 Anatomy, Thorax, Triangle of Auscultation
Anatomy, Thorax, Triangle of Auscultation
Introduction
The so-called "triangle of auscultation" is a clinically important region of the posterior thorax (see Image. Triangle of Auscultation). The area is so named for its value in assessing esophageal obstruction before the advent of roentgenography. Sounds of transiting material near the stomach's cardiac orifice can be heard over this area, allowing examiners to determine the presence of esophageal obstruction.[1] The relative thinness of the structures in the triangle also permits the assessment of other thoracic structures in aid of physical examination and surgical procedures. This article discusses the anatomy of the triangle of auscultation and its importance in diagnosis and management.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The auscultation triangle lies at the inferior angle of the scapula. This region has inferior, medial, lateral, and anterior boundaries.[2]
- Inferior boundary - superior border of the latissimus dorsi muscle
- Medial boundary - lateral margin of the inferior aspect of the trapezius muscle
- Lateral boundary - lower aspect of the scapula's medial border.
- Anterior boundary (floor) - rhomboid major muscle, fascial sheet, 6th and 7th ribs, and intercostal space
The auscultation triangle can be made prominent by instructing the patient to cross their arms over the chest before bending forward. Upper extremity adduction displaces the scapula and the triangle's muscular boundaries, reducing the sound barriers between the examiner's stethoscope and the thoracic structures under evaluation. Wheezing, rhonchi, rales, and other adventitious respiratory sounds are easier to distinguish in this region.[3][4][5]
Embryology
Skeletal muscle formation occurs through the process of myogenesis.[6] The muscle cells originate from the paraxial mesoderm. This layer forms the somites, which later turn into the dermomyotomes and myotomes.
Skeletal muscle development is divided into the myoblast, myotubule, and myofiber stages. Myoblasts, the skeletal muscle cell progenitors, form large, multinucleated cells under the influence of fibroblast growth factors. Myoblasts initially divide and fuse continuously, but the secretion of extracellular matrix proteins heralds their maturation into myotubules. Myofibers form from myotubule fusion. Afterward, they stop dividing as fibroblast growth factors diminish. Myosatellite cells are multipotent cells persisting along the basal membrane that can give rise to new muscle tissue when activated.[7][8][9]
Blood Supply and Lymphatics
The triangle's blood supply is the same as that of its bounding structures.
- Thoracodorsal artery: supplies the latissimus dorsi muscle.[10]
- Superficial cervical artery: supplies the trapezius muscle.[11]
- Dorsal scapular artery: supplies the rhomboid major muscle.[12]
These arteries ensure adequate oxygenation and nutrient supply for the muscles in this region.
Nerves
The auscultation triangle also has the same innervation as that of its bounding structures.
- Thoracodorsal nerve - This nerve is also known as the middle subscapular nerve, and it innervates the latissimus dorsi.
- Accessory nerve (cranial nerve XI) and the C3 to C4 spinal nerves - These nerves supply the trapezius muscle.[13]
- Dorsal scapular nerve: This nerve supplies the rhomboid major.[14]
The triangle of auscultation does not have its own innervation, but the nerves above supply the surrounding structures for sensorimotor function.
Muscles
The auscultation triangle itself lacks significant muscle mass, although muscles form its borders. These muscles include the following:
- Lattisimus dorsi - This large muscle at the triangle's inferior border originates from the T7 to L5 spinous processes, thoracolumbar fascia, inferior angle of the scapula, lower ribs, and iliac crest. The latissimus dorsi inserts on the floor of the bicipital (intertubercular) groove of the humerus. The muscle adducts, medially rotates, and extends the arm at the glenohumeral joint.
- Trapezius - This muscle at the superior border of the triangle originates from the C7 to T12 spinous processes, occipital protuberance, ligamentum nuchae, and medial superior nuchal line. The trapezius inserts on the lateral clavicle, scapular spine, and acromion. The trapezius muscle is divided into the superior, middle, and inferior divisions. The superior fibers extend the neck and elevate and superiorly rotate the scapula. The middle fibers adduct the scapula. The inferior fibers stabilize and help rotate the scapula.[15]
- Rhomboid major - This muscle originates from the T2 to T5 spinous processes and inserts on the inner scapular border below the rhomboid minor. The rhomboid major retracts and rotates the scapula.[16]
These muscles move the arm, neck, and various regions of the thorax. Bending forward with crossed arms pulls the muscles away from the triangle, making auscultation easier.
