Introduction
Bouveret syndrome is a rare complication of gallstone disease (0.3% to 0.5%), characterized by gastric outlet obstruction.[1] This infrequent form of gallstone ileus arises from the impaction of a large stone in the proximal duodenum or pylorus secondary to a spontaneous fistula between the gallbladder and the duodenum or stomach. Due to its rare nature, only 315 cases have been reported in 50 years between 1967 and 2016.[2] It was first described preoperatively by French surgeon M. Beassier in 1770. However, subsequently, L. Bouveret, a French physician, published two comprehensive case reports in 1896 of this condition, and it was named after him.[3]
Bouveret syndrome has a high mortality, estimated at 12 to 30%, because an elderly age group is usually afflicted, delay of diagnosis owing to its non-specific presentation and complexity of the disease.[4] Also, because the disease is rare, there is no agreed guidance of diagnostic workup and management, including endoscopic, laparoscopic, and open surgery.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Bouveret syndrome is the most infrequent variant of gallstone ileus. It results from a gallstone migrating through a bilioenteric fistula and causing obstruction at the gastric outlet and occasionally in also other portions of the intestine. The entry point is typically a fistula between the gallbladder and a portion of the stomach or intestine.[5][6]
The well-studied risk factors for Bouveret syndrome include a history of cholelithiasis, stones greater than 2 cm to 8 cm, female gender, and age older than 60 years. It has been reported that approximately 43% to 68% of patients have a history of recurrent biliary colic, jaundice, or acute cholecystitis.[7]
Epidemiology
Bouveret syndrome is extremely rare and constitutes 1 to 3% of all obstructions caused by gallstones in the gastrointestinal tract, representing 0.3 to 5% of cholelithiasis complications.[8][4] However, most stones are relatively small and pass either unnoticed or with terminal ileum impaction. The highest prevalence of Bouveret syndrome is among frail older women, with a median age of 74 years and a female-to-male ratio of 1.9.[9][10] Thus, it has disproportionately high rates of morbidity and mortality.
Pathophysiology
Following an attack of acute cholecystitis, the resulting inflammation and adhesion of the gallbladder to GI, together with mechanical pressure applied by gallstones on the gallbladder itself and bowel wall, may result in an ischemic tear of the apposed gallbladder and enteric wall; this mechanism potentiates a fistula between the gallbladder and bowel where the gallstone could pass.[11] Apart from acute cholecystitis, a few case reports have been published of the development of a cholecystoenteric fistula consequent to a gallbladder malignancy.[12][13][14]
Bilioenteric fistulas usually present as cholecystoduodenal fistulas and contribute to 68% of the cases. Less common variants, cholecystocolic or cholecystogastric fistulas, account for 17% and 5% of the cases respectively.[15] Cholecystogastric fistula is probably the rarest because of the thickness of the gastric wall.[16] However, most ectopic gallstones pass through defecation or vomiting, even with a bilioenteric fistula. Clinically symptoms of GOO are likely to arise with larger stones in addition to other factors like pre-existing stenosis or post-surgical altered anatomy of the GI tract.[15][17]
History and Physical
The presentation of Bouveret syndrome is typically non-specific and often with waxing and waning symptoms of nausea and vomiting (present in 85% of patients), abdominal distension, and pain (present in 70% of patients) due to the varying locations of the gallstone. The patient may also exhibit epigastric and right hypochondrium pain and signs of dehydration and weight loss. Less frequently, Bouveret syndrome may present with hematemesis secondary to duodenal and celiac artery erosions or the expulsion of stones in the vomitus. Usually, the symptoms begin 5 to 7 days before patients seek medical consultation. Notably, the intensity of the pain often does not correlate with the underlying anatomic alteration.
A physical exam is also non-specific, although one may appreciate dry mucous membranes, abdominal distension, abdominal tenderness, high-pitched bowel sounds, and obstructive jaundice.[18]
Evaluation
Unfortunately, laboratory studies are typically non-specific. Labs may show jaundice and hepatic enzyme alterations, but this is only seen in about one-third of the patients with Bouveret syndrome. Leucocytosis, electrolyte abnormalities, acid-base alterations, and renal failure may also be present, but the grade depends on the comorbidity, the intensity of the inflammatory response, and the compensatory mechanisms of the individual. As far as imaging is concerned, the constellation of pneumobilia, bowel obstruction, and an aberrant gallstone referred to as Rigler's triad is highly suggestive of Bouveret syndrome but is only found in 40% to 50% of cases. Ultrasound may be useful, showing possible cholecystitis, dilated stomach, pneumobilia, and ectopic location of gallstone, yet bowel gas makes it suboptimal. If the gallbladder is contracted, it may be difficult to detect the exact location of the stone (orthotopic or ectopic) using ultrasound.[19][20][21]
Abdominal radiographs, though non-specific, may help identify Bouveret syndrome. The subtle cues include pneumobilia, intestinal obstruction, aberrantly located gallstone, air-fluid levels in the right upper quadrant due to air in the gallbladder, gastric distention, and a change in the location of a previously observed stone. However, abdominal radiographs are only diagnostic in 21% of Bouveret syndrome cases. CT is the imaging modality of choice, with an overall 93% sensitivity, 100% specificity, and 99% diagnostic accuracy. In addition to its higher accuracy than plain radiograph or ultrasound, it can also provide important information about the presence of a fistula, presence of an abscess, inflammatory state of the surrounding lumen and tissue, size of gallstone, and the number of gallstones.
