Introduction
The sublingual gland is the smallest of the three major salivary glands [1], which also include the parotid and submandibular glands. The sublingual gland lies between the muscles of the floor of the oral cavity, which include the geniohyoid muscle, hyoglossus muscle medially, and the mylohyoid muscle inferiorly. The mandible borders the sublingual glands laterally [2].
The ducts of Rivinus, a group of excretory ducts, drain the sublingual gland. The largest sublingual gland excretory duct called the sublingual duct of Bartholin joins Wharton’s duct near the sublingual caruncle. The sublingual caruncle is a papilla located medial to the sublingual gland and lateral to the lingual frenulum [2]. The sublingual gland contributes approximately 5% of saliva in the oral cavity [3].
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The sublingual glands lie inferolateral to the tongue, below the mucosa of the floor of the mouth, and above the mylohyoid muscle. Sublingual tissue is palpable behind the mandibular canines. The sublingual gland acquires an oval shape when sectioned transversely, however, the gland shape is longitudinal and lentiform when sectioned parallel to the body of the mandible [2]. The gland is composed of a major sublingual gland and around eight to thirty minor sublingual glands [1].
The sublingual gland differs from the other major salivary glands, because it lacks intercalated or striated ducts, so the saliva secretes directly through the ducts of Rivinus. These ducts empty along an elevated ridge called the plica fimbriate formed by the sublingual folds, which are oblique to the frenulum linguae bilaterally. The sublingual duct of Bartholin joins Wharton’s duct to form the draining orifice on each side of the lingual frenulum [4].
The sublingual tissue is predominantly a mucous gland, however, is considered a mixed serous and mucous gland. It is made up of mainly mucous acini with serous demilunes. It is the only unencapsulated major salivary gland. Sublingual tissue primarily produces a thick mucinous fluid and lubricates the oral cavity which allows for swallowing, initiating digestion, buffering pH, and dental hygiene [3].
The composition of saliva depends on the salivary flow rate and can vary given each gland's flow rate and overall contribution. Saliva is comprised of both organic and inorganic components. Inorganic components include electrolytes, urea, and ammonia. The organic elements of saliva contain immunoglobulins, enzymes, and proteins [3].
The primary protein found in mucous saliva is mucin, which functions to lubricate and competitively inhibit bacterial attachment to the salivary duct epithelium. This action allows for antimicrobial protection of the sublingual gland [3].
Magnetic Resonance Imaging of the Normal Appearance of the Sublingual Gland
The sublingual gland is located on the sublingual depression, resting on the mylohyoid muscle. It is separated from the genioglossus muscle medially by Wharton's duct. The sublingual gland appears on TI-weighted MRI as a structure of an intermediate signal intensity that is lower than that of the fat tissues surrounding the gland although higher than the signal intensity of the muscles [5].
Embryology
The sublingual gland develops later than the other major salivary glands as it first appears in the eighth week of prenatal development. It originates from epithelial buds surrounding the sublingual folds on the floor of the mouth. These epithelial buds develop into cords, which canalize to form the sublingual ducts and also form the mucous acini. Initially, the sublingual gland develops laterally to the submandibular gland before transitioning to a position anterior and superior to the submandibular gland when development is complete [4].
Blood Supply and Lymphatics
The sublingual glands receive their primary blood supply from the sublingual and submental arteries, which are branches of the lingual artery and facial artery, respectively. These arteries are both branches of the external carotid artery. The sublingual vein drains into the lingual vein, which then flows into the internal jugular system.
The sublingual glands drain into the submandibular lymph nodes. The submandibular lymphatics comprise 3 to 6 nodes, which are located in the submaxillary triangle, beneath the body of the mandible. The nodes are palpable on the superficial surface of the submandibular gland. Malignant tumors may drain into these regional lymph nodes, requiring more extensive neck dissection for the complete treatment of cancer.
Nerves
The sublingual glands receive their parasympathetic input via the chorda tympani nerve, which is a branch of the facial nerve via the submandibular ganglion. The nerve functions in a secretomotor capacity. The chorda tympani branches from the motor branch of the facial nerve in the middle ear cavity, which then exits the middle ear through the petrotympanic fissure. The chorda tympani nerve then travels with the lingual nerve to synapse at the submandibular ganglion. The postganglionic fibers reach the sublingual gland, and release acetylcholine and substance P. Acetylcholine, the primary neurotransmitter, and the muscarinic receptors work to increase salivation [4].
Muscles
The sublingual gland is positioned above the mylohyoid muscle and below the mucosa of the floor of the mouth.
