterial capillaries (afferent branch) to continue with the venous capillaries that converge first in the collecting venules and then in the collecting veins, thus constituting the initial efferent branch of venous macrocirculation.
In the anterior region, the dorsal venous network of the foot through the intercapitular veins that pass through the interdigital spaces; the digital veins, joining two to two in the interdigital spaces, originate the metatarsal veins that are directed in the deep plantar venous arch, converging in the lateral plantar veins; these, after joining posteriorly with the medial plantar veins, originate the two posterior tibial veins. The anterior tibialis originates from the deep veins of the dorsal region of the foot. The medial marginal vein of the foot ascending anterior to the medial malleolus forms the internal or great saphenous vein. The lateral marginal vein of the foot ascending anterior to the lateral malleolus forms the small saphenous vein.
The lymph drained from the lower extremities begins in the foot, where lymph nodes are divided into superficial (epifascial) and deep (subfascial) nodes; the epifascial and subfascial nodal networks are connected by anastomoses. In general, the epifascial system drains the skin and subcutaneous tissues, whereas the subfascial system directly drains the joints, muscles, and bones.[12] The most significant portion of epifascial collectors forms a ventromedial bundle over the dorsum of the foot, which then drains to the superficial inguinal nodes; a smaller dorsal bundle drains first into the popliteal nodes.[13] The subfascial nodes drain into the deep inguinal nodes.
Nerves
The sciatic nerve is the initial nerve that gives rise to most of the innervation of the lower extremity. The sciatic nerve makes its way out of the lumbosacral plexus and passes under the piriformis muscle before traveling distally. Around the distal third of the femur, the sciatic nerve branches and gives rise to the common fibular and tibial nerve. The tibial nerve continues distally to give rise to the medial calcaneal branches, the medial sural cutaneous nerve, and the medial and lateral plantar nerves. The common peroneal nerve gives rise to two main branches, the superficial and deep peroneal nerves. The superficial peroneal nerve primarily gives rise to cutaneous branches that receive sensory information from the skin. The deep peroneal nerve supplies motor function to many of the muscles responsible for the dorsiflexion of the foot.[14][15]
Physiologic Variants
Tibialis Anterior Tendon
Recent studies have shown variability in the insertion of the tibialis anterior tendon. This may be of clinical significance because different insertion points may cause redistributions of force on the foot and ankle. These differences become significant during anterior tibialis tendon ruptures when it may be necessary for biomechanics to match up the previous tendon type.[7]
Accessory Peroneal Muscles
Peroneus quartus is an accessory muscle found in 6 to 22% of people, depending on the study. It typically arises from the peroneus brevis muscle; origins from the peroneus tertius and longus muscles are described. This muscle has been found to have different insertions, including the cuboid, the lateral tubercle of the calcaneus, the apophysis of the cochlea of the calcaneus, or the retrotrochlear eminence of the calcaneus. In some instances, this muscle belly will give rise to a tendon that inserts on a phalanx of the fifth digit, thus earning the name peroneus digiti quinti. If present, the peroneus digiti quinti may help to extend the fifth digit.[16]