In patients unable to tolerate oral contrast or with intense emesis, as well as in cases with iso-attenuating stones, magnetic resonance cholangiopancreatography (MRCP) can be utilized, as it distinguishes stones from fluid, visualizes the fistula with good precision, and does not require the use of oral contrast material. Esophagogastroduodenoscopy (EGD) is another option, with diagnostic and therapeutic advantages. However, simultaneous removal of the stone is only successful in a minority of cases and can be associated with further complications. In about 20% to 40% of cases, the final diagnosis is established intra-operatively when a patient is undergoing laparotomy for small bowel obstruction of an unknown cause. This applies particularly to the 15% to 25% of gallstones that are iso-attenuating and not visible on CT scans.[22][18]
Treatment / Management
The chance of spontaneous resolution of Bouveret syndrome after conservative treatment is rare.[18] Also, a dislodged stone can cause distal obstruction. Endoscopic intervention is currently the first line of treatment of this syndrome. Many case reports of successful endoscopic management have been published in recent decades.[23] The first successful endoscopic visualization and extraction of gallstones of three cases was published in 1985.[24] Subsequently, endoscopic nets and lithotripsy modalities were developed for gallstone extraction. This minimally invasive approach enjoys lower mortality and morbidity rates of endoscopy vs. surgery (1.6% vs. 17.3%) for Bouveret syndrome.[23] However, it has a markedly reduced success rate in contrast to surgical intervention (43.0% vs. 94.1%).[25](A1)
Decompression of the distended stomach by a nasogastric tube should be performed prior to therapeutic endoscopy to reduce the risk of aspiration. More endoscopy-based treatment options have become available with continued progress and refinement of endoscopic techniques over the last two decades. This improvement is reflected in rising success rates for the treatment of Bouveret’s syndrome from 13.6% - 18.0% to 43.0%.[18][25][26] Minimally invasive treatment includes endoscopic retrieval, in addition to mechanical, electrohydraulic lithotripsy, laser, and extracorporeal shock wave. Extraction of impacted stones by Endoscopic graspers, nets, snares, or baskets can be tried. An esophageal overtube or latex rubber can be used to avoid esophageal injury during extraction. Endoscopic nets are reportedly more effective for treating smaller-sized stones than larger ones.[27] Stones of diameter exceeding 2.5 cm need lithotripsy fragmentation to enhance easy passage through the distal alimentary tract and safe removal.(A1)
Mechanical lithotripsy is a common method used, and fluoroscopy is a preferable adjunct to avoid the instrument wrongly entering the cholecystoenteric fistula. The other common method of lithotripsy is electrohydraulic lithotripsy (EHL). High EHL intensity may be needed because of the large gallstones commonly found in cases of Bouveret syndrome.[28] The other problem with EHL is that incidental focusing of the shock waves on the intestine wall may cause bleeding and perforation.[29] Other endoscopic methods are laser lithotripsy (LL) and extracorporeal shockwave lithotripsy (ESWL). The former was used in the mid-1980s for bile duct stones treatment.[30][31] LL has been reported to be effective and safe in treating complicated bile duct stones.[32][33] The benefit of using LL is the precise targeting of energy onto the stone with minimal tissue injury. The direct visual control of the laser application makes the treatment technically easy and safe.[34][35][36] The Food and Drug Administration has approved holmium and neodymium yttrium aluminum garnet lasers as treatments and is available in the market.[37] ESWL has a higher failure rate and is limited by lacking endoscopic control. Utilization of intraoperative ultrasound during ESWL is advisable to tackle the gallstones, as the intraabdominal gases often impede plain XR.[23][38](B3)
Of all the successful endoscopic interventions which have been published in the recent decades, visualization of the gallstones was achieved in approximately two-thirds of cases.[23] Moreover, less than two-thirds can be removed successfully.[18] Endoscopic modality may require more than one session, and fragments of stones can cause postoperative gallstone ileus.[23] Therefore, it is essential to remove these fragments at the end of the procedure.[34] Even so, endoscopic modalities present convenient alternatives, especially when patients are not suitable for surgery. Also, the success rate of these techniques will continue to increase in the future as technology continues to progress.(B3)
Surgery was considered first-line treatment in the past and has demonstrated higher success rates than the minimally invasive modality —up to 90% for enteric or gastric lithotomy alone and up to 82% with simultaneous fistula repair and cholecystectomy.[18] However, surgery has remarkable morbidity and mortality, 37.5% and 11%, respectively.[39] As this disease is usually seen in elderly patients with significant comorbidities, surgery is not feasible for many of these patients. Surgical options may need to be considered to treat patients with Bouveret syndrome when an endoscopic attempt is unsuccessful or no technical expertise is available. The surgical approach consists of open gastrotomy, pylorotomy, or duodenotomy at or proximal to the site of obstruction. Gastrotomy can be used for stone removal if it is possible to manipulate an impacted duodenal gallstone into the stomach.[40] With a distal duodenal impacted stone or a migrated stone into the proximal part of the jejunum, an enterotomy distal to Trietz ligament may be used for stone removal. The distal part of the small intestine must be examined to ensure no other migrated large stones may result in postoperative ileus. Endoscopy may be used as an adjunct to help maneuver the stone into a more suitable location to perform enterotomy or gastrotomy if the gallstone is detected in a difficult area to access during open surgery in one or two sessions.[41][42](B3)
Open surgery of Bouveret syndrome has high morbidity and mortality. When laparoscopic equipment and expertise are available, laparoscopic enterolithotomy should be considered the preferred approach and has been reported as effective and safe in managing this condition in the failure or unavailability of endoscopic therapies.[43][44] However, higher rates of conversion are seen in these difficult cases.[45][46] As with an open approach, stones can be removed by a laparoscope through duodenotomy, pylorotomy, or gastrotomy. After removing impacted gallstones, the small intestine needs to be examined to ensure there are no retained stones.(B3)
Cholecystectomy and fistula repair in one or a multi-step approach to treat Bouveret syndrome is debatable. Most patients are poor surgical candidates as they are older and have multiple comorbidities. Cholecystectomy with fistula repair is generally not recommended as the benefits of cholecystectomy in these patients generally outweigh the risks of further operations or complications from gallstones. However, there is always a risk for recurrent gallstone ileus and gallstone pancreatitis if the fistula is not repaired.[47] It is recommended to perform cholecystectomy in younger patients as there may be an increased risk of gallbladder cancer with cholecystoenteric fistula. Also, cholecystectomy is recommended if malignancy cannot be excluded with diagnostic imaging before surgery.[48] Cholecystectomy warrants consideration in other special conditions, including the previous history of gallstone ileus, common bile duct stone, and gallstone pancreatitis.[49](B3)
Differential Diagnosis
Congenital Cause
- Duodenal web
Inflammatory Causes
- Erosive gastritis
- Peptic ulcer disease
- Crohn disease
Malignant Causes
- Gastric antral carcinoma
- Duodenal carcinoma
- Pancreatic carcinoma
- Ampullary carcinoma
- Cholangiocarcinoma
Prognosis
Bouveret syndrome generally carries a good prognosis provided timely diagnosis and management.
