
Introduction
Abdominal thrusts or the Heimlich maneuver is a first-aid procedure used to treat upper airway obstruction caused by a foreign body. This skill is commonly taught during basic life support (BLS) and advanced cardiac life support (ACLS) classes, but it never receives as much attention as chest compressions and rescue breaths do. The abdominal thrust maneuver can be performed in both children and adults via different techniques.[1]
In the 1960s, choking on food, toys, and other objects was the sixth leading cause of accidental death in the United States. Slapping individuals on the back was the main response and was frequently found to be ineffective, at times even lodging the object further down.[2]
The Heimlich maneuver was initially introduced in 1974 by Dr. Henry Heimlich after proving his theory that the reserve of air in the lung could serve to dislodge objects from the esophagus by quick upwards thrust under the ribcage.[3][4] The medical community of the time did not embrace the maneuver right away. The American Red Cross (ARC) and the American Heart Association (AHA) continued to promoted backslaps for ten years after the introduction of the Heimlich maneuver.[5][6]
Today, the Heimlich maneuver is accepted and taught during BLS and ACLS for conscious adults, but backslaps are still a recommendation for infants, and chest compressions are recommended for unconscious patients. Furthermore, different techniques of the maneuver have been developed with conflicting effectiveness results.[7]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The anatomy associated with the Heimlich maneuver mainly focuses on expelling a foreign body by standing on the rear of the patient, placing arms around, and delivering a sharp inward and upward thrust to the abdomen below the rib cage.[8] Foreign objects associated with choking are usually stuck above the cricoid cartilage in the supra-laryngeal area. As for the maneuver itself, the thrusts must be executed over the epigastric region just below the ribcage and directed upwards towards the head of the patient.[9] If the patient is pregnant, the thrust maneuver can be performed over the sternum.
Physiologically, the abdominal thrust maneuver is effective due to increasing intrathoracic pressure affecting the lung/airway, stomach, and esophagus produced by diaphragmatic thrusts.[10]
Indications
The only accepted indication for the abdominal thrust maneuver is that of the conscious choking adult from a lodged supra-laryngeal foreign body. The universal choking sign is the main indication for the Heimlich maneuver. This sign consists of the inability to speak, breathe, or cough while holding both hands up to one's own throat.[11]
Although initially reported to help with asthma and drowning patients, the Heimlich maneuver has not proven to help with these diagnoses.[12] Another case study presented the inadequate purging use of the Heimlich maneuver in teenagers with eating disorders.[9]
Contraindications
Although there are no absolute contraindications, the abdominal thrust maneuver is not recommended by the AHA for infants or unconscious patients. Also, pregnant subjects should receive management with sternal compressions, as opposed to abdominal.[13]
Personnel
The importance and utility of the Heimlich maneuver lie in the fact that it does not require expertise but simple training of the public.[14] When Dr. Heimlich introduced the abdominal thrust maneuver in 1974 through live television, it was not until real-life anecdotes from viewers came along that the medical community accepted it.[3] Today, it is commonly taught in BLS classes and does not require equipment.
Preparation
