Introduction
Fetal circulation differs from adult circulation in a variety of ways to support the unique physiologic needs of a developing fetus. Vascular structures formed early in gestation provide an initial platform for gas exchange and nutrient delivery. Specialized circulatory structures required for systemic circulation then form later in gestation to support the metabolic needs of the fetus before birth.
Development
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Development
Once there is adequate fetal-placental circulation established, blood transports between fetus and placenta through the umbilical cord containing two umbilical arteries and one umbilical vein. The umbilical arteries carry deoxygenated fetal blood toward the placenta for replenishment, and the umbilical vein carries newly oxygenated and nutrient-rich blood back to the fetus. When delivering oxygenated blood throughout the developing fetus, there are unique physiologic needs, supported by specific structures unique to the fetus which facilitate these needs.
The first important structure is a vessel termed the ductus venosus. When the umbilical vein enters the fetal umbilicus, it branches into two veins: the larger ductus venosus, and a smaller portal sinus. The ductus venosus is a vein which largely bypasses the liver and drains most oxygenated blood directly into the inferior vena cava. However, the liver tissue itself still needs an oxygenated blood supply; to provide this, a portion of blood from the umbilical vein enters the smaller second branch, the portal sinus, which carries oxygenated blood to the liver tissue. These branches of the portal sinus and the ductus venosus allow delivery of some oxygenated blood to be distributed throughout the liver while most oxygenated blood is shunted around the liver to continue on through the ductus venosus and into the inferior vena cava.
Once blood has circulated through the liver, the resulting deoxygenated blood from the liver needs to be drained. Deoxygenated blood leaves the liver through the hepatic vein which drains into the inferior vena cava. Thus, deoxygenated blood from the liver drains to the same vessel which the ductus venosus drains to. Therefore, the inferior vena cava in the fetus carries oxygenated blood from the ductus venosus mixed with a small amount of deoxygenated blood from the hepatic vein. This somewhat decreases the oxygen content of the blood in the inferior vena cava; oxygen content is therefore lower in the inferior vena cava than it was in the umbilical vein when it first entered the fetus.[1][2]
After being carried through the inferior vena cava, the next stop for blood is the right atrium of the fetal heart. In an adult, the heart and lungs work together to both replenish the oxygen content of blood, and then pump that oxygenated blood to be distributed throughout the body. In the fetus though, developing lungs are bathed in amniotic fluid and have no access to oxygen. Thus, the placenta supplies all oxygenated blood, and there is no reason for blood to enter the lungs for oxygenation. The fetal heart therefore serves the sole purpose of pumping blood to be distributed throughout the rest of the developing fetus while allowing the vast majority of blood to bypass the lungs. There are two structures that allow for this bypass of the lungs. The first structure is encountered in the right atrium. An opening within the atrial septum termed the foramen ovale carries blood from the right atrium directly into the left atrium, thereby bypassing the right ventricle and lungs. Blood that traverses through the foramen ovale then travels from left atrium to the left ventricle to the ascending aorta and is then pumped into systemic circulation. This is the method by which most blood bypasses the lungs.
A small portion of blood which entered the right atrium will not pass through the foramen ovale though. The direction in which blood in the right atrium is subsequently directed is based mainly on its pattern of flow. Blood may enter the right atrium through the inferior vena cava, which in the fetus carries mostly well-oxygenated blood from the umbilical vein and some deoxygenated blood from the hepatic vein; or blood may enter through the superior vena cava, which carries oxygen-deprived blood from the superior structures of the fetus, including the head and upper limbs.
When following inferior vena cava blood, the well-oxygenated blood from the ductus venosus courses mainly on the medial side of the vessel. When this blood then enters the right atrium, it stays medial, therefore being directed toward the medially-placed foramen ovale. The less-oxygenated blood that came from the hepatic vein courses on the lateral side of the vessel; this less-oxygenated blood then stays lateral when it enters the right atrium, therefore missing the foramen ovale and instead entering the right ventricle, as it would in adult circulation. Similarly, deoxygenated blood entering the right atrium via the superior vena cava misses the foramen ovale in its downward pattern of flow, and it enters the right ventricle as well. This mixture of blood is then pumped from the right ventricle to the pulmonary trunk. However, the lungs are filled with amniotic fluid, creating a pressure which is too high for blood to enter the pulmonary arteries at this point. This is another protective measure, ensuring minimal fetal blood enters the lungs during development. Instead, a second fetal structure for bypassing the lungs exists, connecting the pulmonary artery directly to the descending aorta. This vessel is termed the ductus arteriosus. Ductus arteriosus patency is maintained in utero by prostaglandins, which have dilatory effects on vessels. Blood shunted through the ductus arteriosus then bypasses the lungs and mixes with blood from the descending aorta, which is carrying the blood that had previously passed through the foramen ovale. Blood which had been shunted around the lungs through either mechanism is then pumped into systemic circulation, bringing oxygenated and nutrient-rich blood to the rest of the developing fetal structures. Once oxygenated blood has circulated and unloaded its oxygen to developing tissue, it is delivered back to the placenta via the umbilical arteries to become re-oxygenated and repeat the process.[3]
Overall, as blood delivered in the umbilical vein traverses through fetal vessels, it gradually decreases in oxygen content over time. Multiple sites of circulation at which oxygen content decreases have been discussed, including: the mixing of deoxygenated hepatic vein blood with oxygenated ductus venosus blood in the inferior vena cava; the mixing of deoxygenated blood from the head and arms with oxygenated ductus venosus blood in the right atrium; and unloading of oxygen throughout the rest of fetal circulation.