Complications
The complications of untreated Bouveret syndrome include ongoing gastric outlet obstruction resulting in anorexia, dehydration, nutritional deficiencies, and electrolyte abnormalities. The most feared complication is intestinal perforation which can lead to major morbidities.
Specific complications are related to the mode of treatment strategy employed. Incomplete lithotripsy may lead to recurrent gallstone ileus. Shock wave dispersion may lead to damage to surrounding structures. If a fistula is not excised, there is a risk of recurrent Bouveret syndrome, biliary sepsis, gallstone pancreatitis, and theoretical cancer risk. Surgery in itself carries the inherent risks of bleeding and infection. In addition, cholecystectomy may result in inadvertent injury to the biliary tree, especially in the presence of inflammation.[50]
Deterrence and Patient Education
Patients who have endoscopic or surgical removal of obstructing stones only without closure of the cholecystoduodenal fistula should be educated on the potential complications of patency of this fistula. These include recurrence of bowel obstruction due to migration of other stones, biliary sepsis, and acute pancreatitis. Therefore, these should seek the emergency department in case of experiencing severe abdominal pain and vomiting.
Pearls and Other Issues
Although a large gallstone is the cause of gastric outlet obstruction, a history of prior gallstone disease is only present in a few patients. Nevertheless, the condition should be considered in the differential diagnosis in elderly patients who have a history of chronic cholecystitis and present with repeated episodes of hematemesis or vomiting.
Enhancing Healthcare Team Outcomes
Bouveret syndrome is a very rare cause of gastric outlet obstruction. Both the diagnosis and management are complex, and the disorder carries high morbidity and mortality. These patients are best managed by an interprofessional team that includes an emergency department physician, a general surgeon, a radiologist, a gastroenterologist, and specialty nurses. The best method of managing these patients still has not been determined, but the patients need close monitoring in an ICU setting. Wound infections, fistula formation, and multiorgan failure have all been reported. The nurse must ensure that the patients have DVT prophylaxis as many patients remain bedridden for a prolonged time.[51][52][53]
Media
(Click Image to Enlarge)
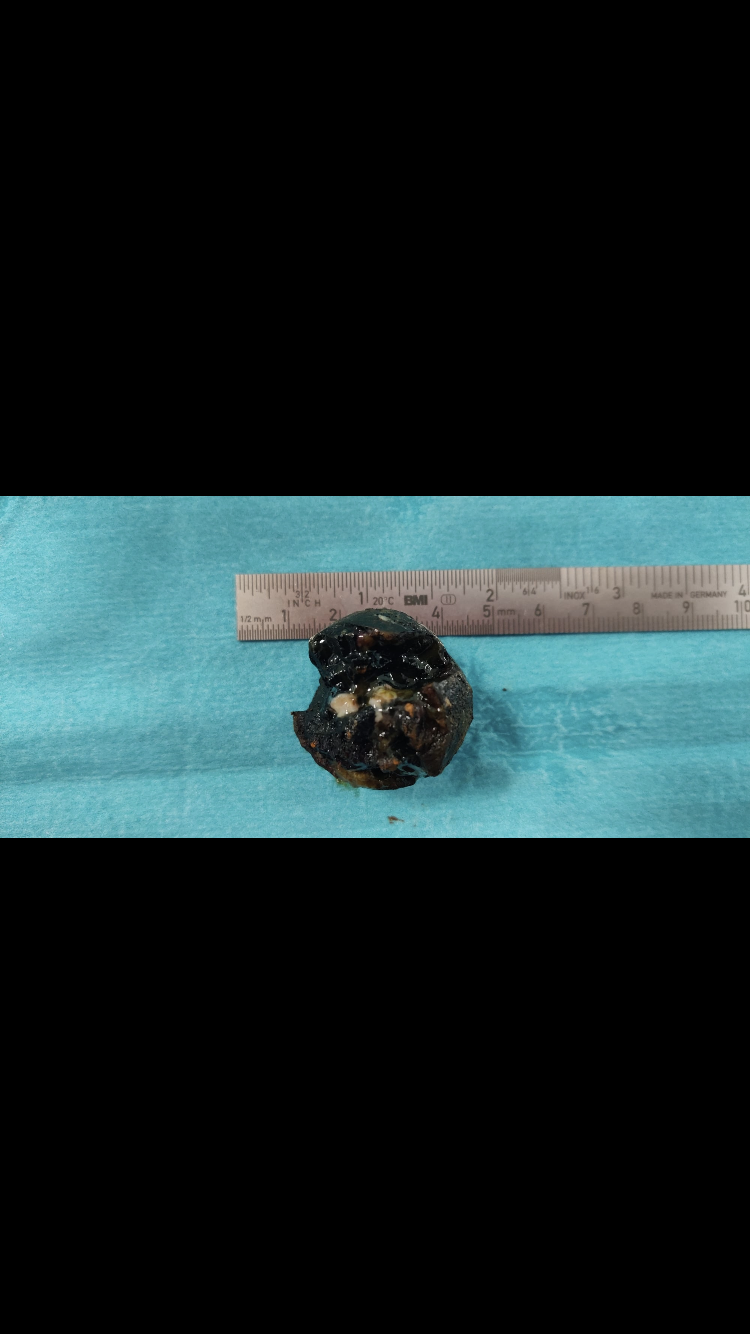
Gallstone extracted after migrating and causing gallstone ileus in the jejunum Contributed by Jasim Al-Musawi
(Click Image to Enlarge)
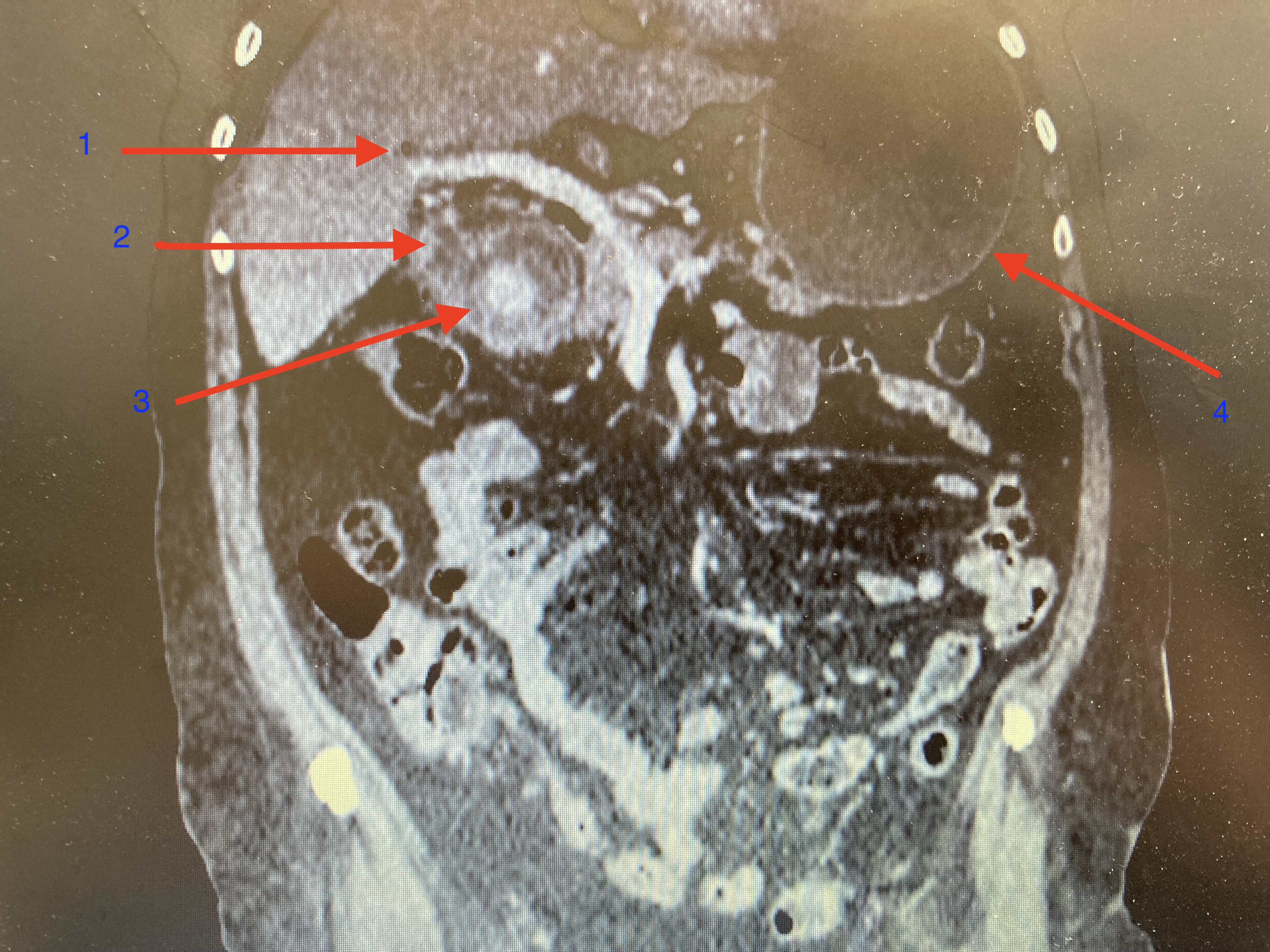
