Introduction
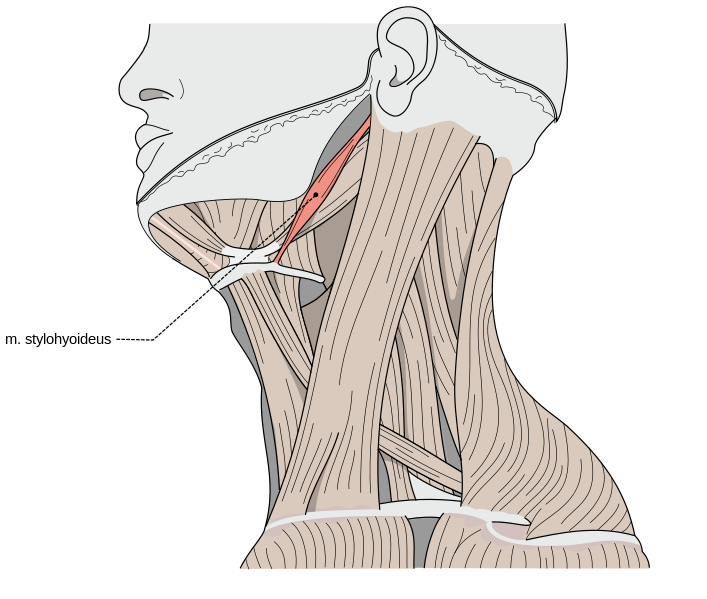
The stylohyoid muscle (musculus stylohyoideus in Latin) is one of the suprahyoid muscles of the neck that stretches between the base of the skull and the hyoid bone (see Image. Stylohyoid Muscle). The stylohyoid is paired and narrow muscle in close proximity to the digastric muscle, extending along the superior border of its posterior belly.
Despite its narrow shape, the stylohyoid muscle plays a role in various functions. It participates in chewing, swallowing, and phonetics when working with the other suprahyoid muscles (stylohyoid, digastric, mylohyoid, and geniohyoid). It contributes to the fixation of the hyoid bone when working the other suprahyoid and infrahyoid muscles.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The stylohyoid muscle consists of a single belly that runs anteroinferior from the styloid process to the hyoid bone.[1] It has the longest mean fiber bundle length of all the suprahyoid muscles.[1] In its origin, the stylohyoid muscle inserts through a small tendon into the posterior aspect of the styloid process, near its base.[2] Then, it extends downward and forwards to attach to the hyoid bone at the junction of the body and greater cornu, immediately superior to the omohyoid muscle's insertion.[2] The stylohyoid muscle is penetrated by the intermediate tendon of the digastric muscle near its insertion.[1][2] See Image. Illustrated Image of the Stylohyoid Muscle.
Ozgur et al. studied 56 specimens of stylohyoid muscles. They found that the point of insertion on the hyoid bone corresponded to the junction of the body and greater horn in 60.7% of cases, and in 39.3% of cases, the insertion point differed.[2] In these specimens, the muscle fibers were atypical and shaped like an arch in front of the hyoid bone. The fibers moved inward and inserted into the hyoid bone.[2]
The stylohyoid muscle connects to the posterior belly of the digastric muscle in its path. It lies anteromedial to the superior margin of the posterior belly of the digastric muscle. The styloglossus muscle lies medially and anterior to the stylohyoid muscle. The stylopharyngeal muscle is located between the stylohyoid and the styloglossus muscle. The stylohyoid and the styloglossus muscles form a space that gives passage to the external carotid artery superiorly and the facial artery inferiorly as it courses from the retrostyloid area to the prestyloid area.[3]
The Styloid Process
The styloid process is a long needle-like structure that extends from the inferior surface of the petrous temporal bone.[4] The stylopharyngeus, stylohyoid, and styloglossus muscles and stylohyoid and stylomandibular ligaments insert into the styloid process.[4]
The styloid process' average length is 2 to 3 cm, and it tapers from its base to the apex.[5][4] Although uncommon, this slender bone projection has sometimes been found to be curved.[6]
The styloid process locates in between the external and internal carotid arteries.[2] Furthermore, other important anatomical structures are near the styloid process. Medially, it relates to the internal jugular vein, the superficial temporal, lingual, facial, maxillary, and internal carotid arteries, and the sphenomandibular ligament.[2][7][8][9] Laterally, it relates to the occipital artery, facial and hypoglossal nerves, and the posterior belly of the digastric muscle.[2][7][8][9]
Function
The stylohyoid muscle connects the hyoid bone to the base of the skull, and it pulls the hyoid bone upward and backward, resulting in elevation of the base of the tongue and elongation of the floor of the mouth. This movement helps in deglutition and this muscle functions in association with other suprahyoid muscles. When the infrahyoid muscles stabilize the hyoid bone, the suprahyoid muscles depress the mandible and open the mouth widely. They also play an active role in improving the flexion movement of the neck and producing treble sounds.
