Introduction
The falx cerebri is a sickle-shaped structure formed from the invagination of the dura mater into the longitudinal fissure between the cerebral hemispheres. The falx cerebri is anchored posteriorly to the internal occipital protuberance, travels superiorly to the corpus callosum, and anchors anteriorly to the crista galli forming a sail-like structure between the cerebral hemispheres. The falx cerebri contains blood vessels, nerves, and is a common site of falcine meningiomas and age-related calcification.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The brain is enveloped by three membranes, the pia mater, arachnoid mater, and dura mater. These three membranes are collectively called the meninges. The dura mater is the strong, fibrous outermost membrane which provides a double layer of protection within the cranial cavity. The two layers of dura mater within the neurocranium are the periosteal layer which adheres directly to the inner neurocranium and meningeal layer which surrounds the brain tissue along with the arachnoid and pia mater. The meningeal dura mater invaginates between brain regions to form dural partitions - the falx cerebri, falx cerebelli, tentorium cerebelli, and sellar diaphragm.
The falx cerebri separates the cerebral hemispheres and provides channels, known as dural sinuses, for blood and cerebral spinal fluid to drain. The falx cerebri is a sail-like structure which is anchored posteriorly at the internal occipital protuberance, superiorly to the periosteal dura mater, and anteriorly to the crista galli which sits above the ethmoid bone.[2] The superior and inferior sagittal sinuses form from spaces between the meningeal dura mater folds which make up the falx cerebri. The superior sagittal sinus follows the superior margin of the falx cerebri and the inferior sagittal sinus follows the free margin of the falx cerebri above the corpus callosum. These sinuses receive cerebral spinal fluid from the arachnoid granulation and blood from meningeal and bridging veins which drain from the dura and neural tissue. The blood from the superior sagittal sinus and inferior sagittal sinus eventually drain into the internal jugular veins and finally into the systemic circulation.[3]
Embryology
The three meningeal layers derive from the meninx primitiva, which is meningeal mesenchyme. The arachnoid and pia form from the leptomenix and the dura mater from the pachymeninx. While the pia mater and arachnoid mater originate from neural crest cells, the dura mater develops from the mesoderm. The dura mater forms a single layer of protection around the developing spinal cord but forms a double layer around the skull, eventually forming the periosteal and meningeal dural membranes. The process is similar to how the parietal and visceral layers of the peritoneum form in the abdominal cavity. The dura mater is a continuous membrane that forms a double layer membrane by folding in on itself where two layers of cells form in the peripheral mesenchyme - the thicker forms the periosteal dura and the thinner, the meningeal dura. As the brain develops, the meningeal dural layer invaginates between the brain regions forming dural partitions. Interruptions in brain development such as semi-lobar holoprosencephaly can prevent the dural partitions from forming appropriately.[4][5]
Blood Supply and Lymphatics
The falx cerebri receives its blood supply primarily from two vessels. The anterior portion of the falx receives its blood supply from the anterior meningeal artery, also known as the anterior falx artery or anterior falcine artery, which arises from the anterior ethmoidal artery.[6] The posterior falx receives its blood supply from the posterior meningeal artery, which is a branch of the ascending pharyngeal artery. The lymphatic drainage of the falx cerebri occurs via the meningeal lymphatic vessels which run parallel to the dural sinuses. These lymphatic vessels drain primarily along a similar path as the dural sinuses eventually exiting the jugular foramen and emptying into the deep cervical lymph nodes. A minority of lymph from the falx cerebri drains anteriorly through the cribriform plate into the lymphatics of the nasal mucosa. Lymphatic of the meninges differs from the lymphatics of the systemic system in a couple of ways. First, the lymphatics mostly lack valves which, in the body, prevent the retroactive flow of lymph because lymphatics are a low-pressure system. Second, the lymphatics are thinner and follow closely with the venous drainage of the meninges with few branch points.[7][8][9]
Nerves
The falx cerebri receives its innervation from all three branches of the trigeminal nerve and receives sympathetic fibers predominantly from the superior cervical ganglia. Additionally, the falx may receive additional innervation from the dorsal rami of cervical nerves 1,2, and 3, the hypoglossal nerve, and recurrent branches of the vagus nerve.[10][11]
Muscles
There are no muscle attachments to, or within the falx cerebri. The only muscle cells associated with the meninges are the smooth muscle cells of the vasculature which run within the meninges.
