Introduction
Asteroid hyalosis (AH) is characterized by yellow-white brilliant reflecting particles surrounded by tightly adherent fibrils inside the vitreous cavity.[1] These particles are known as asteroid bodies (ABs) due to their resemblance to stars (asteroids) in the night sky. AH was initially called "asteroid hyalitis" by Benson in 1894. However, in the absence of inflammation, the term asteroid hyalosis was introduced later. "Scintillatio albescens or 'nivea" is a term used to describe this entity and was introduced by Wiegmann in 1918. AH is a benign vitreous opacification that does not generally need active intervention. However, accurate clinical diagnosis, the study of the associated ophthalmic and systemic features, pathogenesis, and biochemical composition of AH merit discussion.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The exact etiology of asteroid hyalosis is unknown.
Epidemiology
The prevalence of asteroid hyalosis in the adult population is found to be 0.8% to 2.0% in different studies. This has been reported to be 0.8% from a retrospective chart review, 1.2% from fundus photography in the Beaver Dam Eye Study, and 2% from the pathological examination of autopsy specimens.[2][3][4] The prevalence increases with age. Studies based on autopsy specimens documented it to be 3.2% and 6.6% in the age group from 61 to 70 years and more than 91 years, respectively.[4] AH is unilateral in 75 to 90% of cases.[4] There is no racial predisposition. Few studies have mentioned the male-to-female ratio to be 2 to 1.[4] However, one large study did not find any gender predisposition.[2] AH is not heritable, and familial cases are reported rarely.
Pathophysiology
The etiology of asteroid hyalosis remains to be elucidated. Voerhoeff postulated that angiosclerosis of intraocular vessels, along with local deposition of lipids and fats, leads to AH formation. Rodman described type 1 AH in normal vitreous and type 2 AH in vitreous with associated inflammation.[5] Streeten suggested that ABs are produced from exogenous sources since the contents are not present in sufficient quantity in the normal vitreous.[6] Bergren et al. suggested that the release of phospholipid and calcium from degenerated retinal cells could produce AH.[2] Gass observed that AH initially develops near retinal blood vessels. Zauberman and Livni demonstrated the formation of asteroid bodies in the vitreous of albino rats in conjunction with hypercholesterolemia and closure of vertex veins.[7] However, these findings were not replicable by others.
The unilateral occurrence of asteroid hyalosis can be postulated by the contribution from various factors, eg., local inflammation, retinal pigment epithelial degeneration, local changes in pH, vitreous collagen degeneration, and most notably, increased retinal vascular permeability altering the calcium and lipid levels of the vitreous. However, the exact etiology remains to be proved.
Histopathology
The structure and composition of ABs have been studied in various studies using biochemical methods, light, or electron microscopy. Calcium-associated phospholipids are proposed to be the major components of ABs based upon the findings like elemental detection of calcium and phosphorus using energy-dispersive x-ray spectroscopy (EDX) analysis and the intense reaction of ABs with lipid statins.[8]
Feldman et al. in 1967 used thin layer and gas chromatography to reveal the composition of ABs to be sphingomyelin, ceramide dihexoside, cholesterol, cerebroside, cholesteryl esters, with trace quantities of triglyceride and lecithin.[9]
March and Shoch, in 1975, utilized the X-ray microanalyzer to show that phosphate, probably as apatite, was a major constituent of ABs.[10]
Streeten, in 1982, did an ultrastructural analysis of vitreous and found that large ABs were composed of intertwined ribbons of multilaminar membranes with a 6-nm periodicity characteristic of complex lipids, especially phospholipids, lying in a homogeneous background matrix.[6] This finding was supported by Topilow et al. using transmission electron microscopy.[11] Streeten also found that small ABs featured lipid ribbons resulting from the deposition of successive lipid layers on the thin membranes, resulting in variable degrees of civilization.[6]