Embryology
The stylohyoid muscle develops from the mesoderm of the second pharyngeal arch.[10] It appears along with other suprahyoid muscles in the eighth week of gestation.[3]
Blood Supply and Lymphatics
The stylohyoid muscle receives its vascular supply from branches of the external carotid artery, and the occipital branch of the external carotid artery gives branches to the stylohyoid. Lymphatic drainage from this part of the neck goes into the submental and submandibular group of lymph nodes, and then it drains into the deep cervical group of lymph nodes.
Nerves
The nerve supply derives from the facial nerve.[11][10] After exiting the stylomastoid foramen, the digastric branch of the facial nerve supplies the posterior bellies of the digastric muscle and stylohyoid muscles.[10] The nerve for the stylohyoid muscle can arise directly from the facial nerve.[10]
Physiologic Variants
The stylohyoid muscle may be absent or double in some individuals.[2] Physiological variation in its insertion area may also exist. It may insert into the mylohyoid muscle or omohyoid muscles. It has sometimes been found medial to the external carotid.[2]
Surgical Considerations
In the marginal mandibular nerve lesion, which results in asymmetrical lips, surgical intervention is required to improve the aesthetic and functions. Stylohyoid muscle transfer is a possible surgical option when the digastric muscle is not an option.
Clinical Significance
The stylohyoid muscle is a part of a significant anatomical structure known as the stylopharyngeal septum/styloid diaphragm. This septum is considered an essential surgical landmark when attempting to enter the pharyngeal spaces. The septum divides the space into two compartments - prestyloid and retrostyloid - based on its relationship with the septum.
Partial ossification of the ligament of the stylohyoid muscle may lead to Eagle syndrome, also known as the stylohyoid syndrome.[12] This condition results in sharp shooting pain unilaterally in the jaw. The pain may radiate into the throat, tongue, or ear, which causes difficulty in deglutition, sore throat, and tinnitus.[12] Surgical resection of the ligament is required as it compresses the underlying structures.[13]
The facial nerve has a significant contribution to the oropharyngeal phase of deglutition through various muscles. It innervates the stylohyoid muscle in association with other muscles, such as the buccinator muscle, perioral muscles, and the posterior belly of the digastric muscle. Patients with peripheral facial palsy may experience swallowing difficulty.[14] Paralysis or weakness of the stylohyoid may occur if the facial nerve gets damaged. An intracranial facial nerve lesion (before its exit from the stylomastoid foramen) may occur due to a middle ear pathology (tumor or infection). An extracranial lesion of the facial nerve can occur due to an infection of the nerve such as herpes virus, compression during forceps delivery (since incomplete development of the neonatal mastoid process leaves the nerve unprotected), or it can be idiopathic.
Pathologic conditions associated with the stylohyoid muscle may result in cervical and pharyngeal symptoms such as neck pain laterally in the area of the angle of the mandible, submandibular space, and anterior upper neck (see Image. Anterior Neck Muscles and Related Structures). The pain may get exacerbated by normal actions such as speaking, swallowing, yawning, or head-turning. Myofascial pain syndrome can result in severe pain in the stylohyoid muscle; treatment includes nonsteroidal anti-inflammatory drugs to reduce pain and inflammation. Severe cases may require injections to numb the affected area.
