Introduction
The corpus albicans, simply put, is a scar on the surface of the ovary that is a remnant of ovulation.[1] Before degeneration into scar tissue, the corpus albicans was once a thriving endocrine organ called the corpus luteum that functioned to maintain the growing fetus. This activity will examine the structure and function of the normal ovary and its ovulatory function to understand the significance of the corpus albicans itself, which will be followed by a look into the clinical implications of this structure.
Structure
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure
Ovarian structure:
To understand the structure of the corpus albicans, one must first understand the general structure of the ovary itself. The structure of the ovary is made up of three different regions: the cortex, medulla, and hilum. The cortex of the ovary contains two major types of cells, follicular cells, and stromal cells. The cortex also contains the corpora lutea as well as the remnant corpora albicans. The medulla is made up of blood vessels and nerves, and the hilum contains major blood vessels to the ovary.[2]
Corpus luteum structure:
When the formation of the corpus albicans begins, there is a tissue reorganization process that develops. The corpus albicans comes from a precursor endocrine organ called the corpus luteum. As the corpus luteum degenerates, there is an influx of matrix metalloproteinases, fibroblasts, and macrophages that take over the process of both organizations of dense connective tissue of the newly forming corpus albicans, as well as cellular cleanup needed after extensive apoptosis.[3] On histology, the freshly formed corpus luteum will appear as a nodule of dense connective tissue.[2]
Function
The ovulatory cycle:
Understanding the role of the corpus albicans requires first exploring the basics of the ovulatory cycle itself. The ovulatory cycle, or menstrual cycle, average 28 days in length and consists of two ovarian phases: the follicular phase and the luteal phase. The structure of the menstrual cycle (ranging from 26 to 35 days) begins with 5 days of menstruation followed by the remaining 9 days of the follicular phase, then followed by the 14 days of the luteal phase.[4] This cycle begins at the onset of the reproductive years, termed menarche and continues until the end of the reproductive years, termed menopause.[5]
Follicular phase:
The follicular phase lasts fourteen days and starts on the first day of menses and continues until the day of ovulation. The luteal phase, which also lasts 14 days, then follows from ovulation until the day before the beginning of menses. These phases are responsible for producing a viable egg and preparing the endometrium for implantation, respectively. During the follicular phase, the follicle grows and develops under the influence of surrounding stromal cells called granulosa and thecal cells. As the luteinizing hormone (LH) surge reaches its peak, the follicle ruptures and releases a single developed oocyte.
Luteal phase:
The portion of the follicle remaining in the ovary after ovulation will become the corpus luteum. This process is called luteinization. The cells making up the corpus luteum are granulosa cells, thecal cells, and contributing blood vessels. These granulosa cells go on to produce progesterone and estradiol, whereas thecal cells have the job of making androstenedione. The luteal phase will experience one of two outcomes; either an oocyte will be fertilized and implanted into the uterus, or menses will begin. If fertilization occurs, the corpus luteum is responsible for maintaining the endometrium with the production of progesterone and no corpus albicans will be formed. This maintenance of the corpus luteum initiates by the hormone human chorionic gonadotropin (HCG) produced by the implanting trophoblast which will begin production around day 8 after fertilization.[4] If fertilization does not take place, the corpus luteum will then undergo a process termed luteolysis around eight days after ovulation.
Luteolysis:
The first sign of formation of the corpus albicans is with shrinkage of the granulosa cells within the corpus luteum, followed by apoptosis. This process gets explicitly triggered by uterine prostaglandin F2alpha, which ensures that both the corpus luteum will undergo both structural and hormonal degradation.[6] This tissue of the former corpus luteum has now termed the corpus albicans and is seen histologically as a dense connective tissue aggregate.[2] This degradation of the corpus luteum will, in turn, cause the onset of menstruation and the beginning of a new ovulatory cycle. This cycle will continue monthly until the decline of the female's reproductive years, ultimately ending with cessation of ovulatory function, termed menopause.[7]
Microscopy, Light
Under light microscopy, the corpus albicans will frequently be found in the post-menopausal ovary signifying prior ovulatory events.[8] The structure will appear as an aggregate of dense connective tissue.[2] This aspect is the remnant of that of the corpus luteum, which is about 2 cm of diameter, yellow and lobulated with a cystic center.