Winkler and Lunsdorf, in 2001, used electron energy loss spectroscopy (EELS) and energy-filtered transmission electron microscopy (EFTEM) to reveal that asteroid hyalosis is composed of calcium, phosphorus, and oxygen with an elemental similarity to hydroxyapatite. Using fast Fourier transform analysis, these investigators revealed that a fine, parallel-oriented line divides each 7-nm periodicity of asteroid lamellar stacks, separating each 7-nm layer into two halves of 3.5-nm thickness.[8]
Komatsu et al. 2003, did a chemical analysis of vitreous fluid with an energy-dispersive X-ray microanalyzer and reconstructive studies of hydroxylapatite in simulated body fluid. ABs appeared as "snowballs" under the scanning electron microscope covered with the clotted matrix of vitreous substances superficial to a pumice stone-like structure. They inferred that AH was produced not only by changes in ionic tension but also by changes in the vitreous extracellular matrix during aging and disease.[12]
Lin and colleagues in 2007 identified carotene by confocal micro-Raman spectroscopy, which was verified by high-performance liquid chromatography (HPLC).[13]
History and Physical
Systemic diseases like diabetes mellitus (DM), systemic hypertension, and hyperlipidemia have been associated with asteroid hyalosis, but controversies do exist. A study by Smith et al. found 70% of patients with AH had DM according to a glucose tolerance test, but the absence of a control group was the limitation of the study. Luxenberg and Sime, in a clinic-based study, reported no difference in the prevalence rate of AH in DM and control groups.[14] In 1991, Bergren et al. did a large study involving 12205 patients, out of which 29% of the 101 AH patients had a history of DM in comparison to 10% of 101 controls.[2] The difference was statistically significant (P=0.00007). However, Fawzi AA et al., in their study involving 10801 autopsy eyes, did not find any significant association with DM.[4] The unilateral occurrence of AH in the setting of systemic disease like DM questions its significant association. Similarly, an association of AH with other diseases like hypertension, atherosclerosis, and hyperlipidemia failed to be reproducible in large population-based studies. Hypercholesterolemia, elevated serum calcium levels, and gout are described to be associated with AH in small studies.[14][15]
Evaluation
Patients with asteroid hyalosis are usually asymptomatic, and this condition is mostly diagnosed during the routine ophthalmic examination.[16] In eyes with AH, only a small proportion of light gets scattered, and the smooth surface of the ABs results in the minimal scattering of light. ABs may be visually symptomatic when they are sufficiently closer to the macula or when a complete posterior vitreous detachment causes the particles to be concentrated behind the lens. These unusual cases may need vitrectomy.
Ophthalmic Evaluation
By ophthalmoscopy, ABs are small round refractile opacities associated with vitreous strands and suspended in the vitreous cavity. They move along with the movement of the vitreous body and get back to their previous position after the movement stops. (Supplementary video) However, they do not settle with gravity. The size of these particles is found to be 3 to 100 microns.[11] During ophthalmoscopy, the reflected light from these particles returns to the examiner and confounds the view. There occurs less reflection of light indirect ophthalmoscopy than in slit-lamp biomicroscopy with a 90 diopter lens or indirect ophthalmoscopy with a 20 diopter lens. So, direct ophthalmoscopy gives a relatively better view of the fundus in AH. The presence of AH in diabetic retinopathy eyes warrants fundus fluorescein angiography (FFA), especially in eyes with suspected neovascularisations.[17] With the advent of wide-angle FFA, not only neovascularisations but also peripheral lesions e.g., malignancies, can be detected.[18] Optical coherence tomography angiography (OCTA) is being increasingly used as an alternative to FFA, and there are reports of its utility in detecting lesions in diabetic retinopathy.[19] Widefield fundus autofluorescence images are found to be helpful for the accurate localization of laser scars in the presence of AH.[20] Optical coherence tomography (OCT) helps in the study of the vitreoretinal interface in these eyes.[21] AH may induce media opacity during OCT scanning of the retina, and Swept source-OCT has superior diagnostic capabilities compared to SD-OCT in these settings.[22] B scan helps in the diagnosis of AH by the presence of moderate to high amplitude point spikes in the vitreous cavity separated by a clear zone from the retinal surface.[23] Recently, Reports of multicolor imaging of the fundus has been reported to be a preferred modality to detect retinal lesions that are difficult to be detected in color fundus photography.[24]