Cases of choking happen in mere seconds and unexpectedly, making preparation nearly impossible. As mentioned above, the Heimlich maneuver is taught during BLS for the conscious choking adult.
Technique or Treatment
The commonly known abdominal thrust maneuver, known as the Heimlich maneuver, is performed by a bystander on a person who appears to be choking. The bystander stands behind the subject and wraps his/her arms around the upper abdominal region, about two inches above the belly button. Making a fist with one hand and wrapping the other hand tightly over the fist and delivering five sharp midline thrusts inward and upward.[15] Recently, other techniques such as the circumferential (horizontal) abdominal thrust, chair thrust, and auto up-thrust have been studied comparing the gastric and esophageal pressures generated with each, finding that chair thrusts might be more effective in these parameters.[7]
Other studies report higher effectiveness of lateral thoracic and abdominal thrusts in the generation of airway pressure as studied in pigs.[16][17] A manikin study in 2017 reported improved effectiveness of the Heimlich maneuver while on a supine or prone position for adults and prone position for children.[18] Another study reports using a modified table Heimlich maneuver with success in four unconscious patients.[19]
Complications
Ever since the introduction of the Heimlich maneuver, cases of harm inflicted by the forceful displacement of the diaphragm and sudden increase in intrathoracic pressure have driven numerous studies and reviews. Although this maneuver is considered life-saving and generally safe to perform, serious intra-abdominal harm can ensue from incorrect technique and unusually vigorous application.[20] One manikin study mentioned above also concluded that the risk of serious harm ensues if the foreign body is not relieved after the first set of thrusts.[18] The most commonly reported complications are rib fractures and gastric or esophageal perforations. Although other rare traumatic injuries such as splenic rupture, pneumomediastinum, aortic valve cusp rupture, aortic dissection, diaphragmatic herniation, esophageal and jejunal perforation, hepatic rupture, cholesterol embolization leading to arterial occlusion, and mesenteric laceration have been described.[21][22][23][24][25][26][27][28]
Clinical Significance
The abdominal thrust maneuver impact on basic life support, both in the medical and public sector, cannot be quantified. Despite the rare instances of intraabdominal complications, the Heimlich maneuver is considered a quick and inexpensive technique that does not require medical knowledge or expertise to perform.[3] With the addition of the maneuver by the AHA into the BLS program, medical performance and effectiveness of cardiopulmonary resuscitation improved.[29] A 2015 study evidenced the improved outcomes of patients treated in the field by bystanders in comparison with those treated initially in the hospital.[30]
Enhancing Healthcare Team Outcomes
The Heimlich maneuver exemplifies what is achievable by involving the general population in community healthcare. BLS training is progressively a requirement for an increasing part of the community, even including high-school students.[31] [Level 3] Ultimately, the overall improvement in patient outcomes has relied heavily on bystander cardiopulmonary resuscitation and basic life support.[32] [Level 1]
Media
(Click Image to Enlarge)
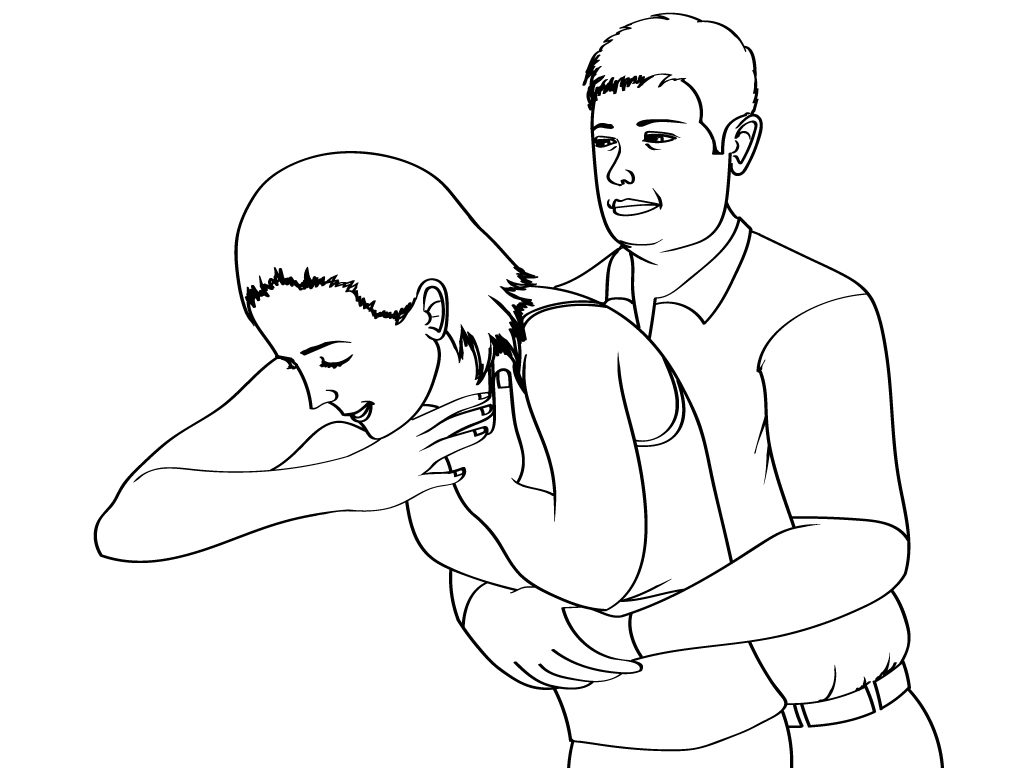
Abdominal Thrust
Contributed by Scott Dulebohn, MD
References
Pai-Dhungat JV, Parikh F. Heimlich Manoeuvre. The Journal of the Association of Physicians of India. 2015 Mar:63(3):123-4 [PubMed PMID: 26543985]
Hoffman JR. Treatment of foreign body obstruction of the upper airway. The Western journal of medicine. 1982 Jan:136(1):11-22 [PubMed PMID: 7072236]