Several studies have shown the association between the presence of a peroneus quartus muscle and associated pathology. Symptomatology in the form of ankle pain in the absence of trauma to the lateral ankle is common. Other pathology noted includes peroneal subluxation, tendinous calcification, and hypertrophy of the retrotrochlear eminence of the calcaneus, causing pain.[17]
Clinical Significance
The muscles acting directly on or around the foot are responsible for many actions that allow for normal gait and posture. Injuries to these muscles can result in many conditions that may interfere with the ability to complete activities of daily living. Achilles tendon rupture, hammer toe, and pes planus (flat foot) are common conditions associated with the foot muscles. Each of these affects patients differently and may come with other comorbidities. Treatment of these conditions varies based on severity and the age of the patient. Conservative non-operative management of Achilles tendon rupture, for example, has shown to be non-inferior to operative management in older patients.[18]
Media
(Click Image to Enlarge)
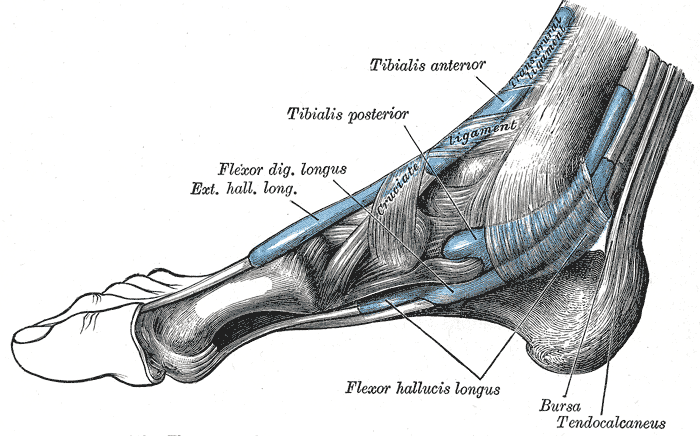
Extrinsic Foot Muscles. This medial view of the right foot shows the tendons of the tibialis anterior, tibialis posterior, flexor digitorum longus, extensor hallucis longus, and flexor hallucis longus. The retrocalcaneal bursa, tendo calcaneus (Achilles tendon), and transcrural and cruciate ligaments are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
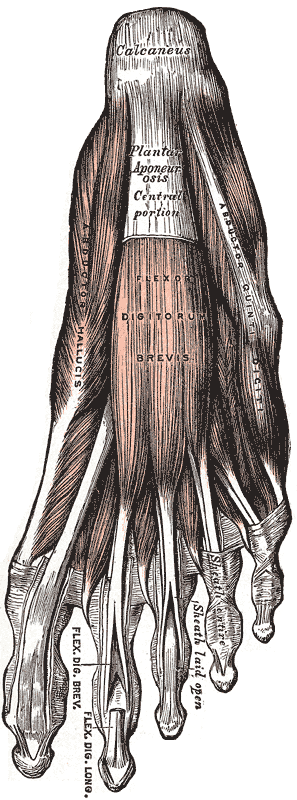
Muscles and Fascia of the Foot, Calcaneus, Plantar Aponeurosis Central portion, Abductor Quinti Digiti, Abductor Hallucis, Flexor Digitorum Brevis, Flexor Digiti Brevis and Longus
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)

Muscles of the Foot; Dorsal View, Tibialis Posterior, Long Plantar Ligament, Sheath of Peroneus Longus, Flexor Hallucis Brevis, Adductor Hallucis, Adductor Hallucis, Flexor Digiti Quinti Brevis
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
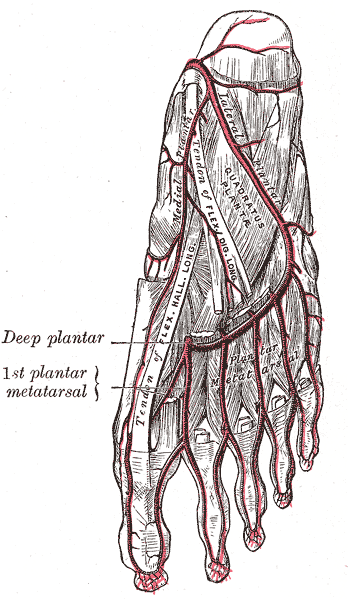
Arteries for the Bottom of the foot; Lateral and Medial Plantar Artery, Plantar Metatarsal artery
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
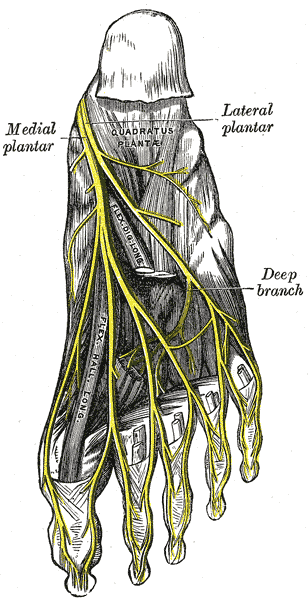
The Sacral and Coccygeal Nerves, The Plantar Nerves, Medial; Lateral Plantar, Deep Branch
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Ling ZX, Kumar VP. The myofascial compartments of the foot: a cadaver study. The Journal of bone and joint surgery. British volume. 2008 Aug:90(8):1114-8. doi: 10.1302/0301-620X.90B8.20836. Epub [PubMed PMID: 18669973]
Level 3 (low-level) evidenceReach JS Jr, Amrami KK, Felmlee JP, Stanley DW, Alcorn JM, Turner NS. The compartments of the foot: a 3-tesla magnetic resonance imaging study with clinical correlates for needle pressure testing. Foot & ankle international. 2007 May:28(5):584-94 [PubMed PMID: 17559766]
Faymonville C, Andermahr J, Seidel U, Müller LP, Skouras E, Eysel P, Stein G. Compartments of the foot: topographic anatomy. Surgical and radiologic anatomy : SRA. 2012 Dec:34(10):929-33. doi: 10.1007/s00276-012-0982-3. Epub 2012 May 26 [PubMed PMID: 22638720]
Orbay H, Kerem M, Unlü RE, Esmer AF, Cömert A, Tüccar E, Sensöz O. Vascular anatomy of plantar muscles. Annals of plastic surgery. 2007 Apr:58(4):420-6 [PubMed PMID: 17413886]