An intact vitreoretinal interface without posterior vitreous detachment is found more often in AH.[4][11] Studies have postulated that the attached posterior vitreous may be responsible for the formation of ABs.[2] AH is seen less often in myopic eyes than in hyperopic eyes.[2] There is a report of less frequent retinal detachment in eyes with AH. Other ophthalmic associations like retinitis pigmentosa, uveal melanoma, and pre-Descemet dystrophy have been less frequently reported in the literature.[25][26][27][28]
Treatment / Management
Since asteroid hyalosis is most often asymptomatic, it needs observation only.[16][29] However, care should be taken not to miss any other significant fundus pathology in the context of a difficult fundoscopy. The presence of neovascularization in eyes with AH and DR can be detected with FFA.[17][20] OCT is useful to detect any vitreoretinal surface anomaly, and B scan can be helpful to detect any mass lesion obscured by the ABs.[21][23](B3)
Cataract surgery in the presence of AH
Cataract surgery in the presence of AH may pose certain issues of which the surgeon must be aware.[30][31](B3)
- A scan may show falsely short axial length due to confusing echoes from ABs. A comparison with the axial length of the fellow eye may be helpful.
- Reflections from the ABs can cause an impaired view of the posterior capsule.
- Silicone intraocular lenses should be avoided due to possible deposition of calcium and phosphorus content of ABs over the posterior lens surface.
Though there are reports of successful removal of calcium deposits from the surface of silicon IOLs in the presence of AH by laser capsulotomy and pars plana vitrectomy, IOL exchange remains the preferred treatment of choice in these settings.[32][33][34](B3)
There are certain scenarios where vitrectomy is needed in AH.[35][36][37][38](B3)
- Poor visualization of fundus and failure of imaging modalities like FFA, OCT and B scan to detect the cause of visual symptoms
- Inability to perform laser photocoagulation especially in a case of DR
- Inability to find retinal breaks in the presence of a rhegmatogenous retinal detachment
- Visual symptoms e.g., floaters or visual decline (rarely)
Differential Diagnosis
Asteroid hyalosis needs to be differentiated from similar appearing fundus pathology, e.g., synchysis scintillans, amyloidosis, vitritis, old vitreous hemorrhage, and malignancy, particularly lymphoma and masquerade syndromes. Synchysis scintillans or cholesterolosis bulbi occurs in end-stage eyes or with eyes with a degenerative disease and characterized by cholesterol crystal deposits freely floating and then settling in liquefied vitreous. Vitreous amyloidosis is mostly bilateral, visually symptomatic, and histopathology of vitreous samples is confirmatory in these cases. Vitritis patients have defective vision and other associated features like clinical history, pain, redness, etc. pointing towards inflammation. Vitreous hemorrhages should prompt to look for retinal vascular pathologies, retinal breaks, or associated features of trauma. Malignancies like lymphoma can be diagnosed by histopathology of the vitreous sample. However, AH mimicking vitreous seeds in a patient with retinoblastoma (RB) needs to be properly diagnosed, and protocol for the management of RB should be followed.[39]
Prognosis
Asteroid hyalosis is most often asymptomatic, and hence prognosis is good. However, in the presence of other ophthalmic comorbidities like diabetic retinopathy, the prognosis depends upon the associated diseases. Similarly, the presence of AH in situations like retinal detachment without an identifiable break, symptomatic floaters, etc., warrants vitrectomy, and the prognosis depend upon these associated diseases. Special care during biometry to avoid wrong intraocular lens power calculation helps in better prognosis in eyes with AH undergoing cataract surgery.