Notably, when fetal blood is delivered to the placenta, there is no mixing with maternal blood under normal physiologic circumstances. Fetal blood remains within the villi of the chorionic plate, and maternal blood is confined to intervillous spaces between the chorionic villi. Fetal and maternal blood is further separated by a placental membrane between fetal and placental tissue. At the fourth month of gestation, the placental membrane becomes thinner, bringing the fetal side closer to the placental side. This allows for an increased rate of exchange within the placenta to accommodate the increased demand in fetal circulation as the fetus grows larger. Metabolic waste products, gases, and a variety of other substances (for example, immunoglobulins and certain drugs) diffuse down their concentration gradients from one circulation to the other across the placental membrane. Therefore, the placental membrane is not a true barrier; it allows for efficient separation of fetal from maternal blood while still allowing movement of materials to facilitate metabolic and respiratory needs of the fetus.[4]
At the time of birth, multiple changes occur to transition from fetal circulation to infant circulation. All structures unique to fetal circulation are no longer necessary and undergo changes to reflect this. Two main triggers induce the structural changes: cessation of placental blood flow, and the initiation of respiration. The structural changes that occur to each structure are as follows:
- Umbilical arteries: Discontinuation of placental blood flow, and subsequent fall in pressure, causes occlusion of the umbilical arteries a few minutes following delivery. Full occlusion of the distal arteries occurs in the months following birth. Once fully occluded, the distal portions of the former umbilical arteries become the medial umbilical ligaments, found on the anterior abdominal wall. The proximal portions of the former umbilical arteries remain open as the superior vesical arteries.
- Umbilical vein: This vessel remains open for some time after birth, allowing a final volume of blood of approximately 80-100 mL to flow from the placenta into the infant prior to occlusion. Eventually, the umbilical vein also obliterates, forming the ligamentum hepatis teres, which is the lower portion of the falciform ligament, which remains intra-abdominally into adulthood as a fibrous connection between the anterior surface of the liver and the anterior abdominal wall.
- Ductus venosus: At birth, the ductus venosus collapses. Over time, it obliterates into a ligament termed the ligamentum venosus, a fibrous remnant coursing from the ligamentum hepatis teres to the inferior vena cava.
- Foramen ovale: Initiation of respiration opens the pulmonary circulation and lowers dramatically the pulmonary arterial pressure and hence the right atrial pressure. Because of the dramatic increase in pulmonary blood flow, the left atrial pressure increases. Blood preferentially enters the path of least resistance; in the fetus, this path was the ductus arteriosus. In an infant immediately following delivery, lower pressure in the lungs means that lung vasculature has become the new path of least resistance, and the majority of blood will now enter the pulmonary arteries and circulate through the lung vasculature. Subsequently, within the atrial septum, the septum primum is pushed against the septum secundum. Over time, this leads to fusion of the two septa and therefore closure of the foramen ovale. The resulting layer of tissue which completely closes the foramen ovale is termed the fossa ovalis, and it is visible into adulthood as a depression within the septum of the right atrium.