Alagoz MS, Orbay H, Uysal AC, Comert A, Tuccar E. Vascular anatomy of the metatarsal bones and the interosseous muscles of the foot. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2009 Sep:62(9):1227-32. doi: 10.1016/j.bjps.2007.12.083. Epub 2008 Jun 20 [PubMed PMID: 18572002]
Kalin PJ, Hirsch BE. The origins and function of the interosseous muscles of the foot. Journal of anatomy. 1987 Jun:152():83-91 [PubMed PMID: 3654378]
Olewnik Ł, Podgórski M, Polguj M, Topol M. A cadaveric and sonographic study of the morphology of the tibialis anterior tendon - a proposal for a new classification. Journal of foot and ankle research. 2019:12():9. doi: 10.1186/s13047-019-0319-0. Epub 2019 Feb 1 [PubMed PMID: 30733832]
Amis AA, de Leeuw PA, van Dijk CN. Surgical anatomy of the foot and ankle. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2010 May:18(5):555-6. doi: 10.1007/s00167-010-1107-3. Epub [PubMed PMID: 20306016]
Chiou-Tan F, Furr-Stimming E, John J, Harrell JS, Zhang H, Taber KH. Procedure-oriented sectional anatomy of the foot. Journal of computer assisted tomography. 2015 Jan-Feb:39(1):140-2. doi: 10.1097/RCT.0000000000000165. Epub [PubMed PMID: 25279850]
Level 2 (mid-level) evidenceO'Rahilly R, Müller F. Developmental stages in human embryos: revised and new measurements. Cells, tissues, organs. 2010:192(2):73-84. doi: 10.1159/000289817. Epub 2010 Feb 26 [PubMed PMID: 20185898]
Jeanty P, Cousaert E, Cantraine F, Hobbins JC, Tack B, Struyven J. A longitudinal study of fetal limb growth. American journal of perinatology. 1984 Jan:1(2):136-44 [PubMed PMID: 6335042]
Level 2 (mid-level) evidenceJensen MR, Simonsen L, Karlsmark T, Bülow J. Lymphoedema of the lower extremities--background, pathophysiology and diagnostic considerations. Clinical physiology and functional imaging. 2010 Nov:30(6):389-98. doi: 10.1111/j.1475-097X.2010.00969.x. Epub 2010 Aug 16 [PubMed PMID: 20718809]
Schacht V, Luedemann W, Abels C, Berens von Rautenfeld D. Anatomy of the subcutaneous lymph vascular network of the human leg in relation to the great saphenous vein. Anatomical record (Hoboken, N.J. : 2007). 2009 Jan:292(1):87-93. doi: 10.1002/ar.20765. Epub [PubMed PMID: 18951505]
Yablon CM, Hammer MR, Morag Y, Brandon CJ, Fessell DP, Jacobson JA. US of the Peripheral Nerves of the Lower Extremity: A Landmark Approach. Radiographics : a review publication of the Radiological Society of North America, Inc. 2016 Mar-Apr:36(2):464-78. doi: 10.1148/rg.2016150120. Epub 2016 Feb 12 [PubMed PMID: 26871986]
Taber KH, Duncan G, Chiou-Tan F, Patni P, Hayman LA. Sectional neuroanatomy of the lower limb II: leg and foot. Journal of computer assisted tomography. 2001 Sep-Oct:25(5):823-6 [PubMed PMID: 11584247]
Yammine K. The accessory peroneal (fibular) muscles: peroneus quartus and peroneus digiti quinti. A systematic review and meta-analysis. Surgical and radiologic anatomy : SRA. 2015 Aug:37(6):617-27. doi: 10.1007/s00276-015-1438-3. Epub 2015 Feb 1 [PubMed PMID: 25638531]
Level 1 (high-level) evidenceZammit J, Singh D. The peroneus quartus muscle. Anatomy and clinical relevance. The Journal of bone and joint surgery. British volume. 2003 Nov:85(8):1134-7 [PubMed PMID: 14653594]
Level 2 (mid-level) evidenceZhou K, Song L, Zhang P, Wang C, Wang W. Surgical Versus Non-Surgical Methods for Acute Achilles Tendon Rupture: A Meta-Analysis of Randomized Controlled Trials. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2018 Nov-Dec:57(6):1191-1199. doi: 10.1053/j.jfas.2018.05.007. Epub [PubMed PMID: 30368430]
Level 1 (high-level) evidence