Initial computed tomography of the abdomen revealed typical bouveret syndrome with Rigler triad. 1) Pneumobilia 2) Collapse of gallbladder 3) Ectopic gallstone in the proximal duodenum, size more than 4cm 4) Distended stomach Contributed by Jasim Al-Musawi
(Click Image to Enlarge)
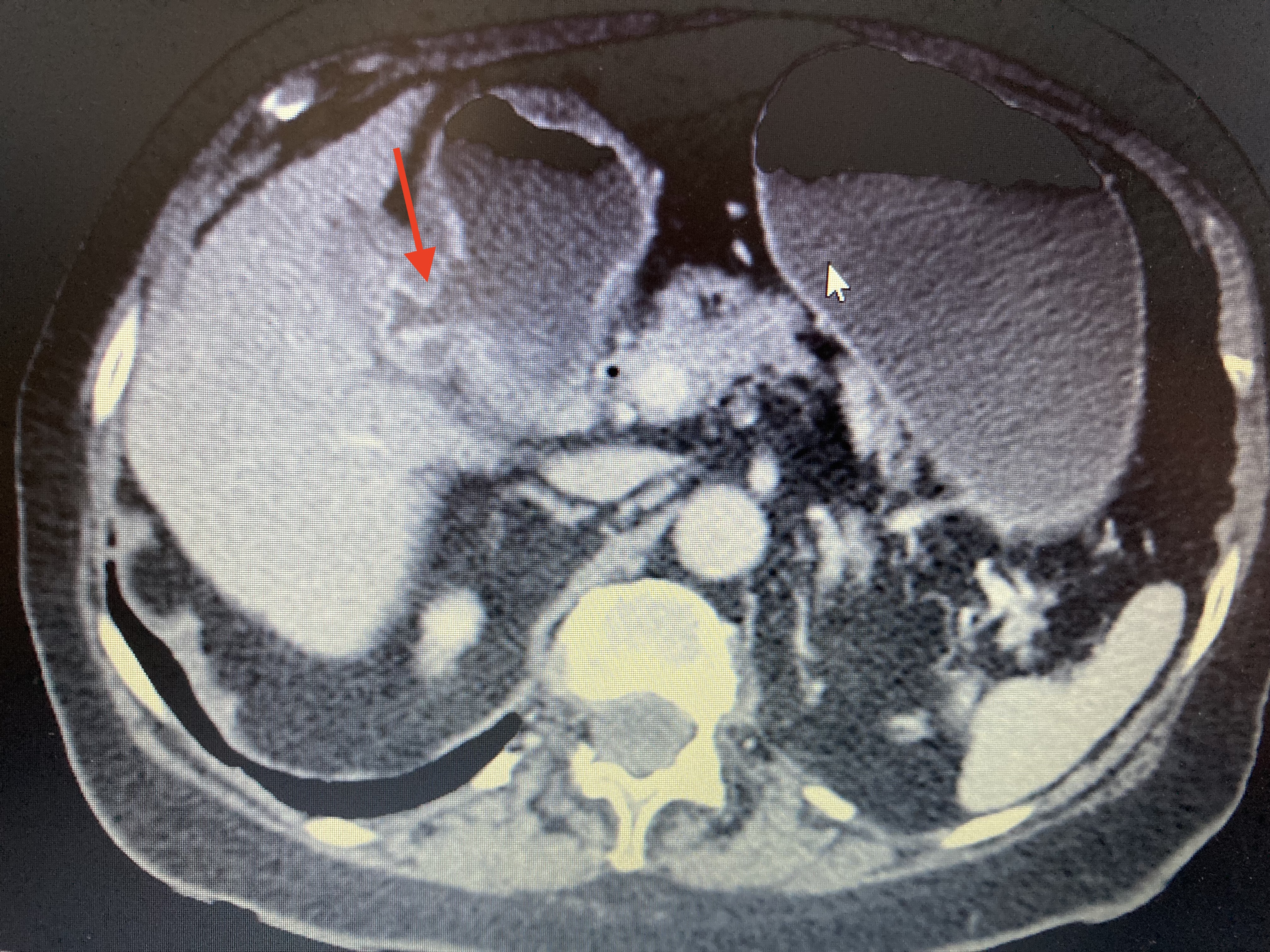
Computed tomography of the abdomen for a patient with Bouveret syndrome, showing a cholecystoduodenal fistula (shown by arrow). Contributed by Jasim Al-Musawi
(Click Image to Enlarge)
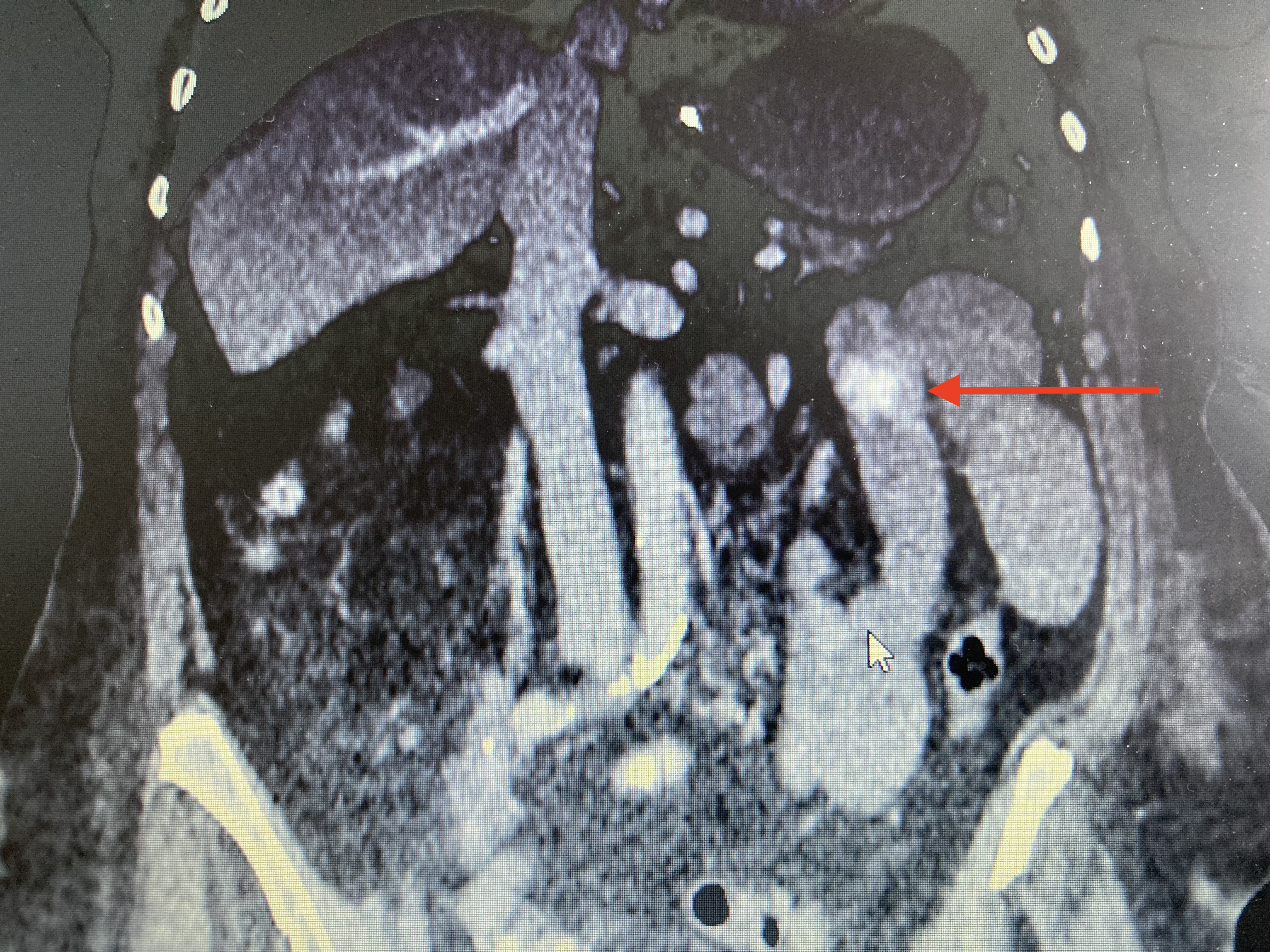
Computed tomography of the abdomen showing a migrated gallstone after endoscopic lithotripsy, causing gallstone ileus in the proximal jejunum. Contributed by Jasim Al-Musawi
(Click Video to Play)
References
Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. The American journal of gastroenterology. 2002 Feb:97(2):249-54 [PubMed PMID: 11866258]
Jin L, Naidu K. Bouveret syndrome-a rare form of gastric outlet obstruction. Journal of surgical case reports. 2021 May:2021(5):rjab183. doi: 10.1093/jscr/rjab183. Epub 2021 May 19 [PubMed PMID: 34040753]
Level 3 (low-level) evidenceLawther RE, Diamond T. Bouveret's syndrome: gallstone ileus causing gastric outlet obstruction. The Ulster medical journal. 2000 May:69(1):69-70 [PubMed PMID: 10881651]
Level 3 (low-level) evidenceHaddad FG, Mansour W, Deeb L. Bouveret's Syndrome: Literature Review. Cureus. 2018 Mar 10:10(3):e2299. doi: 10.7759/cureus.2299. Epub 2018 Mar 10 [PubMed PMID: 29755896]
Yılmaz EM, Cartı EB, Kandemir A. Rare cause of duodenal obstruction: Bouveret syndrome. Turkish journal of surgery. 2018 Aug 28:():1-3. doi: 10.5152/turkjsurg.2017.3794. Epub 2018 Aug 28 [PubMed PMID: 30216175]
Rodrigues ILM. Bouveret syndrome and its imaging diagnosis. Radiologia brasileira. 2018 Jul-Aug:51(4):276-277. doi: 10.1590/0100-3984.2016.0220. Epub [PubMed PMID: 30202139]
Haddad FG, Mansour W, Mansour J, Deeb L. From Bouveret's Syndrome to Gallstone Ileus: The Journey of a Migrating Stone! Cureus. 2018 Mar 26:10(3):e2370. doi: 10.7759/cureus.2370. Epub 2018 Mar 26 [PubMed PMID: 29805939]
Baharith H, Khan K. Bouveret syndrome: when there are no options. Canadian journal of gastroenterology & hepatology. 2015 Jan-Feb:29(1):17-8 [PubMed PMID: 25706571]
Level 3 (low-level) evidenceAyantunde AA, Agrawal A. Gallstone ileus: diagnosis and management. World journal of surgery. 2007 Jun:31(6):1292-7 [PubMed PMID: 17436117]
Level 2 (mid-level) evidenceWarren DJ, Peck RJ, Majeed AW. Bouveret's Syndrome: a Case Report. Journal of radiology case reports. 2008:2(4):14-7. doi: 10.3941/jrcr.v2i4.60. Epub 2008 Oct 1 [PubMed PMID: 22470599]
Level 3 (low-level) evidenceLanghorst J, Schumacher B, Deselaers T, Neuhaus H. Successful endoscopic therapy of a gastric outlet obstruction due to a gallstone with intracorporeal laser lithotripsy: a case of Bouveret's syndrome. Gastrointestinal endoscopy. 2000 Feb:51(2):209-13 [PubMed PMID: 10650271]