Complications
Asteroid hyalosis is benign and does not cause any complications. However, some cases may develop dense AH and cause troublesome floaters, which may need vitrectomy. The presence of AH in the anterior vitreous face may cause intraoperative reflections during cataract surgery, and hence awareness about this effect will help the surgeon avoid intraoperative complications.
Deterrence and Patient Education
Patients with diabetes mellitus and asteroid hyalosis should be informed of the need for fundus fluorescein angiography in case of doubtful neovascularisation in the retina for early identification and management of proliferative diabetic retinopathy.
Enhancing Healthcare Team Outcomes
The diagnosis and management of asteroid hyalosis are essential. The possible associations like diabetes, hypertension, and hyperlipidemia, when present, should be managed by interprofessional team communication with endocrinologists and general physicians. The team can also include optometrists, ophthalmologists, ophthalmology nurses, and operating room nurses. The nurses participate in patient education and follow-up, informing the ophthalmologist of any issues. [Level 5]
Media
(Click Video to Play)
(Click Image to Enlarge)
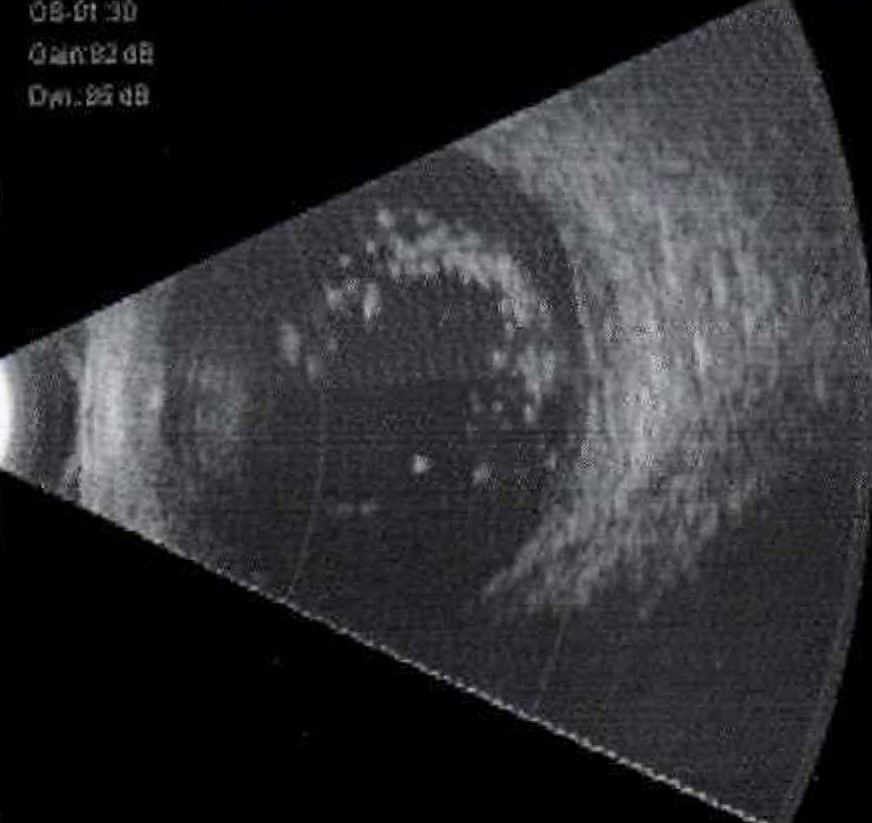
Ultrasound B-Scan image of an eye with asteroid hyalosis. Please note the dot echoes in the vitreous cavity and a clear zone between the dot echoes and the retina. Contributed by Dr Chitaranjan Mishra, DNB, FICO, MRCS, Aravind Eye Hospital, Madurai.