Roehr B. Henry Heimlich. BMJ (Clinical research ed.). 2017 Jan 9:356():j118. doi: 10.1136/bmj.j118. Epub 2017 Jan 9 [PubMed PMID: 28069709]
Shampo MA, Kyle RA. Henry Heimlich--Heimlich maneuver. Mayo Clinic proceedings. 2000 May:75(5):474 [PubMed PMID: 10807076]
Sternbach G, Kiskaddon RT. Henry Heimlich: a life-saving maneuver for food choking. The Journal of emergency medicine. 1985:3(2):143-8 [PubMed PMID: 4093566]
Heimlich HJ, Patrick EA. The Heimlich maneuver. Best technique for saving any choking victim's life. Postgraduate medicine. 1990 May 1:87(6):38-48, 53 [PubMed PMID: 2186401]
Pavitt MJ, Swanton LL, Hind M, Apps M, Polkey MI, Green M, Hopkinson NS. Choking on a foreign body: a physiological study of the effectiveness of abdominal thrust manoeuvres to increase thoracic pressure. Thorax. 2017 Jun:72(6):576-578. doi: 10.1136/thoraxjnl-2016-209540. Epub 2017 Apr 12 [PubMed PMID: 28404809]
Godet M, Chevillotte J. [Nursing care of airway obstruction caused by food]. Revue de l'infirmiere. 2015 May:(211):47-8. doi: 10.1016/j.revinf.2015.02.018. Epub [PubMed PMID: 26145700]
Boachie A, Kusi Appiah E, Jubin M, Jasper K. Purging using the Heimlich maneuver among children and adolescents with eating disorders. The International journal of eating disorders. 2015 Sep:48(6):795-7. doi: 10.1002/eat.22408. Epub 2015 Apr 2 [PubMed PMID: 25846517]
Nilsson O, Norlander T, Linder A. [Foreign body in the airways]. Lakartidningen. 2012 Dec 19-2013 Jan 8:109(51-52):2361-5 [PubMed PMID: 23367552]
Yildirim E. Principles of Urgent Management of Acute Airway Obstruction. Thoracic surgery clinics. 2018 Aug:28(3):415-428. doi: 10.1016/j.thorsurg.2018.05.006. Epub [PubMed PMID: 30054079]
Rosen P, Stoto M, Harley J. The use of the Heimlich maneuver in near drowning: Institute of Medicine report. The Journal of emergency medicine. 1995 May-Jun:13(3):397-405 [PubMed PMID: 7673638]
Guildner CW, Williams D, Subitch T. Airway obstructed by foreign material: the Heimlich maneuver. JACEP. 1976 Sep:5(9):675-7 [PubMed PMID: 1018395]
Patsaki A, Pantazopoulos I, Dontas I, Passali C, Papadimitriou L, Xanthos T. Evaluation of Greek high school teachers' knowledge in basic life support, automated external defibrillation, and foreign body airway obstruction: implications for nursing interventions. Journal of emergency nursing. 2012 Mar:38(2):176-81. doi: 10.1016/j.jen.2010.09.002. Epub 2010 Oct 20 [PubMed PMID: 22401622]
Pai-Dhungat JV, Parikh F. Heimlich Maneuver. The Journal of the Association of Physicians of India. 2008 Sep:56():715 [PubMed PMID: 19086360]
Lippmann J, Taylor DM, Slocombe R, McDonald CF, Walker T, Nolan G. Lateral versus anterior thoracic thrusts in the generation of airway pressure in anaesthetised pigs. Resuscitation. 2013 Apr:84(4):515-9. doi: 10.1016/j.resuscitation.2012.11.024. Epub 2012 Nov 29 [PubMed PMID: 23200993]
Level 3 (low-level) evidenceRottenberg EM. Could there ever be evidence to support using lateral chest thrusts in humans with the victim lying on their side to clear upper-airway obstruction? Resuscitation. 2013 Jun:84(6):e69. doi: 10.1016/j.resuscitation.2013.01.039. Epub 2013 Feb 27 [PubMed PMID: 23454441]
Level 3 (low-level) evidenceIchikawa M, Oishi S, Mochizuki K, Nitta K, Okamoto K, Imamura H. Influence of body position during Heimlich maneuver to relieve supralaryngeal obstruction: a manikin study. Acute medicine & surgery. 2017 Oct:4(4):418-425. doi: 10.1002/ams2.297. Epub 2017 Jul 17 [PubMed PMID: 29123902]
Blain H, Bonnafous M, Grovalet N, Jonquet O, David M. The table maneuver: a procedure used with success in four cases of unconscious choking older subjects. The American journal of medicine. 2010 Dec:123(12):1150.e7-9. doi: 10.1016/j.amjmed.2010.07.010. Epub 2010 Oct 1 [PubMed PMID: 20870197]