Level 3 (low-level) evidenceZissin R, Osadchy A, Klein E, Konikoff F. Consecutive instances of gallstone ileus due to obstruction first at the ileum and then at the duodenum complicating a gallbladder carcinoma: a case report. Emergency radiology. 2006 Mar:12(3):108-10 [PubMed PMID: 16362271]
Level 3 (low-level) evidenceShinoda M, Aiura K, Yamagishi Y, Masugi Y, Takano K, Maruyama S, Irino T, Takabayashi K, Hoshino Y, Nishiya S, Hibi T, Kawachi S, Tanabe M, Ueda M, Sakamoto M, Hibi T, Kitagawa Y. Bouveret's syndrome with a concomitant incidental T1 gallbladder cancer. Clinical journal of gastroenterology. 2010 Oct:3(5):248-53. doi: 10.1007/s12328-010-0170-0. Epub 2010 Sep 4 [PubMed PMID: 26190330]
Sharma D, Jakhetia A, Agarwal L, Baruah D, Rohtagi A, Kumar A. Carcinoma Gall Bladder with Bouveret's Syndrome: A Rare Cause of Gastric Outlet Obstruction. The Indian journal of surgery. 2010 Aug:72(4):350-1. doi: 10.1007/s12262-010-0145-x. Epub 2010 Nov 23 [PubMed PMID: 21938203]
Mavroeidis VK, Matthioudakis DI, Economou NK, Karanikas ID. Bouveret syndrome-the rarest variant of gallstone ileus: a case report and literature review. Case reports in surgery. 2013:2013():839370. doi: 10.1155/2013/839370. Epub 2013 Jun 24 [PubMed PMID: 23864977]
Level 3 (low-level) evidenceOsman K, Maselli D, Kendi AT, Larson M. Bouveret's syndrome and cholecystogastric fistula: a case-report and review of the literature. Clinical journal of gastroenterology. 2020 Aug:13(4):527-531. doi: 10.1007/s12328-020-01114-7. Epub 2020 Mar 30 [PubMed PMID: 32232771]
Level 3 (low-level) evidenceIancu C, Bodea R, Al Hajjar N, Todea-Iancu D, Bălă O, Acalovschi I. Bouveret syndrome associated with acute gangrenous cholecystitis. Journal of gastrointestinal and liver diseases : JGLD. 2008 Mar:17(1):87-90 [PubMed PMID: 18392252]
Level 3 (low-level) evidenceCappell MS, Davis M. Characterization of Bouveret's syndrome: a comprehensive review of 128 cases. The American journal of gastroenterology. 2006 Sep:101(9):2139-46 [PubMed PMID: 16817848]
Level 3 (low-level) evidenceAlibegovic E, Kurtcehajic A, Hujdurovic A, Mujagic S, Alibegovic J, Kurtcehajic D. Bouveret Syndrome or Gallstone Ileus. The American journal of medicine. 2018 Apr:131(4):e175. doi: 10.1016/j.amjmed.2017.10.044. Epub [PubMed PMID: 29555049]
Su HL, Tsai MJ. Bouveret syndrome. QJM : monthly journal of the Association of Physicians. 2018 Jul 1:111(7):489-490. doi: 10.1093/qjmed/hcy020. Epub [PubMed PMID: 29394400]
Di Re AM, Punch G, Richardson AJ, Pleass H. Rare case of Bouveret syndrome. ANZ journal of surgery. 2019 May:89(5):E198-E199. doi: 10.1111/ans.14215. Epub 2017 Oct 13 [PubMed PMID: 29027328]