Physiologic Variants
Anatomic variations differ based on which lung segment the auscultation triangle projects on from the surface. Cadaver studies reveal that the triangle can project on either the superior segment of the inferior lobe, posterior basal segment, or lateral basal segment. The projection was mirrored bilaterally in half of the cases.[3]
Surgical Considerations
The triangle of auscultation has advantages when used as an access route for various surgical procedures due to the absence of large muscular structures within the area. These procedures include:
- Scapular tumor excision - The triangle provides direct access to tumors originating from the ventral aspect of the scapula, particularly near the inferior angle. Osteochondromas have been excised through this window. The approach minimizes blood loss since the rhomboid major and trapezius are not dissected.
- Thoracotomy - A thoracotomy through the triangle of auscultation permits access to internal thoracic structures such as the lungs, pulmonary vasculature, heart, or aorta. This procedure may be performed emergently to evacuate a pericardial tamponade, control thoracic hemorrhage, administer internal cardiac massage, or cross-clamp the descending thoracic aorta. Access through the auscultation triangle reduces morbidity, as it dispenses the need for a latissimus dorsi incision.[17]
- Pleurectomy - A pleurectomy with access via the triangle reduces the need for a painful thoracotomy procedure. Recurrent spontaneous pneumothorax is a pleurectomy indication.[18]
- Rhomboid intercostal nerve block - A rhomboid intercostal nerve block can also be administered through this region to alleviate pain from rib fractures or a thoracotomy. Typically, this nerve block is accomplished by injecting a local anesthetic agent into the fascial plane between the upper intercostal portion of the rhomboids.[19]
Additionally, awareness of the triangle of auscultation is essential in patient positioning, as it can serve as a reference point for avoiding unnecessary back pressure or trauma during surgery.
Clinical Significance
The triangle of auscultation offers several advantages when performing thoracic auscultation and surgical procedures. The thinness of the structures in this region allows better acoustics and access to internal thoracic structures, as discussed in the previous sections. Knowledge of the anatomy of this region can help improve diagnostic accuracy and surgical safety.
Media
(Click Image to Enlarge)
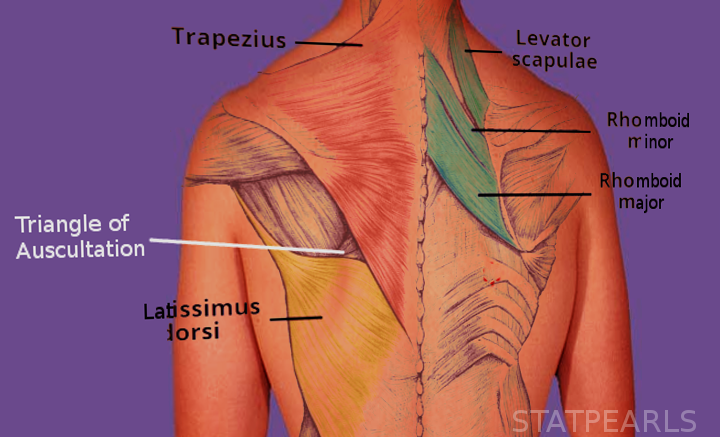
Triangle of Auscultation. The triangle of auscultation is bounded by the latissimus dorsi muscle (inferior), trapezius muscle (medial), scapula (lateral), and the rhomboid major, fascial sheet, 6th and 7th ribs, and intercostal space (anterior or floor).