Clinical Significance
Luteal phase deficiency:
Luteal phase deficiency is defined as a decreased lifespan of the corpus luteum and thus causes the premature formation of the corpus albicans. Normally the corpus luteum has a lifespan of eleven to fourteen days, but in a luteal phase defect the corpus luteum functions for less than nine days. Typically this deficiency is caused by a lack of the proper progesterone levels that are responsible for maintenance of the corpus luteum. Clinically, this deficiency can be a cause for recurrent early pregnancy loss. The past diagnostic gold standard for a luteal phase defect was a luteal phase biopsy; however, the medical community has decided its imprecision makes it no longer clinically relevant. Treatment can include progesterone supplementation.[9]
Corpus Albicans calcification:
The corpus albicans is infrequently visible on clinical imaging. However, in post-menopausal women, sometimes the corpus albicans can have an abnormal appearance due to the menopausal related hormonal changes. A decrease in estrogen and a decrease in both immune-mediated phagocytic and fibroblastic activity can lead to poor formation and regression of the corpus albicans; this can lead to ultrasound detection of these structures and possible confusion with ovarian neoplasms. Both hemosiderin and calcium deposition within the structure of the corpus albicans itself can lead to increased ultrasound detection. They appear as small echogenic foci without distal acoustic shadowing. In addition to ultrasound, these calcifications can also show up in plain film radiographs of the pelvis.[10]
Media
(Click Image to Enlarge)
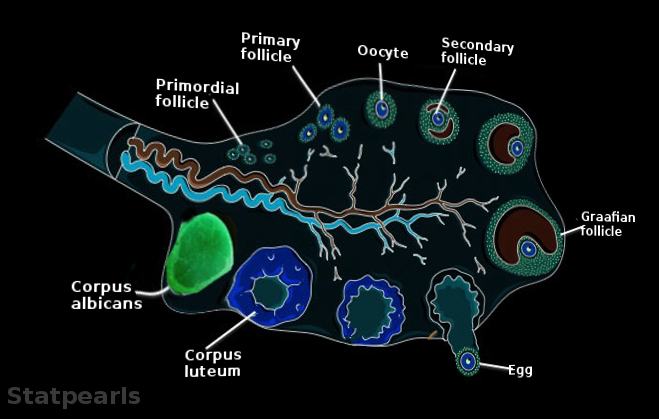
Corpus albicans Image courtesy Statpearls
References
Oliver R, Pillarisetty LS. Anatomy, Abdomen and Pelvis, Ovary Corpus Luteum. StatPearls. 2023 Jan:(): [PubMed PMID: 30969526]
Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, New M, Purnell J, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Williams CJ, Erickson GF. Morphology and Physiology of the Ovary. Endotext. 2000:(): [PubMed PMID: 25905186]
Duncan WC. The human corpus luteum: remodelling during luteolysis and maternal recognition of pregnancy. Reviews of reproduction. 2000 Jan:5(1):12-7 [PubMed PMID: 10711731]
Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Animal reproduction science. 2011 Apr:124(3-4):229-36. doi: 10.1016/j.anireprosci.2010.08.030. Epub 2010 Sep 3 [PubMed PMID: 20869180]
Level 3 (low-level) evidencePerheentupa A, Huhtaniemi I. Aging of the human ovary and testis. Molecular and cellular endocrinology. 2009 Feb 5:299(1):2-13. doi: 10.1016/j.mce.2008.11.004. Epub 2008 Nov 18 [PubMed PMID: 19059459]
Galvão AM, Skarzynski D, Ferreira-Dias G. Luteolysis and the Auto-, Paracrine Role of Cytokines From Tumor Necrosis Factor α and Transforming Growth Factor β Superfamilies. Vitamins and hormones. 2018:107():287-315. doi: 10.1016/bs.vh.2018.01.001. Epub 2018 Feb 9 [PubMed PMID: 29544635]
Rojas J, Chávez-Castillo M, Olivar LC, Calvo M, Mejías J, Rojas M, Morillo J, Bermúdez V. Physiologic Course of Female Reproductive Function: A Molecular Look into the Prologue of Life. Journal of pregnancy. 2015:2015():715735. doi: 10.1155/2015/715735. Epub 2015 Dec 1 [PubMed PMID: 26697222]
Hariri LP, Bonnema GT, Schmidt K, Winkler AM, Korde V, Hatch KD, Davis JR, Brewer MA, Barton JK. Laparoscopic optical coherence tomography imaging of human ovarian cancer. Gynecologic oncology. 2009 Aug:114(2):188-94. doi: 10.1016/j.ygyno.2009.05.014. Epub 2009 May 29 [PubMed PMID: 19481241]
Mesen TB, Young SL. Progesterone and the luteal phase: a requisite to reproduction. Obstetrics and gynecology clinics of North America. 2015 Mar:42(1):135-51. doi: 10.1016/j.ogc.2014.10.003. Epub 2015 Jan 5 [PubMed PMID: 25681845]
Millet J, Much M, Gunabushanam G, Buza N, Schwartz PE, Scoutt LM. Large ovarian calcifications from an unresorbed corpus albicans. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2012 Sep:31(9):1465-8 [PubMed PMID: 22922629]
Level 3 (low-level) evidence