If the stylohyoid muscle inserts in an unusual fashion where it covers the hyoid bone as a belt, patients may report stylohyoid syndrome symptoms, including orofacial and cervical pain usually triggered by neck movements.[2][15]
Other Issues
The stylohyoid muscle is nearly horizontal in children. However, its shape and length change with age; thus, the course of the stylohyoid muscle becomes more vertical in adults.
The stylohyoid muscle can be palpated by placing the fingers along the direction of the muscle fiber under the chin and superiorly to the hyoid bone. Palpation is done laterally from the hyoid bone towards the ear lobe along the anterior border of the sternocleidomastoid muscle. At the same time, the patient is asked to swallow or place the tongue against the mouth roof, pushing against it.
Media
(Click Image to Enlarge)
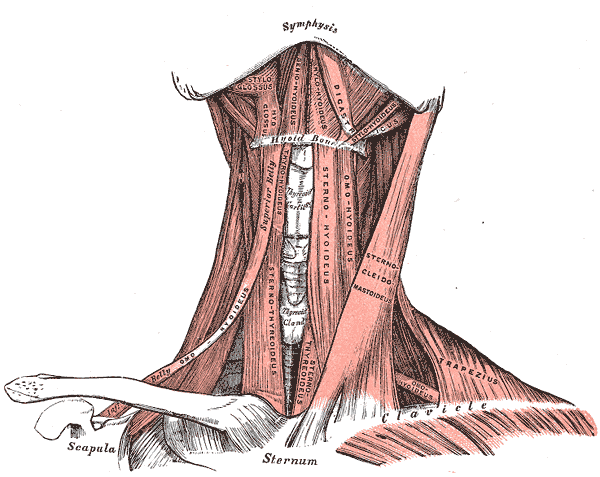
Anterior Neck Muscles and Related Structures. This illustration shows the supra- and infrahyoid, styloglossus, hyoglossus, geniohyoideus, mylohyoideus, digastricus, stylohyoideus, omohyoideus, sternothyroideus, sternohyoideus, omohyoideus, sternocleidomastoideus, trapezius, and omohyoideus muscles. The mandibular symphysis, thyroid cartilage, thyroid gland, hyoid bone, clavicles, scapula, and sternum are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
(Click Image to Enlarge)
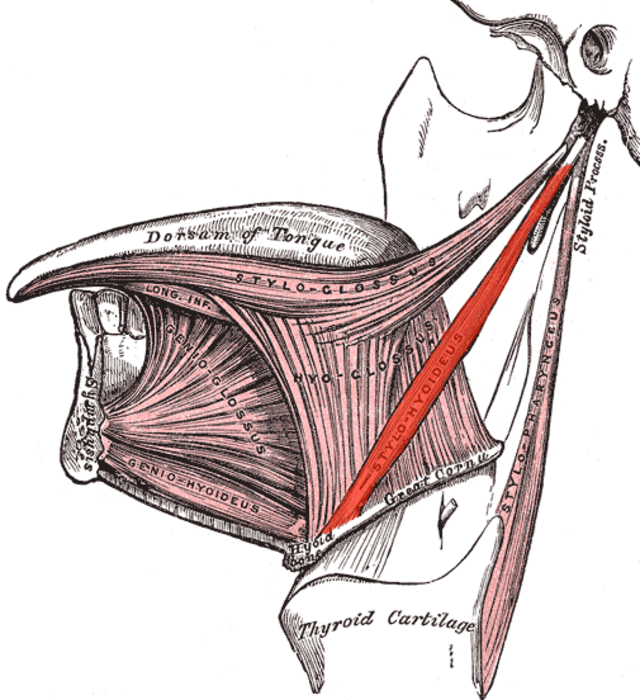
Illustrated Image of the Stylohyoid Muscle. This illustration of the stylohyoid muscle is highlighted in red.