Level 3 (low-level) evidenceWolf DA. Heimlich trauma: a violent maneuver. The American journal of forensic medicine and pathology. 2001 Mar:22(1):65-7 [PubMed PMID: 11444666]
Level 3 (low-level) evidenceCecchetto G, Viel G, Cecchetto A, Kusstatscher S, Montisci M. Fatal splenic rupture following Heimlich maneuver: case report and literature review. The American journal of forensic medicine and pathology. 2011 Jun:32(2):169-71. doi: 10.1097/PAF.0b013e318219c878. Epub [PubMed PMID: 21512385]
Level 3 (low-level) evidenceMatharoo G, Kalia A, Phatak T, Bhattacharyya N. Diaphragmatic rupture with gastric volvulus after Heimlich maneuver. European journal of pediatric surgery : official journal of Austrian Association of Pediatric Surgery ... [et al] = Zeitschrift fur Kinderchirurgie. 2013 Dec:23(6):502-4. doi: 10.1055/s-0032-1330850. Epub 2012 Nov 21 [PubMed PMID: 23172561]
Dupre MW, Silva E, Brotman S. Traumatic rupture of the stomach secondary to Heimlich maneuver. The American journal of emergency medicine. 1993 Nov:11(6):611-2 [PubMed PMID: 8240565]
Level 3 (low-level) evidenceCouper K, Abu Hassan A, Ohri V, Patterson E, Tang HT, Bingham R, Olasveengen T, Perkins GD, International Liaison Committee on Resuscitation Basic and Paediatric Life Support Task Force Collaborators. Removal of foreign body airway obstruction: A systematic review of interventions. Resuscitation. 2020 Nov:156():174-181. doi: 10.1016/j.resuscitation.2020.09.007. Epub 2020 Sep 16 [PubMed PMID: 32949674]
Level 1 (high-level) evidencePawlukiewicz AJ, Merrill DR, Griffiths SA, Frantz G, Bridwell RE. Cholesterol embolization and arterial occlusion from the Heimlich maneuver. The American journal of emergency medicine. 2021 May:43():290.e1-290.e3. doi: 10.1016/j.ajem.2020.09.079. Epub 2020 Sep 30 [PubMed PMID: 33036850]
Lee KY, Wu YL, Ho SW. Silent Aortic Dissection after the Heimlich Maneuver: A Case Report. The Journal of emergency medicine. 2019 Feb:56(2):210-212. doi: 10.1016/j.jemermed.2018.09.053. Epub 2018 Nov 9 [PubMed PMID: 30420310]
Level 3 (low-level) evidenceKoss SL, Karle WE, Dibelius G, Kamat A, Berzofsky C. Esophageal perforation as a complication of the Heimlich maneuver in a pediatric patient: A case report. Ear, nose, & throat journal. 2018 Jul:97(7):E1-E3 [PubMed PMID: 30036437]
Level 3 (low-level) evidenceTruong T, Salire K, De Cicco I, Cherian S, Aisenberg G. Incarcerated diaphragmatic hernia following Heimlich maneuver. Proceedings (Baylor University. Medical Center). 2018 Jan:31(1):48-50. doi: 10.1080/08998280.2017.1391034. Epub 2017 Dec 4 [PubMed PMID: 29686551]
Onan A, Simsek N, Elcin M, Turan S, Erbil B, Deniz KZ. A review of simulation-enhanced, team-based cardiopulmonary resuscitation training for undergraduate students. Nurse education in practice. 2017 Nov:27():134-143. doi: 10.1016/j.nepr.2017.08.023. Epub 2017 Sep 4 [PubMed PMID: 28892727]
Kinoshita K, Azuhata T, Kawano D, Kawahara Y. Relationships between pre-hospital characteristics and outcome in victims of foreign body airway obstruction during meals. Resuscitation. 2015 Mar:88():63-7. doi: 10.1016/j.resuscitation.2014.12.018. Epub 2014 Dec 31 [PubMed PMID: 25555359]
Level 2 (mid-level) evidenceChoi HS, Lee DH, Kim CW, Kim SE, Oh JH. Peer-assisted learning to train high-school students to perform basic life-support. World journal of emergency medicine. 2015:6(3):186-90. doi: 10.5847/wjem.j.1920-8642.2015.03.004. Epub [PubMed PMID: 26401178]
Bradley SM, Rea TD. Improving bystander cardiopulmonary resuscitation. Current opinion in critical care. 2011 Jun:17(3):219-24. doi: 10.1097/MCC.0b013e32834697d8. Epub [PubMed PMID: 21499092]
Level 3 (low-level) evidence