Definition/Introduction
A wound forms when biological tissues like skin, mucous membranes, and organs are damaged. Different injuries can cause wounds; properly cleaning and dressing the wounds is essential to prevent infections and additional harm.[1][2] The surgical wound classification (SWC) system was initially developed in 1964 by the National Academy of Sciences and the National Research Council. The SWC system was created to represent the bacterial load in a surgical field. The Centers for Disease Control and Prevention (CDC) later refined this system by establishing 4 different classes of wound statuses outlined below.[3] Each class has a postoperative risk of a surgical site infection (SSI) with scores of 1% to 5%, 3% to 11%, 10% to 17%, and more than 27%, respectively.[4]
- Class 1 wounds are categorized as clean wounds. These types of wounds are not infected, do not exhibit any signs of inflammation, and are typically closed. If drainage is required, a closed draining approach is recommended. It is worth noting that Class 1 wounds do not involve the respiratory, alimentary, genital, or urinary tracts. Examples of clean wounds include an inguinal hernia repair or a thyroidectomy.
- Class 2 wounds are categorized as clean-contaminated, which means they have a low level of contamination. These types of wounds involve entry into the respiratory, alimentary, genital, or urinary tracts but only under controlled circumstances.
- Class 3 wounds are classified as contaminated and typically result from a breach in sterile techniques or leakage from the gastrointestinal tract. Incisions resulting from acute or nonpurulent inflammation are also considered Class 3 wounds.
- Class 4 wounds are considered to be dirty or infected. These injuries usually occur from inadequate treatment of traumatic wounds, gross purulence, and evident infections. When tissues lose vitality, it can lead to Class 4 wounds. This is often caused by surgery or microorganisms found in perforated organs.[3]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
One of the major concerns about the SWC system is its low inter-rater reliability among healthcare professionals.[3][5] A study across multiple medical centers examined the discrepancy between the information documented by circulating operative room nurses during surgeries and the postoperative diagnosis. The findings highlighted a frequent discordance in wound classification, and the extent of the discrepancy varied based on the institution and type of operation. The difference was more common in unclean cases as compared to clean procedures.[6] The significance of this concept is amplified by the fact that clean wounds are unlikely to be over-classified, and the dirtiest wounds are unlikely to be under-classified.[4]
The process of wound classification is intricate and can be influenced by many factors.[7][4] Additionally, this generalized wound classification scheme has proved ineffective within various subspecialties, including trauma orthopedic surgical and neonatal surgical wounds.[8][9] This highlights the importance of wound classification systems specific to each medical specialty. These systems can effectively categorize wounds based on injury severity, location, and patient comorbidities.[9] The SWC system was established when all surgical procedures were conducted openly. With the increasing number of laparoscopic procedures, it is necessary to consider the impact when determining the classification of wounds. [10]
Clinical Significance