References
Tripathy K. Asteroid Hyalosis. The New England journal of medicine. 2018 Aug 23:379(8):e12. doi: 10.1056/NEJMicm1712355. Epub [PubMed PMID: 30134134]
Bergren RL, Brown GC, Duker JS. Prevalence and association of asteroid hyalosis with systemic diseases. American journal of ophthalmology. 1991 Mar 15:111(3):289-93 [PubMed PMID: 2000898]
Moss SE, Klein R, Klein BE. Asteroid hyalosis in a population: the Beaver Dam eye study. American journal of ophthalmology. 2001 Jul:132(1):70-5 [PubMed PMID: 11438056]
Fawzi AA, Vo B, Kriwanek R, Ramkumar HL, Cha C, Carts A, Heckenlively JR, Foos RY, Glasgow BJ. Asteroid hyalosis in an autopsy population: The University of California at Los Angeles (UCLA) experience. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Apr:123(4):486-90 [PubMed PMID: 15824221]
Level 2 (mid-level) evidenceRODMAN HI, JOHNSON FB, ZIMMERMAN LE. New histo-pathological and histochemical observations concerning asteroid hyalitis. Archives of ophthalmology (Chicago, Ill. : 1960). 1961 Oct:66():552-63 [PubMed PMID: 14493131]
Streeten BW. Vitreous asteroid bodies. Ultrastructural characteristics and composition. Archives of ophthalmology (Chicago, Ill. : 1960). 1982 Jun:100(6):969-75 [PubMed PMID: 7092637]
Zauberman H, Livni N. Experimental vascular occlusion in hypercholesterolemic rabbits. Investigative ophthalmology & visual science. 1981 Aug:21(2):248-55 [PubMed PMID: 7251308]
Level 3 (low-level) evidenceWinkler J, Lünsdorf H. Ultrastructure and composition of asteroid bodies. Investigative ophthalmology & visual science. 2001 Apr:42(5):902-7 [PubMed PMID: 11274065]
Feldman GL. Human ocular lipids: their analysis and distribution. Survey of ophthalmology. 1967 Jun:12(3):207-43 [PubMed PMID: 4867603]
Level 3 (low-level) evidenceMarch WF, Shoch D. Electron diffraction study of asteroid bodies. Investigative ophthalmology. 1975 May:14(5):399-400 [PubMed PMID: 165161]
Topilow HW, Kenyon KR, Takahashi M, Freeman HM, Tolentino FI, Hanninen LA. Asteroid hyalosis. Biomicroscopy, ultrastructure, and composition. Archives of ophthalmology (Chicago, Ill. : 1960). 1982 Jun:100(6):964-8 [PubMed PMID: 7092636]
Level 3 (low-level) evidenceKomatsu H, Kamura Y, Ishi K, Kashima Y. Fine structure and morphogenesis of asteroid hyalosis. Medical electron microscopy : official journal of the Clinical Electron Microscopy Society of Japan. 2003 Jun:36(2):112-9 [PubMed PMID: 12825125]
Level 3 (low-level) evidenceLin SY,Chen KH,Cheng WT,Ho CT,Wang SL, Preliminary identification of Beta-carotene in the vitreous asteroid bodies by micro-Raman spectroscopy and HPLC analysis. Microscopy and microanalysis : the official journal of Microscopy Society of America, Microbeam Analysis Society, Microscopical Society of Canada. 2007 Apr; [PubMed PMID: 17367552]
Level 3 (low-level) evidenceLuxenberg M, Sime D. Relationship of asteroid hyalosis to diabetes mellitus and plasma lipid levels. American journal of ophthalmology. 1969 Mar:67(3):406-13 [PubMed PMID: 5774257]