Level 3 (low-level) evidenceYu YB, Song Y, Xu JB, Qi FZ. Bouveret's syndrome: A rare presentation of gastric outlet obstruction. Experimental and therapeutic medicine. 2019 Mar:17(3):1813-1816. doi: 10.3892/etm.2019.7150. Epub 2019 Jan 3 [PubMed PMID: 30783453]
Level 2 (mid-level) evidenceDumonceau JM, Devière J. Novel treatment options for Bouveret's syndrome: a comprehensive review of 61 cases of successful endoscopic treatment. Expert review of gastroenterology & hepatology. 2016 Nov:10(11):1245-1255 [PubMed PMID: 27677937]
Level 3 (low-level) evidenceIñíguez A, Butte JM, Zúñiga JM, Crovari F, Llanos O. [Bouveret syndrome: report of four cases]. Revista medica de Chile. 2008 Feb:136(2):163-8 [PubMed PMID: 18483669]
Level 3 (low-level) evidenceOng J, Swift C, Stokell BG, Ong S, Lucarelli P, Shankar A, Rouhani FJ, Al-Naeeb Y. Bouveret Syndrome: A Systematic Review of Endoscopic Therapy and a Novel Predictive Tool to Aid in Management. Journal of clinical gastroenterology. 2020 Oct:54(9):758-768. doi: 10.1097/MCG.0000000000001221. Epub [PubMed PMID: 32898384]
Level 1 (high-level) evidenceLowe AS, Stephenson S, Kay CL, May J. Duodenal obstruction by gallstones (Bouveret's syndrome): a review of the literature. Endoscopy. 2005 Jan:37(1):82-7 [PubMed PMID: 15657864]
Jindal A, Philips CA, Jamwal K, Sarin SK. Use of a Roth Net Platinum Universal Retriever for the endoscopic management of a large symptomatic gallstone causing Bouveret's syndrome. Endoscopy. 2016 Sep:48(S 01):E308 [PubMed PMID: 27669536]
Kaushik N, Moser AJ, Slivka A, Chandrupatala S, Martin JA. Gastric outlet obstruction caused by gallstones: case report and review of the literature. Digestive diseases and sciences. 2005 Mar:50(3):470-3 [PubMed PMID: 15810628]
Level 3 (low-level) evidenceBinmoeller KF, Brückner M, Thonke F, Soehendra N. Treatment of difficult bile duct stones using mechanical, electrohydraulic and extracorporeal shock wave lithotripsy. Endoscopy. 1993 Mar:25(3):201-6 [PubMed PMID: 8519238]
Kozarek RA, Low DE, Ball TJ. Tunable dye laser lithotripsy: in vitro studies and in vivo treatment of choledocholithiasis. Gastrointestinal endoscopy. 1988 Sep-Oct:34(5):418-21 [PubMed PMID: 2903114]
Level 3 (low-level) evidenceCotton PB, Kozarek RA, Schapiro RH, Nishioka NS, Kelsey PB, Ball TJ, Putnam WS, Barkun A, Weinerth J. Endoscopic laser lithotripsy of large bile duct stones. Gastroenterology. 1990 Oct:99(4):1128-33 [PubMed PMID: 1975549]
Lv S, Fang Z, Wang A, Yang J, Zhang W. Choledochoscopic Holmium Laser Lithotripsy for Difficult Bile Duct Stones. Journal of laparoendoscopic & advanced surgical techniques. Part A. 2017 Jan:27(1):24-27. doi: 10.1089/lap.2016.0289. Epub 2017 Jan 3 [PubMed PMID: 28048950]
Schatloff O, Rimon U, Garniek A, Lindner U, Morag R, Mor Y, Ramon J, Winkler H. Percutaneous transhepatic lithotripsy with the holmium: YAG laser for the treatment of refractory biliary lithiasis. Surgical laparoscopy, endoscopy & percutaneous techniques. 2009 Apr:19(2):106-9. doi: 10.1097/SLE.0b013e31819fa5d5. Epub [PubMed PMID: 19390274]