The clinical significance of proper wound classification lies in its ability to help predict the likelihood of surgical site infections, postoperative complications, and reoperation.[11] Correctly classified wounds can potentially aid in assessing morbidity, mortality, and quality of life.[12] Patients receiving grafts can also benefit from this classification scheme because it helps to evaluate the degree of bacterial contamination upon grafting and, by extension, the ability of the graft to heal correctly.[13] When it comes to determining surgical site infections, SWC is an essential factor. These infections are crucial quality indicators universally used in healthcare systems. [6][10]
Although there have been significant improvements in surgical sterility techniques to reduce the incidence of surgical site infections, the problem remains and may never be eradicated. However, identifying and understanding the risk factors associated with SSIs can help minimize the potential for infection. Not only are SSIs expensive, but they also have an increased morbidity risk. Risk factors can be exogenous (ie, surgical personnel or technique) or intrinsic (ie, chlorhexidine bath wipes or methicillin-resistant Staphylococcus aureus contamination). Blood loss, case urgency, case duration, type of anesthesia used, resident participation, and the performance of higher-risk procedures (ie, colon surgery and hysterectomy) are other factors contributing to the risk of infection.[14]
A common misconception is that the human body is sterile, but in reality, infections can occur due to a complex interplay among the host, potential pathogens, and the environment. When a microorganism manages to overcome the host's defenses, it can cause harm to the body. The infection process is not yet fully understood, and it is influenced by factors such as the microorganism's pathogenicity and virulence, as well as the host's immunocompetence. On the other hand, not all host-pathogen interactions lead to disease, and it's essential to establish new terms and definitions to understand these interactions better. While microbiological evaluation alone is usually insufficient for diagnosing infections, a thorough patient assessment is critical. Additionally, different wounds can support diverse communities of microorganisms, and the acquisition of microbial species can result in contamination, colonization, or infection. It is worth noting that colonization is not always synonymous with infection. [15]
Nursing, Allied Health, and Interprofessional Team Interventions
Studies have shown that prioritizing wound classifications in a curriculum can lead to a notable improvement in the accurate documentation of wound classifications.[4] Recently, the Association of periOperative Nurses (AORN) analyzed how surgical wound classification can be enhanced through surveys. The association found that limited resources and poor communication with surgeons were the factors causing discrepancies between nursing and surgeon documentation. To address this issue, AORN introduced a reference tool in the electronic health record, which significantly decreased documentation discrepancy, bringing it down to approximately 13%.[16]
Nursing, Allied Health, and Interprofessional Team Monitoring
Accurately classifying wounds and managing them appropriately is crucial for healthcare teams. This will provide optimal patient-centered care and improve the quality of life while avoiding infections and additional trauma to the wound.[15]
Media
(Click Image to Enlarge)
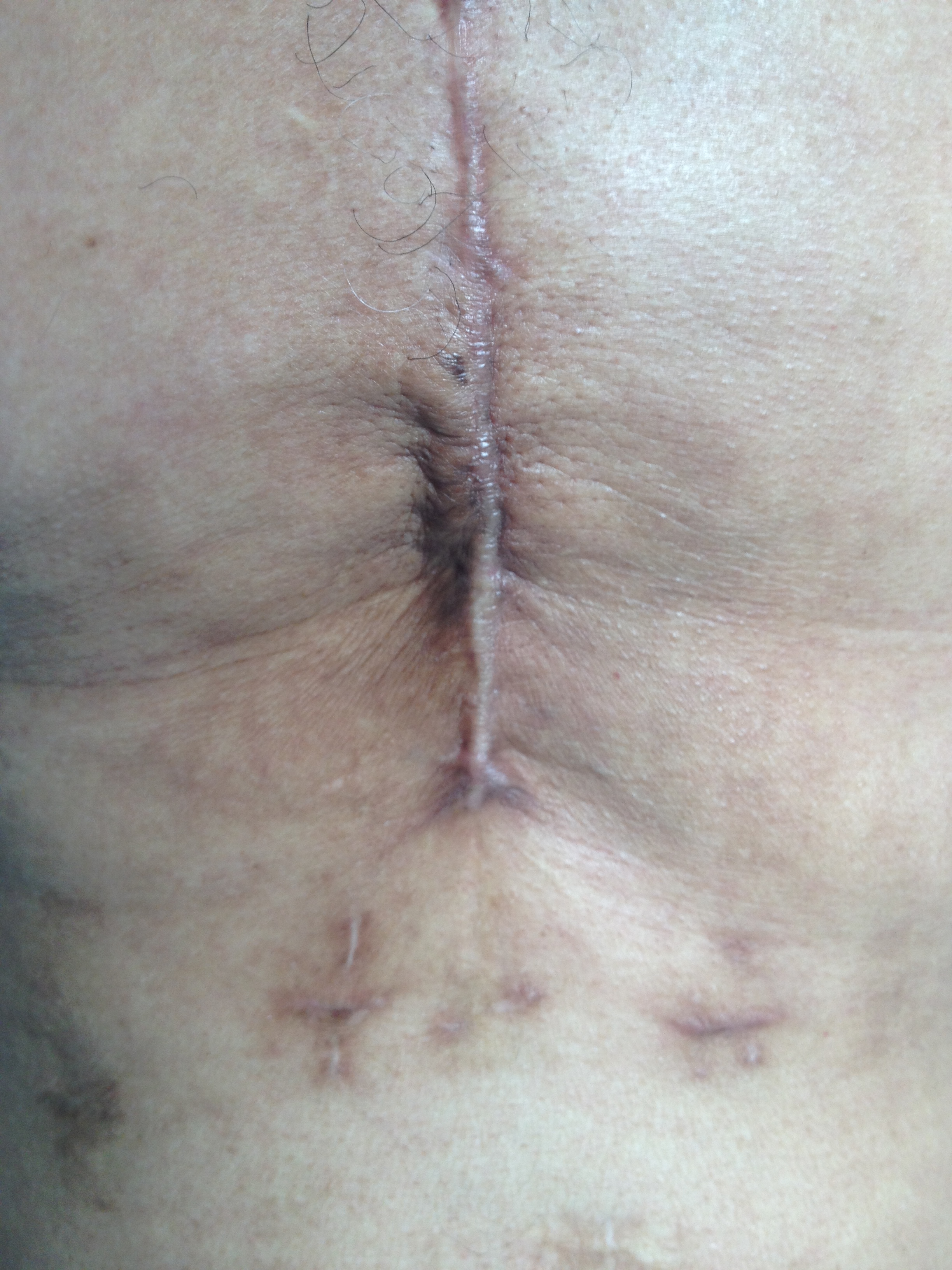
The photo shows a previous sternotomy; the wound has healed and is not infected, but shows a possible evolution in a hypertrophic scar. Contributed by Bruno Bordoni, PhD.