Uwe Gille, Public Domain, via Wikimedia Commons
References
Shaw SM, Martino R, Mahdi A, Sawyer FK, Mathur S, Hope A, Agur AM. Architecture of the Suprahyoid Muscles: A Volumetric Musculoaponeurotic Analysis. Journal of speech, language, and hearing research : JSLHR. 2017 Oct 17:60(10):2808-2818. doi: 10.1044/2017_JSLHR-S-16-0277. Epub [PubMed PMID: 28973130]
Ozgur Z, Govsa F, Celik S, Ozgur T. An unreported anatomical finding: unusual insertions of the stylohyoid and digastric muscles. Surgical and radiologic anatomy : SRA. 2010 Jun:32(5):513-7. doi: 10.1007/s00276-009-0553-4. Epub 2009 Sep 11 [PubMed PMID: 19763380]
Otonari-Yamamoto M, Nakajima K, Tsuji Y, Otonari T, Curtin HD, Okano T, Sano T. Imaging of the mylohyoid muscle: separation of submandibular and sublingual spaces. AJR. American journal of roentgenology. 2010 May:194(5):W431-8. doi: 10.2214/AJR.09.3516. Epub [PubMed PMID: 20410390]
Abuhaimed AK,Alvarez R,Menezes RG, Anatomy, Head and Neck, Styloid Process StatPearls. 2021 Jan; [PubMed PMID: 31082019]
Glogoff MR, Baum SM, Cheifetz I. Diagnosis and treatment of Eagle's syndrome. Journal of oral surgery (American Dental Association : 1965). 1981 Dec:39(12):941-4 [PubMed PMID: 6948095]
Level 3 (low-level) evidenceDas S, Suhaimi FH, Othman F, Latiff AA. Anomalous styloid process and its clinical implications. Bratislavske lekarske listy. 2008:109(1):31-3 [PubMed PMID: 18447260]
Gözil R, Yener N, Calgüner E, Araç M, Tunç E, Bahcelioğlu M. Morphological characteristics of styloid process evaluated by computerized axial tomography. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2001 Nov:183(6):527-35 [PubMed PMID: 11766524]
Guyuron B, Problem neck, hyoid bone, and submental myotomy. Plastic and reconstructive surgery. 1992 Nov; [PubMed PMID: 1410036]
Kay DJ, Har-El G, Lucente FE. A complete stylohyoid bone with a stylohyoid joint. American journal of otolaryngology. 2001 Sep-Oct:22(5):358-61 [PubMed PMID: 11562889]
Level 3 (low-level) evidenceTakezawa K, Townsend G, Ghabriel M. The facial nerve: anatomy and associated disorders for oral health professionals. Odontology. 2018 Apr:106(2):103-116. doi: 10.1007/s10266-017-0330-5. Epub 2017 Dec 14 [PubMed PMID: 29243182]
Piagkou M, Anagnostopoulou S, Kouladouros K, Piagkos G. Eagle's syndrome: a review of the literature. Clinical anatomy (New York, N.Y.). 2009 Jul:22(5):545-58. doi: 10.1002/ca.20804. Epub [PubMed PMID: 19418452]
Monteagudo PT, Rossinol VL, do Nascimento Verreschi IT, Dias-da-Silva MR. Stylohyoid Ligament Calcification: A Greater-Than-Expected Cause of Otalgia in Turner Syndrome. Journal of the Endocrine Society. 2019 Jul 1:3(7):1403-1408. doi: 10.1210/js.2019-00009. Epub 2019 May 23 [PubMed PMID: 31286106]
Demirtaş H, Kayan M, Koyuncuoğlu HR, Çelik AO, Kara M, Şengeze N. Eagle Syndrome Causing Vascular Compression with Cervical Rotation: Case Report. Polish journal of radiology. 2016:81():277-80. doi: 10.12659/PJR.896741. Epub 2016 Jun 13 [PubMed PMID: 27354882]
Level 3 (low-level) evidenceSeçil Y, Aydogdu I, Ertekin C. Peripheral facial palsy and dysfunction of the oropharynx. Journal of neurology, neurosurgery, and psychiatry. 2002 Mar:72(3):391-3 [PubMed PMID: 11861704]
Bokhari MR, Graham C, Mohseni M. Eagle Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 28613540]