Physiologic Variants
Sublingual gland hypertrophy may be the result of a congenital absence of the submandibular gland. [6]
Surgical Considerations
An operation to excise the sublingual gland most commonly involves transoral electrocautery and blunt dissection. Structures most at risk of injury during gland excision are the lingual nerve and Wharton's duct. The sublingual tissue can be found in the anterior floor of the mouth and directly deep to Wharton’s duct.
A sublingual gland flap can be used to manage major pathologies affecting the mandible and maxilla bones; it seems that this surgery is capable of giving excellent results. [7]
Clinical Significance
Ranula
A ranula is a pseudocyst caused by either the extravasation of saliva or the retention of mucous of the sublingual gland [8]. It is worth noting that a pseudocyst differentiates from a cyst because the former lacks epithelial lining to the cyst wall [8]. A ranula can be described as simple or deep. Simple ranulas are mucous retention cysts located deep to the floor of the mouth but remain above the mylohyoid muscle. A deep or cervical ranula occurs when the sublingual duct is leaking, and the collecting mucous dissects through the mylohyoid muscle into the submental or lateral neck adjacent tissue planes, forming a pseudocyst. Both are usually caused by local trauma that damages the sublingual gland allowing mucous to collect. The ranula presents as a fluctuant, swollen mass at the floor of the mouth with a bluish tint. If larger, this may lead to dysphagia, however, it is usually painless unless infected. The ranula is primarily located lateral to the midline of the floor of the mouth, and this helps to distinguish its presentation from a dermoid cyst which usually presents in the midline [9].
Diagnosis involves a thorough clinical history and physical exam. Ultrasound helps to differentiate between a simple or deep ranula as it can confirm the depth above or below the mylohyoid muscle and the overall quality of the lesion. Ultrasound can also identify rupture or herniation of the sublingual gland. Treatment options include removal of the sublingual gland with ranula excision, marsupialization, or sclerotherapy. Excising the sublingual gland helps to minimize recurrence. This lesion usually presents in children and is the most common pathologic lesion of the sublingual gland [9].
Neoplasia
Neoplastic diseases may affect the sublingual gland as 3% to 4% of head and neck cancers involve salivary glands. The larger the size of the gland, the higher the odds of a mass being benign [3].
Sublingual gland tumors are usually malignant and comprise about 1.6% of all salivary gland malignancies. Adenoid cystic carcinoma and mucoepidermoid carcinoma count as the most common sublingual gland malignancies reported. Most tumors present with an asymptomatic floor of mouth swelling and present similarly to benign conditions making diagnosis difficult. Treatment course most commonly includes surgical tumor excision. Neck dissection and radiation therapy may be indicated in advanced tumor staging or aggressive pathologies [10].
Sialolithiasis
Salivary stones (calculi) obstructing an excretory duct is a common salivary gland disease. The pathophysiology of salivary calculi is related to salivary stasis and overall inflammation of the excretory duct. Salivary stones may cause swelling of the duct or gland causing colicky peri-prandial pain. Salivary calculi are manually palpable when lodged in a duct. Ultrasound can aid diagnosis along with adjunctive CT or MR sialography if workup is negative, but suspicion remains high. Initial treatment is conservative, which comprises oral hydration and sialagogues. Surgery is only recommended when a conservative approach fails, and symptoms persist. Sialolithiasis mainly impacts the submandibular gland and rarely occurs in the sublingual gland [3].
Sialadenitis
Acute sialadenitis refers to salivary gland inflammation and may be caused by bacterial or viral infection. The inflammation may be accompanied by fever, pain, and gland swelling. If the etiology is a bacterial infection, then antibiotics are recommended. Otherwise, oral hydration and sialagogues are indicated. If the formation of an abscess complicates the infection, surgical intervention may be required. Chronic inflammation of the salivary glands can be related to recurrent infections, autoimmune conditions (e.g. Sjogren's syndrome), or radiation exposure. The sublingual gland is rarely affected by any of these acute or chronic problems in isolation [3].
Regeneration of the Salivary Glands
After surgical resection of tumors of the salivary glands and radiation therapy of head and neck cancers, patients may have a residual long-term loss of function of the salivary glands. This is where regenerative medicine comes into play, with the possibility of restoring the lost glandular function. It could also potentially help patients suffering from gland disfunction, like in Sjögren syndrome [11].
Other Issues
The use of interferential current stimulation has been investigated for patients who suffer from dry mouth. It may be an approach to stimulate the function of the sublingual and submandibular glands. This therapy modality does not create distress or pain for the patient [12].