Image courtesy S Bhimji MD
References
Prakash S, Kalra P, Khan Y, Dhal A. Ventral scapular osteochondroma excision through 'triangle of auscultation': A case series. Journal of orthopaedic surgery (Hong Kong). 2020 Jan-Apr:28(1):2309499019892848. doi: 10.1177/2309499019892848. Epub [PubMed PMID: 31916491]
Level 2 (mid-level) evidenceNazarian J, Down G, Lau OJ. Pleurectomy through the triangle of auscultation for treatment of recurrent pneumothorax in younger patients. Evaluation of 60 consecutive cases. Archives of surgery (Chicago, Ill. : 1960). 1988 Jan:123(1):113-4 [PubMed PMID: 3337648]
Level 3 (low-level) evidenceDiDio LJ, Yeasting RA. Projection of the triangle of auscultation on the human pulmonary surface. International surgery. 1977 Jun-Jul:62(6-7):338-40 [PubMed PMID: 893009]
Reyes FM, Modi P, Le JK. Lung Exam. StatPearls. 2023 Jan:(): [PubMed PMID: 29083650]
Rankin AJ, Rankin SH, Rankin AC. Auscultating heart and breath sounds through patients' gowns: who does this and does it matter? Postgraduate medical journal. 2015 Jul:91(1077):379-83. doi: 10.1136/postgradmedj-2015-133321. Epub 2015 Jul 16 [PubMed PMID: 26183342]
Chal J, Pourquié O. Making muscle: skeletal myogenesis in vivo and in vitro. Development (Cambridge, England). 2017 Jun 15:144(12):2104-2122. doi: 10.1242/dev.151035. Epub [PubMed PMID: 28634270]
Hernández-Hernández JM, García-González EG, Brun CE, Rudnicki MA. The myogenic regulatory factors, determinants of muscle development, cell identity and regeneration. Seminars in cell & developmental biology. 2017 Dec:72():10-18. doi: 10.1016/j.semcdb.2017.11.010. Epub 2017 Nov 15 [PubMed PMID: 29127045]
Musumeci G, Castrogiovanni P, Coleman R, Szychlinska MA, Salvatorelli L, Parenti R, Magro G, Imbesi R. Somitogenesis: From somite to skeletal muscle. Acta histochemica. 2015 May-Jun:117(4-5):313-28. doi: 10.1016/j.acthis.2015.02.011. Epub 2015 Apr 4 [PubMed PMID: 25850375]
Sato T, Koizumi M, Kim JH, Kim JH, Wang BJ, Murakami G, Cho BH. Fetal development of deep back muscles in the human thoracic region with a focus on transversospinalis muscles and the medial branch of the spinal nerve posterior ramus. Journal of anatomy. 2011 Dec:219(6):756-65. doi: 10.1111/j.1469-7580.2011.01430.x. Epub 2011 Sep 29 [PubMed PMID: 21954879]
Dennis M, Granger A, Ortiz A, Terrell M, Loukos M, Schober J. The anatomy of the musculocutaneous latissimus dorsi flap for neophalloplasty. Clinical anatomy (New York, N.Y.). 2018 Mar:31(2):152-159. doi: 10.1002/ca.23016. Epub 2017 Dec 28 [PubMed PMID: 29178203]
Yang D, Morris SF. Trapezius muscle: anatomic basis for flap design. Annals of plastic surgery. 1998 Jul:41(1):52-7 [PubMed PMID: 9678469]
HUELKE DF. The dorsal scapular artery--a proposed term for the artery to the rhomboid muscles. The Anatomical record. 1962 Jan:142():57-61 [PubMed PMID: 14449723]
Pu YM, Tang EY, Yang XD. Trapezius muscle innervation from the spinal accessory nerve and branches of the cervical plexus. International journal of oral and maxillofacial surgery. 2008 Jun:37(6):567-72. doi: 10.1016/j.ijom.2008.02.002. Epub 2008 Mar 17 [PubMed PMID: 18346876]
Lee DG, Chang MC. Dorsal scapular nerve injury after trigger point injection into the rhomboid major muscle: A case report. Journal of back and musculoskeletal rehabilitation. 2018 Feb 6:31(1):211-214. doi: 10.3233/BMR-169740. Epub [PubMed PMID: 28854498]
Level 3 (low-level) evidenceCamargo PR, Neumann DA. Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 2: trapezius. Brazilian journal of physical therapy. 2019 Nov-Dec:23(6):467-475. doi: 10.1016/j.bjpt.2019.01.011. Epub 2019 Feb 3 [PubMed PMID: 30797676]
Jung H, Bae J, Kim J, Yoo Y, Lee HJ, Rho H, Han AH, Moon JY. Can the Rhomboid Major Muscle Be Used to Identify the Thoracic Spinal Segment on Ultrasonography? A Prospective Observational Study. Pain medicine (Malden, Mass.). 2022 Sep 30:23(10):1670-1678. doi: 10.1093/pm/pnac043. Epub [PubMed PMID: 35289904]
Level 2 (mid-level) evidenceKhan IH, McManus KG, McCraith A, McGuigan JA. Muscle sparing thoracotomy: a biomechanical analysis confirms preservation of muscle strength but no improvement in wound discomfort. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2000 Dec:18(6):656-61 [PubMed PMID: 11113671]
Lau OJ, Shawkat S. Pleurectomy through the triangle of auscultation. Thorax. 1982 Dec:37(12):945-6 [PubMed PMID: 7170685]
Ökmen K. Efficacy of rhomboid intercostal block for analgesia after thoracotomy. The Korean journal of pain. 2019 Apr 1:32(2):129-132. doi: 10.3344/kjp.2019.32.2.129. Epub [PubMed PMID: 31091512]