- Ductus arteriosus: Closure of the ductus arteriosus occurs almost immediately following birth. In response to initial respiration, bradykinin gets released from the lungs. Bradykinin then acts on the ductus arteriosus, causing contraction of the muscular vessel walls and subsequent closure of the vessel. Complete obliteration into a fibrous remnant called the ligamentum arteriosum occurs in the months following birth.[5]
Clinical Significance
Umbilical Vein
The brief persistence of blood flow through the umbilical vein after birth is the rationale behind the practice of delayed cord clamping following delivery. Umbilical cords are recommended not to be clamped until at least 30-60 seconds following delivery to allow for the maximum volume of blood to be transferred to the infant before disconnection from the placenta; this has been shown to increase iron stores in the neonate, increase hemoglobin levels, and improve transitional circulation. This practice of delayed cord clamping is therefore recommended following birth unless there is either a maternal or neonatal indication for immediate cord clamping.[6]
Foramen Ovale
The foramen ovale only completely closes as expected in about 75% of adults. In the 25% whose foramen ovale does not close, a patent foramen ovale exists. Fortunately, the left atrial pressure is usually higher than the right atrial pressure, a very tiny amount of blood may be shunted back to the right atrium without any clinical significance. During certain uncommon situations such as Valsalva maneuver, a small amount of deoxygenated blood from the right atrium may be allowed to enter the left atrium, bypassing the lungs without oxygenation. This patency may or may not be symptomatic, and management ranges widely as a result. Often no intervention is required, or surgery may sometimes be indicated to close the patent foramen ovale. Note that this is quite different than an atrial septal defect, in which a pathological opening exists between the left and right atria, and tends to be more severe and usually shows symptoms, whereas a patent foramen ovale may never be detected nor show symptoms.
A complication of patent foramen ovale (PFO) that may be of clinical concern is a paradoxical embolus, which is an embolus originating in systemic venous circulation that travels to the heart, crosses the heart laterally through the patent foramen ovale, and can result in a stroke. However, it is an uncommon occurrence given the high prevalence of patent foramen ovale and the low prevalence of paradoxical emboli.[7] The risk is predictably related to the size of the PFO.
Ductus Arteriosus
The ductus arteriosus may persist, failing to obliterate within the months after birth and has associations with congenital rubella infections and as well as with preterm delivery.[8] The resulting patent ductus arteriosus (PDA, see figure) will allow for a small volume of blood to flow continuously from the aorta to the pulmonary circulation and rarely some deoxygenated blood to enter systemic circulation from the pulmonary artery. This continuous shunt of blood is the basis of a continuous murmur on auscultation. If left untreated for years, the increase in pulmonary blood flow caused by the increase in the aortic to pulmonary arterial shunt will result in pulmonary arterial hypertension and more right to left shunt and more deoxygenation of the systemic circulation causing cyanosis. The affected individual may start showing signs of cyanosis, typically in the lower extremities, due to a decreased amount of oxygen delivery. Management of a PDA is highly dependent on the clinical situation.