Safir A, Dunn SN, Martin RG, Tate GW, Mincey GJ. Is asteroid hyalosis ocular gout? Annals of ophthalmology. 1990 Feb:22(2):70-7 [PubMed PMID: 2316956]
Khoshnevis M, Rosen S, Sebag J. Asteroid hyalosis-a comprehensive review. Survey of ophthalmology. 2019 Jul-Aug:64(4):452-462. doi: 10.1016/j.survophthal.2019.01.008. Epub 2019 Jan 30 [PubMed PMID: 30707924]
Level 3 (low-level) evidenceHampton GR, Nelsen PT, Hay PB. Viewing through the asteroids. Ophthalmology. 1981 Jul:88(7):669-72 [PubMed PMID: 7267035]
Motiani MV, McCannel CA, Almanzor R, McCannel TA. Diagnosis of Choroidal Melanoma in Dense Asteroid Hyalosis. Seminars in ophthalmology. 2017:32(2):257-259. doi: 10.3109/08820538.2015.1053627. Epub 2016 Apr 8 [PubMed PMID: 27058861]
Rani PK, Prajapati RC. Role of OCT Angiography in the Detection of Retinal Vascular and Macular Abnormalities in Subjects with Asteroid Hyalosis. Seminars in ophthalmology. 2018 Nov 26:():1-5. doi: 10.1080/08820538.2018.1551497. Epub 2018 Nov 26 [PubMed PMID: 30475665]
Ogino K, Murakami T, Yoshimura N. Photocoagulation guided by wide-field fundus autofluorescence in eyes with asteroid hyalosis. Eye (London, England). 2014 May:28(5):634-5. doi: 10.1038/eye.2014.52. Epub 2014 Mar 7 [PubMed PMID: 24603417]
Level 3 (low-level) evidenceHwang JC, Barile GR, Schiff WM, Ober MD, Smith RT, Del Priore LV, Turano MR, Chang S. Optical coherence tomography in asteroid hyalosis. Retina (Philadelphia, Pa.). 2006 Jul-Aug:26(6):661-5 [PubMed PMID: 16829809]
Level 3 (low-level) evidenceAlasil T, Adhi M, Liu JJ, Fujimoto JG, Duker JS, Baumal CR. Spectral-domain and swept-source OCT imaging of asteroid hyalosis: a case report. Ophthalmic surgery, lasers & imaging retina. 2014 Sep-Oct:45(5):459-61 [PubMed PMID: 25230400]
Level 3 (low-level) evidenceKachewar SG, Kulkarni DS. An Imaging Review of Intra-ocular Calcifications. Journal of clinical and diagnostic research : JCDR. 2014 Jan:8(1):203-5. doi: 10.7860/JCDR/2014/4475.3904. Epub 2014 Jan 12 [PubMed PMID: 24596775]
Saurabh K, Roy R, Chowdhury M. Efficacy of Multicolor Imaging in Patients With Asteroid Hyalosis: Seeing the Unseen. JAMA ophthalmology. 2018 Apr 1:136(4):446-447. doi: 10.1001/jamaophthalmol.2018.0026. Epub [PubMed PMID: 29522059]
van den Born LI, van Soest S, van Schooneveld MJ, Riemslag FC, de Jong PT, Bleeker-Wagemakers EM. Autosomal recessive retinitis pigmentosa with preserved para-arteriolar retinal pigment epithelium. American journal of ophthalmology. 1994 Oct 15:118(4):430-9 [PubMed PMID: 7943119]
Level 2 (mid-level) evidenceDodwell DG, Freeman K, Shoch D. Juvenile asteroid hyalosis and pre-Descemet's dystrophy. American journal of ophthalmology. 1988 Oct 15:106(4):504-5 [PubMed PMID: 3263047]
Level 3 (low-level) evidenceIkeda Y, Hisatomi T, Murakami Y, Miyazaki M, Kohno R, Takahashi H, Hata Y, Ishibashi T. Retinitis pigmentosa associated with asteroid hyalosis. Retina (Philadelphia, Pa.). 2010 Sep:30(8):1278-81. doi: 10.1097/IAE.0b013e3181dcfc0a. Epub [PubMed PMID: 20827143]