Media
(Click Image to Enlarge)
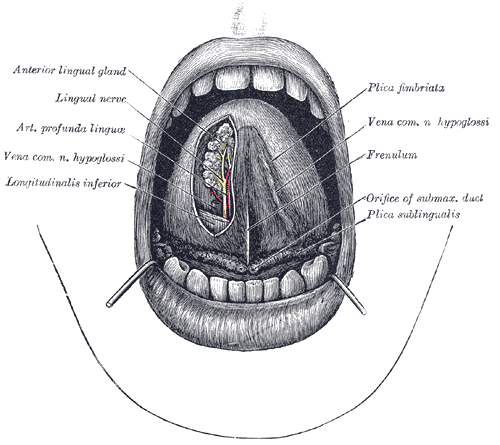
The Mouth, The mouth cavity, The apex of the tongue is turned upward, Anterior lingual gland, Lingual nerve, Arterial Profunda linguae, Vena Common Hypoglossi nerve, Longitudinalis inferior, Plica fimbriata, Frenulum, Plica sublingualis
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Kessler AT, Bhatt AA. Review of the Major and Minor Salivary Glands, Part 1: Anatomy, Infectious, and Inflammatory Processes. Journal of clinical imaging science. 2018:8():47. doi: 10.4103/jcis.JCIS_45_18. Epub 2018 Nov 15 [PubMed PMID: 30546931]
Bialek EJ, Jakubowski W, Zajkowski P, Szopinski KT, Osmolski A. US of the major salivary glands: anatomy and spatial relationships, pathologic conditions, and pitfalls. Radiographics : a review publication of the Radiological Society of North America, Inc. 2006 May-Jun:26(3):745-63 [PubMed PMID: 16702452]
Armstrong MA, Turturro MA. Salivary gland emergencies. Emergency medicine clinics of North America. 2013 May:31(2):481-99. doi: 10.1016/j.emc.2013.01.004. Epub [PubMed PMID: 23601484]
Holmberg KV, Hoffman MP. Anatomy, biogenesis and regeneration of salivary glands. Monographs in oral science. 2014:24():1-13. doi: 10.1159/000358776. Epub 2014 May 23 [PubMed PMID: 24862590]
Sumi M, Izumi M, Yonetsu K, Nakamura T. Sublingual gland: MR features of normal and diseased states. AJR. American journal of roentgenology. 1999 Mar:172(3):717-22 [PubMed PMID: 10063867]
Level 2 (mid-level) evidenceChung J, Lee YW. Functional compensation of a hypertrophied sublingual gland and the absence of the ipsilateral submandibular gland. The British journal of oral & maxillofacial surgery. 2019 Oct:57(8):813-816. doi: 10.1016/j.bjoms.2019.06.019. Epub 2019 Jul 2 [PubMed PMID: 31277911]
Jose A, Rawat A, Singh S, Nagori SA, Roychoudhury A. Management of Intraoral Surgical Defects Using Sublingual Gland Flap. The Journal of craniofacial surgery. 2020 Nov/Dec:31(8):e766-e767. doi: 10.1097/SCS.0000000000006714. Epub [PubMed PMID: 33136905]
Nguyen BN, Malone BN, Sidman JD, Barnett Roby B. Excision of sublingual gland as treatment for ranulas in pediatric patients. International journal of pediatric otorhinolaryngology. 2017 Jun:97():154-156. doi: 10.1016/j.ijporl.2017.04.003. Epub 2017 Apr 5 [PubMed PMID: 28483227]
Ugga L, Ravanelli M, Pallottino AA, Farina D, Maroldi R. Diagnostic work-up in obstructive and inflammatory salivary gland disorders. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 2017 Apr:37(2):83-93. doi: 10.14639/0392-100X-1597. Epub [PubMed PMID: 28516970]
Andreasen S, Bjørndal K, Agander TK, Wessel I, Homøe P. Tumors of the sublingual gland: a national clinicopathologic study of 29 cases. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2016 Nov:273(11):3847-3856 [PubMed PMID: 27015666]
Level 3 (low-level) evidenceKok MR, Yamano S, Lodde BM, Wang J, Couwenhoven RI, Yakar S, Voutetakis A, Leroith D, Schmidt M, Afione S, Pillemer SR, Tsutsui MT, Tak PP, Chiorini JA, Baum BJ. Local adeno-associated virus-mediated interleukin 10 gene transfer has disease-modifying effects in a murine model of Sjögren's syndrome. Human gene therapy. 2003 Nov 20:14(17):1605-18 [PubMed PMID: 14633403]
Level 3 (low-level) evidenceHasegawa Y, Sugahara K, Sano S, Sakuramoto A, Kishimoto H, Oku Y. Enhanced salivary secretion by interferential current stimulation in patients with dry mouth: a pilot study. Oral surgery, oral medicine, oral pathology and oral radiology. 2016 May:121(5):481-9. doi: 10.1016/j.oooo.2016.01.017. Epub 2016 Feb 13 [PubMed PMID: 27017403]
Level 3 (low-level) evidence