Physiologic Variants
Agenesis of the falx cerebri has been documented and usually correlates with other developmental complications. Falx cerebri agenesis in individuals without other neural symptoms is exceptionally rare. Additionally, a persistent falcine sinus occurs in patients where the straight sinus fails to form during development or is thrombosed.[12]
Surgical Considerations
The falx cerebri is a significant surgical landmark for neurosurgeons accessing the lateral ventricles via an interhemispheric transcallosal approach. Agenesis or partial agenesis of the falx cerebri allows the cerebral hemispheres to adhere and prevent midline transcallosal surgical access to the ventricles.[13]
Clinical Significance
In addition to the pathologies that affect all of the dural structures (e.g., bacterial meningitis), the falx cerebri is clinically significant in two common scenarios. First, the falx cerebri is the site of falcine meningiomas which account for approximately ~8.5% of intracranial meningiomas. These meningiomas are benign and form well-circumscribed, usually round masses attached to the dura. Meningiomas primarily arise from arachnoidal cap cells and can cause seizures. Headaches, nausea, and vomiting are common manifestations due to increased intracranial pressure following its significant growth. Biopsy findings will show tumor cells depending on the grade of the tumor and also showing syncytial nests, which may calcify into psammoma bodies.[14][15] Symptomatic meningiomas are often removed surgically with occasional preoperative embolization to reduce its size and intraoperative bleeding. Practitioners can follow the principle of adequate exposure, devascularisation, intracapsular decompression, and then followed by complete excision. Damage to the sagittal sinus, thereby leading to bleeding and air embolism and malignant brain edema due to venous infarction is the main intraoperative concern. Therefore, study regarding the patency of the sinus, its probable invasion by the tumor and the status of the collateral vessels is of paramount importance while formulating the management plan of these tumors especially for tumors attached to the middle and posterior third of the superior sagittal sinus.
The second common clinical scenario occurs in traumatic brain injury leading to a substantial anterior cranial fossa extradural hematoma or the frontal contusions. They can cause significant mass effect forcing the ipsilateral cingulate gyrus to herniate under the falx cerebri leading to subfalcine herniation.[16]
Media
(Click Image to Enlarge)
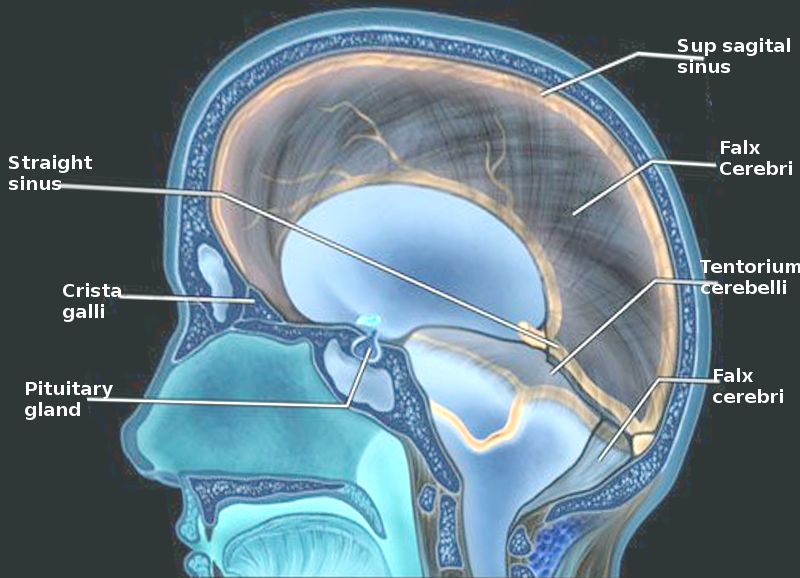
Falx cerebri Image courtesy O. Chaigasame
References
WELIKALA AH. Extensive calcification of the falx cerebri. The British journal of radiology. 1947 Jul:20(235):295 [PubMed PMID: 20249177]
Kostecki K, De Jesus O, Pearson-Shaver AL. Subfalcine Herniation. StatPearls. 2023 Jan:(): [PubMed PMID: 30725631]