Level 2 (mid-level) evidenceBurris CKH,Azari AA,Kanavi MR,Dubielzig RR,Lee V,Gottlieb JL,Potter HD,Kim K,Raven ML,Rodriguez ME,Reddy DN,Albert DM, Is There an Increased Prevalence of Asteroid Hyalosis in Eyes with Uveal Melanoma? A Histopathologic Study. Ocular oncology and pathology. 2017 Nov [PubMed PMID: 29344477]
Mouna A, Berrod JP, Conart JB. Visual Outcomes of Pars Plana Vitrectomy with Epiretinal Membrane Peeling in Patients with Asteroid Hyalosis: A Matched Cohort Study. Ophthalmic research. 2017:58(1):35-39. doi: 10.1159/000468990. Epub 2017 May 3 [PubMed PMID: 28463846]
Martin RG, Safir A. Asteroid hyalosis affecting the choice of intraocular lens implant. Journal of cataract and refractive surgery. 1987 Jan:13(1):62-5 [PubMed PMID: 3550044]
Level 3 (low-level) evidenceWackernagel W, Ettinger K, Weitgasser U, Bakir BG, Schmut O, Goessler W, Faschinger C. Opacification of a silicone intraocular lens caused by calcium deposits on the optic. Journal of cataract and refractive surgery. 2004 Feb:30(2):517-20 [PubMed PMID: 15030853]
Level 3 (low-level) evidenceLee YJ,Han SB, Laser treatment of silicone intraocular lens opacification associated with asteroid hyalosis. Taiwan journal of ophthalmology. 2019 Jan-Mar [PubMed PMID: 30993069]
Platt SM, Iezzi R, Mahr MA, Erie JC. Surgical removal of dystrophic calcification on a silicone intraocular lens in association with asteroid hyalosis. Journal of cataract and refractive surgery. 2017 Dec:43(12):1608-1610. doi: 10.1016/j.jcrs.2017.09.026. Epub [PubMed PMID: 29335107]
Espandar L, Mukherjee N, Werner L, Mamalis N, Kim T. Diagnosis and management of opacified silicone intraocular lenses in patients with asteroid hyalosis. Journal of cataract and refractive surgery. 2015 Jan:41(1):222-5. doi: 10.1016/j.jcrs.2014.11.009. Epub [PubMed PMID: 25532646]
Level 3 (low-level) evidenceSebag J, Yee KMP, Nguyen JH, Nguyen-Cuu J. Long-Term Safety and Efficacy of Limited Vitrectomy for Vision Degrading Vitreopathy Resulting from Vitreous Floaters. Ophthalmology. Retina. 2018 Sep:2(9):881-887. doi: 10.1016/j.oret.2018.03.011. Epub 2018 May 11 [PubMed PMID: 31047219]
Okuda Y, Kakurai K, Sato T, Morishita S, Fukumoto M, Kohmoto R, Takagi M, Kobayashi T, Kida T, Ikeda T. Two Cases of Rhegmatogenous Retinal Detachment Associated with Asteroid Hyalosis. Case reports in ophthalmology. 2018 Jan-Apr:9(1):43-48. doi: 10.1159/000485888. Epub 2018 Jan 17 [PubMed PMID: 29643781]
Level 3 (low-level) evidenceRenaldo DP. Pars plana vitrectomy for asteroid hyalosis. Retina (Philadelphia, Pa.). 1981:1(3):252-4 [PubMed PMID: 7348845]
Level 3 (low-level) evidenceLambrou FH Jr, Sternberg P Jr, Meredith TA, Mines J, Fine SL. Vitrectomy when asteroid hyalosis prevents laser photocoagulation. Ophthalmic surgery. 1989 Feb:20(2):100-2 [PubMed PMID: 2927889]
Level 3 (low-level) evidenceWilliams BK Jr, Elimimian EB, Shields CL. Asteroid Hyalosis Simulating Vitreous Seeds in a Patient With Retinoblastoma. Journal of pediatric ophthalmology and strabismus. 2019 Jul 5:56():e41-e44. doi: 10.3928/01913913-20190515-01. Epub 2019 Jul 5 [PubMed PMID: 31282959]