If a PDA is the only defect following delivery, and no other cardiac abnormalities are present, a prostaglandin synthesis inhibitor may be used to disrupt the prostaglandin production that is contributing to the maintained patency of the vessel. Indomethacin, a COX-2 inhibitor, has historically been the treatment of choice; ibuprofen and acetaminophen may also be efficacious options, although more research is needed.[9] Surgical closure may also be a consideration. Conversely, there are certain cyanotic congenital heart defects (for example, transposition of the great vessels) in which the circulatory system allows little or no deoxygenated blood delivery to the lungs. As a result, little or no oxygenated blood can be delivered systemically, causing cyanosis in peripheral tissues. In this case, therapeutically maintaining a patent ductus arteriosus allows some mixing of oxygenated and deoxygenated blood, allowing some amount of oxygenated blood into systemic circulation, which can assist in decreasing the severity of cyanosis in affected infants. To accomplish this, prostaglandin E1 may be administered to maintain patency of the ductus arteriosus until surgical correction of the underlying heart defect can be performed.[10]
Media
(Click Image to Enlarge)
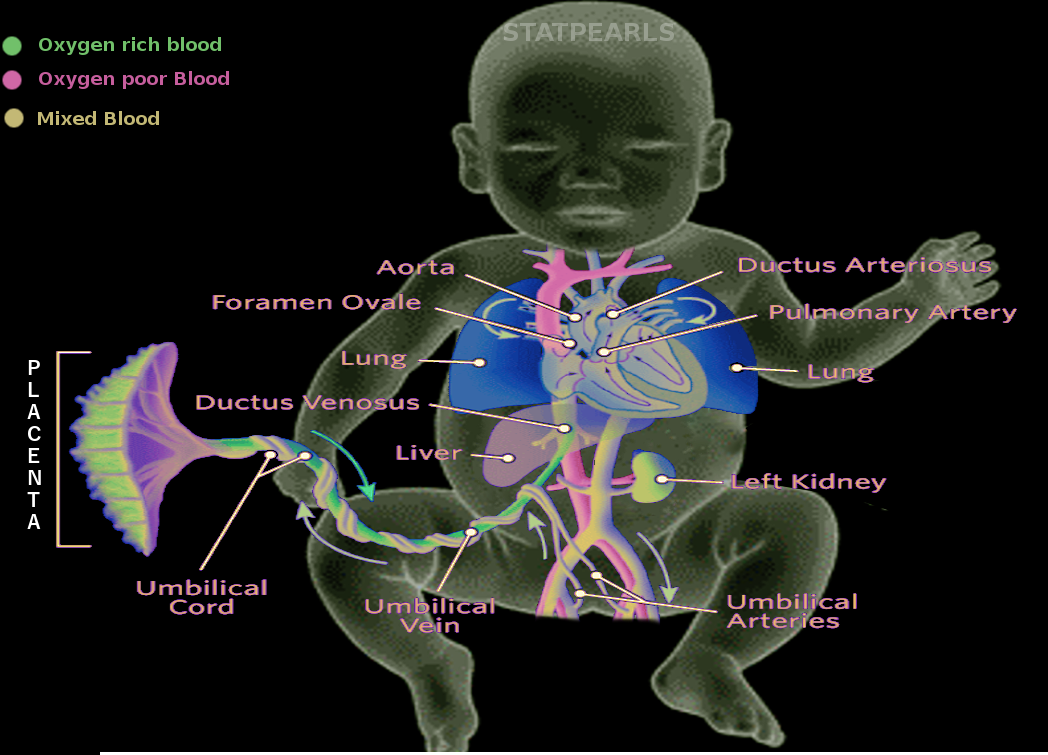
Fetal circulation Image courtesy S Bhimji MD
References
Kiserud T, Stratford L, Hanson MA. Umbilical flow distribution to the liver and the ductus venosus: an in vitro investigation of the fluid dynamic mechanisms in the fetal sheep. American journal of obstetrics and gynecology. 1997 Jul:177(1):86-90 [PubMed PMID: 9240587]
Level 3 (low-level) evidenceGürses C, Karadağ B, İsenlik BST. Normal variants of ductus venosus spectral Doppler flow patterns in normal pregnancies. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2020 Apr:33(8):1288-1294. doi: 10.1080/14767058.2018.1517323. Epub 2018 Oct 1 [PubMed PMID: 30153762]
DAWES GS. The umbilical circulation. American journal of obstetrics and gynecology. 1962 Dec 1:84():1634-48 [PubMed PMID: 14025579]
HOLMES RP, DAVIES DV. The vascular pattern of the placenta and its development in the rat. The Journal of obstetrics and gynaecology of the British Empire. 1948 Oct:55(5):583-607 [PubMed PMID: 18892167]
Level 3 (low-level) evidenceHillman NH, Kallapur SG, Jobe AH. Physiology of transition from intrauterine to extrauterine life. Clinics in perinatology. 2012 Dec:39(4):769-83. doi: 10.1016/j.clp.2012.09.009. Epub [PubMed PMID: 23164177]
. Committee Opinion No. 684: Delayed Umbilical Cord Clamping After Birth. Obstetrics and gynecology. 2017 Jan:129(1):1. doi: 10.1097/AOG.0000000000001860. Epub [PubMed PMID: 28002310]
Level 3 (low-level) evidenceAarli SJ, Kråkenes J, Omdal TR, Waje-Andreassen U. Patent foramen ovale in an elderly male with multiple embolic infarcts. Clinical case reports. 2018 Dec:6(12):2403-2406. doi: 10.1002/ccr3.1852. Epub 2018 Oct 26 [PubMed PMID: 30564337]
Level 3 (low-level) evidenceOster ME, Riehle-Colarusso T, Correa A. An update on cardiovascular malformations in congenital rubella syndrome. Birth defects research. Part A, Clinical and molecular teratology. 2010 Jan:88(1):1-8. doi: 10.1002/bdra.20621. Epub [PubMed PMID: 19697432]
Ferguson JM. Pharmacotherapy for patent ductus arteriosus closure. Congenital heart disease. 2019 Jan:14(1):52-56. doi: 10.1111/chd.12715. Epub 2018 Dec 11 [PubMed PMID: 30536827]
Akkinapally S, Hundalani SG, Kulkarni M, Fernandes CJ, Cabrera AG, Shivanna B, Pammi M. Prostaglandin E1 for maintaining ductal patency in neonates with ductal-dependent cardiac lesions. The Cochrane database of systematic reviews. 2018 Feb 27:2(2):CD011417. doi: 10.1002/14651858.CD011417.pub2. Epub 2018 Feb 27 [PubMed PMID: 29486048]
Level 1 (high-level) evidence