Alsolaiman MM, Reitz C, Nawras AT, Rodgers JB, Maliakkal BJ. Bouveret's syndrome complicated by distal gallstone ileus after laser lithotropsy using Holmium: YAG laser. BMC gastroenterology. 2002 Jun 18:2():15 [PubMed PMID: 12086587]
Level 3 (low-level) evidencePickhardt PJ, Friedland JA, Hruza DS, Fisher AJ. Case report. CT, MR cholangiopancreatography, and endoscopy findings in Bouveret's syndrome. AJR. American journal of roentgenology. 2003 Apr:180(4):1033-5 [PubMed PMID: 12646450]
Level 3 (low-level) evidenceRogart JN, Perkal M, Nagar A. Successful Multimodality Endoscopic Treatment of Gastric Outlet Obstruction Caused by an Impacted Gallstone (Bouveret's Syndrome). Diagnostic and therapeutic endoscopy. 2008:2008():471512. doi: 10.1155/2008/471512. Epub [PubMed PMID: 18493330]
Level 3 (low-level) evidenceASGE Technology Committee, Watson RR, Parsi MA, Aslanian HR, Goodman AJ, Lichtenstein DR, Melson J, Navaneethan U, Pannala R, Sethi A, Sullivan SA, Thosani NC, Trikudanathan G, Trindade AJ, Maple JT. Biliary and pancreatic lithotripsy devices. VideoGIE : an official video journal of the American Society for Gastrointestinal Endoscopy. 2018 Nov:3(11):329-338. doi: 10.1016/j.vgie.2018.07.010. Epub 2018 Sep 26 [PubMed PMID: 30402576]
Reinhardt SW, Jin LX, Pitt SC, Earl TM, Chapman WC, Doyle MB. Bouveret's syndrome complicated by classic gallstone ileus: progression of disease or iatrogenic? Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2013 Nov:17(11):2020-4. doi: 10.1007/s11605-013-2301-7. Epub 2013 Sep 10 [PubMed PMID: 24018589]
Level 3 (low-level) evidencePavlidis TE, Atmatzidis KS, Papaziogas BT, Papaziogas TB. Management of gallstone ileus. Journal of hepato-biliary-pancreatic surgery. 2003:10(4):299-302 [PubMed PMID: 14598150]
Gallego Otaegui L, Sainz Lete A, Gutiérrez Ríos RD, Alkorta Zuloaga M, Arteaga Martín X, Jiménez Agüero R, Medrano Gómez MÁ, Ruiz Montesinos I, Beguiristain Gómez A. A rare presentation of gallstones: Bouveret´s syndrome, a case report. Revista espanola de enfermedades digestivas. 2016 Jul:108(7):434-6 [PubMed PMID: 27659106]
Level 3 (low-level) evidenceStein PH, Lee C, Sejpal DV. A Rock and a Hard Place: Successful Combined Endoscopic and Surgical Treatment of Bouveret's Syndrome. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2015 Dec:13(13):A25-6. doi: 10.1016/j.cgh.2015.07.044. Epub 2015 Aug 5 [PubMed PMID: 26254202]
Thompson RJ, Gidwani A, Caddy G, McKenna E, McCallion K. Endoscopically assisted minimally invasive surgery for gallstones. Irish journal of medical science. 2009 Mar:178(1):85-7 [PubMed PMID: 17973154]