Bayot ML, Reddy V, Zabel MK. Neuroanatomy, Dural Venous Sinuses. StatPearls. 2023 Jan:(): [PubMed PMID: 29489265]
O'Rahilly R, Müller F. The meninges in human development. Journal of neuropathology and experimental neurology. 1986 Sep:45(5):588-608 [PubMed PMID: 3746345]
Cayea PD, Balcar I, Alberti O Jr, Jones TB. Prenatal diagnosis of semilobar holoprosencephaly. AJR. American journal of roentgenology. 1984 Feb:142(2):401-2 [PubMed PMID: 6607617]
Level 3 (low-level) evidencePollock JA, Newton TH. The anterior falx artery: normal and pathologic anatomy. Radiology. 1968 Dec:91(6):1089-95 [PubMed PMID: 5699608]
Da Mesquita S, Fu Z, Kipnis J. The Meningeal Lymphatic System: A New Player in Neurophysiology. Neuron. 2018 Oct 24:100(2):375-388. doi: 10.1016/j.neuron.2018.09.022. Epub [PubMed PMID: 30359603]
Absinta M, Ha SK, Nair G, Sati P, Luciano NJ, Palisoc M, Louveau A, Zaghloul KA, Pittaluga S, Kipnis J, Reich DS. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. eLife. 2017 Oct 3:6():. doi: 10.7554/eLife.29738. Epub 2017 Oct 3 [PubMed PMID: 28971799]
Louveau A, Smirnov I, Keyes TJ, Eccles JD, Rouhani SJ, Peske JD, Derecki NC, Castle D, Mandell JW, Lee KS, Harris TH, Kipnis J. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015 Jul 16:523(7560):337-41. doi: 10.1038/nature14432. Epub 2015 Jun 1 [PubMed PMID: 26030524]
Lee SH, Shin KJ, Koh KS, Song WC. Visualization of the tentorial innervation of human dura mater. Journal of anatomy. 2017 Nov:231(5):683-689. doi: 10.1111/joa.12659. Epub 2017 Jul 10 [PubMed PMID: 28695607]
Lv X, Wu Z, Li Y. Innervation of the cerebral dura mater. The neuroradiology journal. 2014 Jun:27(3):293-8. doi: 10.15274/NRJ-2014-10052. Epub 2014 Jun 17 [PubMed PMID: 24976196]
Level 3 (low-level) evidenceRyu CW. Persistent falcine sinus: is it really rare? AJNR. American journal of neuroradiology. 2010 Feb:31(2):367-9. doi: 10.3174/ajnr.A1794. Epub 2009 Sep 24 [PubMed PMID: 19779000]
Level 2 (mid-level) evidenceChaddad-Neto F, Devanir Silva da Costa M, Bozkurt B, Leonardo Doria-Netto H, de Araujo Paz D, da Silva Centeno R, Grande AW, Cavalheiro S, Yağmurlu K, Spetzler RF, Preul MC. Contralateral anterior interhemispheric-transcallosal-transrostral approach to the subcallosal region: a novel surgical technique. Journal of neurosurgery. 2018 Aug:129(2):508-514. doi: 10.3171/2017.4.JNS16951. Epub 2017 Nov 3 [PubMed PMID: 29099298]
Shaikh N, Dixit K, Raizer J. Recent advances in managing/understanding meningioma. F1000Research. 2018:7():. pii: F1000 Faculty Rev-490. doi: 10.12688/f1000research.13674.1. Epub 2018 Apr 24 [PubMed PMID: 29770198]
Level 3 (low-level) evidenceMurrone D, De Paulis D, di Norcia V, Di Vitantonio H, Galzio RJ. Surgical management of falcine meningiomas: Experience of 95 patients. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2017 Mar:37():25-30. doi: 10.1016/j.jocn.2016.11.002. Epub 2016 Nov 22 [PubMed PMID: 27884604]
Munakomi S, Das JM. Brain Herniation. StatPearls. 2024 Jan:(): [PubMed PMID: 31194403]