References
Kujath P, Michelsen A. Wounds - from physiology to wound dressing. Deutsches Arzteblatt international. 2008 Mar:105(13):239-48. doi: 10.3238/arztebl.2008.0239. Epub 2008 Mar 28 [PubMed PMID: 19629204]
Wilkins RG, Unverdorben M. Wound cleaning and wound healing: a concise review. Advances in skin & wound care. 2013 Apr:26(4):160-3. doi: 10.1097/01.ASW.0000428861.26671.41. Epub [PubMed PMID: 23507692]
Level 3 (low-level) evidenceOnyekwelu I, Yakkanti R, Protzer L, Pinkston CM, Tucker C, Seligson D. Surgical Wound Classification and Surgical Site Infections in the Orthopaedic Patient. Journal of the American Academy of Orthopaedic Surgeons. Global research & reviews. 2017 Jun:1(3):e022. doi: 10.5435/JAAOSGlobal-D-17-00022. Epub 2017 Jun 13 [PubMed PMID: 30211353]
Gorvetzian JW, Epler KE, Schrader S, Romero JM, Schrader R, Greenbaum A, McKee R. Operating room staff and surgeon documentation curriculum improves wound classification accuracy. Heliyon. 2018 Aug:4(8):e00728. doi: 10.1016/j.heliyon.2018.e00728. Epub 2018 Aug 8 [PubMed PMID: 30109278]
Levy SM, Holzmann-Pazgal G, Lally KP, Davis K, Kao LS, Tsao K. Quality check of a quality measure: surgical wound classification discrepancies impact risk-stratified surgical site infection rates in pediatric appendicitis. Journal of the American College of Surgeons. 2013 Dec:217(6):969-73. doi: 10.1016/j.jamcollsurg.2013.07.398. Epub 2013 Sep 13 [PubMed PMID: 24041560]
Level 2 (mid-level) evidenceLevy SM, Lally KP, Blakely ML, Calkins CM, Dassinger MS, Duggan E, Huang EY, Kawaguchi AL, Lopez ME, Russell RT, St Peter SD, Streck CJ, Vogel AM, Tsao K, Pediatric Surgery Research Collaborative. Surgical wound misclassification: a multicenter evaluation. Journal of the American College of Surgeons. 2015 Mar:220(3):323-9. doi: 10.1016/j.jamcollsurg.2014.11.007. Epub 2014 Nov 20 [PubMed PMID: 25532617]
Level 2 (mid-level) evidenceTsao K. Surgical Wound Misclassification: A Multicenter Evaluation: In Reply to Dodds and Dodds. Journal of the American College of Surgeons. 2015 Sep:221(3):781-2. doi: 10.1016/j.jamcollsurg.2015.06.005. Epub [PubMed PMID: 26296687]
Vu LT, Nobuhara KK, Lee H, Farmer DL. Conflicts in wound classification of neonatal operations. Journal of pediatric surgery. 2009 Jun:44(6):1206-11. doi: 10.1016/j.jpedsurg.2009.02.026. Epub [PubMed PMID: 19524742]
Level 2 (mid-level) evidenceScolaro JA, Agel J, Marmor M, Dumpe J, Karam M, Kellam J, Meinberg E, Munz J, Nguyen M, Soles G, Stinner D, Marecek GS. Adaptation of the Centers for Disease Control Surgical Wound Classification System for Orthopaedic Trauma Surgery. Journal of orthopaedic trauma. 2022 May 1:36(5):219-223. doi: 10.1097/BOT.0000000000002269. Epub [PubMed PMID: 35588171]
Oyetunji TA, Gonzalez DO, Gonzalez KW, Nwomeh BC, St Peter SD. Wound classification in pediatric surgical procedures: Measured and found wanting. Journal of pediatric surgery. 2016 Jun:51(6):1014-6. doi: 10.1016/j.jpedsurg.2016.02.070. Epub 2016 Mar 2 [PubMed PMID: 26996591]
Mioton LM, Jordan SW, Hanwright PJ, Bilimoria KY, Kim JY. The Relationship between Preoperative Wound Classification and Postoperative Infection: A Multi-Institutional Analysis of 15,289 Patients. Archives of plastic surgery. 2013 Sep:40(5):522-9. doi: 10.5999/aps.2013.40.5.522. Epub 2013 Sep 13 [PubMed PMID: 24086804]
Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. The impact of surgical-site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infection control and hospital epidemiology. 2002 Apr:23(4):183-9 [PubMed PMID: 12002232]
Level 2 (mid-level) evidenceHarth KC, Blatnik JA, Anderson JM, Jacobs MR, Zeinali F, Rosen MJ. Effect of surgical wound classification on biologic graft performance in complex hernia repair: an experimental study. Surgery. 2013 Apr:153(4):481-92. doi: 10.1016/j.surg.2012.08.064. Epub 2012 Dec 4 [PubMed PMID: 23218885]
Level 3 (low-level) evidenceWaltz PK, Zuckerbraun BS. Surgical Site Infections and Associated Operative Characteristics. Surgical infections. 2017 May/Jun:18(4):447-450. doi: 10.1089/sur.2017.062. Epub 2017 Apr 27 [PubMed PMID: 28448197]
Negut I, Grumezescu V, Grumezescu AM. Treatment Strategies for Infected Wounds. Molecules (Basel, Switzerland). 2018 Sep 18:23(9):. doi: 10.3390/molecules23092392. Epub 2018 Sep 18 [PubMed PMID: 30231567]
. Improving the accuracy of surgical wound classification documentation. AORN journal. 2021 Dec:114(6):P10-P12. doi: 10.1002/aorn.13581. Epub [PubMed PMID: 34846746]