Level 3 (low-level) evidenceNewton RC, Loizides S, Penney N, Singh KK. Laparoscopic management of Bouveret syndrome. BMJ case reports. 2015 Apr 22:2015():. doi: 10.1136/bcr-2015-209869. Epub 2015 Apr 22 [PubMed PMID: 25903213]
Level 3 (low-level) evidenceYang D, Wang Z, Duan ZJ, Jin S. Laparoscopic treatment of an upper gastrointestinal obstruction due to Bouveret's syndrome. World journal of gastroenterology. 2013 Oct 28:19(40):6943-6. doi: 10.3748/wjg.v19.i40.6943. Epub [PubMed PMID: 24187475]
Level 3 (low-level) evidenceBalakrishnan S, Samdani T, Singhal T, Hussain A, Grandy-Smith S, Nicholls J, El-Hasani S. Patient experience with gallstone disease in a national health service district hospital. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2008 Oct-Dec:12(4):389-94 [PubMed PMID: 19275855]
Hussain A. Difficult laparoscopic cholecystectomy: current evidence and strategies of management. Surgical laparoscopy, endoscopy & percutaneous techniques. 2011 Aug:21(4):211-7. doi: 10.1097/SLE.0b013e318220f1b1. Epub [PubMed PMID: 21857467]
Jafferbhoy S, Rustum Q, Shiwani M. Bouveret's syndrome: should we remove the gall bladder? BMJ case reports. 2011 Apr 1:2011():. doi: 10.1136/bcr.02.2011.3891. Epub 2011 Apr 1 [PubMed PMID: 22700609]
Level 3 (low-level) evidenceLee W, Han SS, Lee SD, Kim YK, Kim SH, Woo SM, Lee WJ, Koh YW, Hong EK, Park SJ. Bouveret's syndrome: a case report and a review of the literature. Korean journal of hepato-biliary-pancreatic surgery. 2012 May:16(2):84-7. doi: 10.14701/kjhbps.2012.16.2.84. Epub 2012 May 31 [PubMed PMID: 26388913]
Level 3 (low-level) evidenceLopes CV, Lima FK, Hartmann AA. Bouveret syndrome and pancreatic acinar cell carcinoma. Endoscopy. 2017 Feb:49(S 01):E62-E63. doi: 10.1055/s-0042-123499. Epub 2017 Jan 30 [PubMed PMID: 28135730]
Alemi F, Seiser N, Ayloo S. Gallstone Disease: Cholecystitis, Mirizzi Syndrome, Bouveret Syndrome, Gallstone Ileus. The Surgical clinics of North America. 2019 Apr:99(2):231-244. doi: 10.1016/j.suc.2018.12.006. Epub [PubMed PMID: 30846032]
Ploneda-Valencia CF, Gallo-Morales M, Rinchon C, Navarro-Muñiz E, Bautista-López CA, de la Cerda-Trujillo LF, Rea-Azpeitia LA, López-Lizarraga CR. Gallstone ileus: An overview of the literature. Revista de gastroenterologia de Mexico. 2017 Jul-Sep:82(3):248-254. doi: 10.1016/j.rgmx.2016.07.006. Epub 2017 Apr 19 [PubMed PMID: 28433486]
Level 3 (low-level) evidenceSaldaña Dueñas C, Fernández-Urien I, Rullán Iriarte M, Vila Costa JJ. Laser lithotripsy resolution for Bouveret syndrome. Endoscopy. 2017 Feb:49(S 01):E101-E102. doi: 10.1055/s-0043-102178. Epub 2017 Feb 13 [PubMed PMID: 28192808]
Bhattarai M, Bansal P, Patel B, Lalos A. Exploring the Diagnosis and Management of Bouveret's Syndrome. JNMA; journal of the Nepal Medical Association. 2016 Jan-Mar:54(201):33-35 [PubMed PMID: 27935909]