
 Anatomy, Head and Neck, Sphenopalatine Foramen
Anatomy, Head and Neck, Sphenopalatine Foramen
Introduction
The sphenopalatine foramen (SPF) represents an opening on the lateral nasal wall that is present at the articulation between the superior aspect of the vertical portion of the palatine bone and the inferior projection of the sphenoid bone.[1] The sphenopalatine foramen connects the nasal cavity to the pterygopalatine fossa of the skull and houses the sphenopalatine artery (SPA) and vein, the posterior superior lateral nasal nerve, and the nasopalatine nerves.[2][3][2] Moreover, the sphenopalatine foramen provides an important anatomical landmark for those who perform procedures where knowledge of the sphenopalatine foramen and its contents remains critical, including the creation of a nasoseptal flap for nasal reconstruction or skull base repairs, posterior epistaxis control, and functional endoscopic sinonasal surgery. Herein we discuss the anatomy of the sphenopalatine foramen, including its structure, function, contents, embryology, anatomical variations, and clinical relevance.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Boundaries of the sphenopalatine foramen[4]:
- Superiorly: the body of the sphenoid
- Anteriorly: the orbital process of the palatine bone.
- Posteriorly: the sphenoidal process of the palatine bone.
- Inferiorly: the perpendicular plate of the palatine bone.
The foramen can be found at the posterior-superior-medial corner of the maxillary sinus, just deep to the attachment of the middle turbinate, but exists in a variety of locations:
- Class I (35 to 82%): the opening is purely into the superior meatus (e.g., above the middle turbinate)
- Class II (15 to 56%): opening spans the ethmoidal crest (e.g., at the transition of the middle and superior meatus)
- Class III (2 to 9%): openings exist on both sides of the ethmoidal crest.
- Studies that have examined the shape of this foramen have reported that it can appear in various shapes, including square, oval, triangular, and piriform deep grooves that extend superiorly and inferiorly from the foramen.
- In adults, the sphenopalatine foramen measures roughly 6 mm and 5.5 mm in the vertical and horizontal planes, respectively.
Endoscopic landmarks for sphenopalatine foramen localization[2][9]:
- The posterior wall of the maxillary sinus: within 1 cm anterior to the sphenopalatine foramen
- Maxillary line: 3.7 cm anterior to the sphenopalatine foramen
- Anterior head of the middle turbinate: 3.4 cm anterior to the sphenopalatine foramen
- Inferior turbinate horizontal lamina: 1.3 cm inferior to the sphenopalatine foramen
- Basal lamella: 1.2 cm anterior to the sphenopalatine foramen
- Choanal arch: 0.9 cm posterior to the sphenopalatine foramen
- Nasal floor: 1.8-2.7 cm inferior to the sphenopalatine foramen
- Ethmoid crest (i.e., crista ethmoidalis): a sharp bony projection that characterizes the anterior portion of the sphenopalatine foramen
- NOTE: Females have statistically shorter distances to the sphenopalatine foramen from the nasal floor, maxillary line, choanal arch, and anterior head of the middle turbinate.
- Approximately 80 to 90% of individuals have one sphenopalatine foramen per side, while around 10 to 20% of individuals may possess an accessory sphenopalatine foramen, which is typically located anteroinferior to the sphenopalatine foramen. This arrangement is thought to be dictated by the embryologic development of the sphenopalatine artery, which can be highly variable in terms of its number of branches as well as the location of the branch points. Nevertheless, no variables or characteristics show any association with the presence of an accessory sphenopalatine foramen.
Contents of the sphenopalatine foramen[1][8][11]:
- Sphenopalatine artery (SPA) - a terminal branch of the internal maxillary artery (branch of the external carotid artery). The sphenopalatine artery is the dominant blood supply to the posterior mucosa of the nasal cavity.
- Posterior superior lateral nasal nerve - a branch of the nasopalatine nerve that provides sensory innervation to the lateral wall of the nasal cavity
- Nasopalatine nerve - a derivative of the pterygopalatine ganglion that is considered part of the parasympathetic nervous system.
Embryology
The sphenopalatine foramen forms from the fusion of the palatine bone and the sphenoid bone around the sphenopalatine artery; thus, a description of the embryology of the structures, as mentioned earlier, will provide a better understanding of the development of the sphenopalatine foramen.
- Sphenopalatine artery: Around the fourth to the fifth week of embryologic development, the aortic arch forms from the mesoderm of the first pharyngeal arch. The aortic sac that gives rise to the aortic arch then forms the maxillary artery and its subsequent branches, including the sphenopalatine artery. The branches and diameter of the sphenopalatine artery determine the number, shape, and size of the sphenopalatine foramen.[8]
- Sphenoid bone: The sphenoid bone forms from neural crest cells and first develops as the body of the sphenoid at around 7 to 8 weeks of fetal development. The body of the sphenoid is originally formed in two parts: the pre-sphenoid, otherwise known as the tuberculum sellae, which is associated with the lesser wings and the post-sphenoid, otherwise known as the sella turcica and the dorsum sellae, which is associated with the greater wings and pterygoid process. The pre-sphenoid portion begins to ossify around the ninth week of fetal development, while the post-sphenoid portion begins to ossify around the eighth week of fetal development. The pre- and post-sphenoid portions of the sphenoid bone typically fuse around the eighth month of life.[12]
- Palatine bone: The palatine bone derives from neural crest cells and forms around the ninth week of embryologic development as part of secondary palate formation.
In summary, the subsequent fusion of the palatine and sphenoid bone around the sphenopalatine artery result in the formation of the sphenopalatine foramen.[13]
Nerves
The neural contents of the sphenopalatine foramen include the posterior superior lateral nasal nerve and the nasopalatine nerve.
- Nasopalatine nerve represents a derivative of the pterygopalatine ganglion (PPG), which originates in the pterygopalatine fossa.[1][11] The pterygopalatine ganglion is the largest parasympathetic ganglion of the maxillary nerve branches. Preganglionic parasympathetic nerve fibers from the Vidian nerve carry these fibers from their source—the greater petrosal branch of facial nerve—to the pterygopalatine ganglion. The postganglionic parasympathetic fibers from this pterygopalatine ganglion provide parasympathetic innervation to the mucosal glands of the nose and assist with mucous production and maintenance of the nasal mucosa.[14] The nasopalatine nerve travels from its origin in the pterygopalatine fossa alongside the sphenopalatine artery through the sphenopalatine foramen. It then follows a descending course in a supra-periosteal plane from the posterior-superior aspect of the septum to the anterior inferior aspect of the septum, where it connects with the greater palatine nerve. This nerve provides sensory innervation to the nasal mucosa along its course.[15]
- The posterior superior lateral nasal nerve represents a branch of the nasopalatine nerve and provides sensory information to the lateral wall of the nasal cavity.
Physiologic Variants
As mentioned previously, several studies have reported that approximately 10 to 20% of individuals have an accessory sphenopalatine foramen, generally located anterior and inferior to the natural sphenopalatine foramen. This variation is thought to be due to the variable branching of the sphenopalatine artery.[8] Additionally, it merits noting that the foramina can range in size, shape, and location, as mentioned above (see STRUCTURE AND FUNCTION).[8][10]
Surgical Considerations
The sphenopalatine foramen remains an important surgical landmark for a variety of procedures. For instance, knowledge of the sphenopalatine foramen’s location is useful when performing endoscopic sinus surgery, as the sphenopalatine foramen can be infiltrated with local anesthetics and vasoconstricting agents to provide better anesthesia and hemostasis, respectively. Knowledge of the sphenopalatine foramen’s location proves particularly important when performing a nasoseptal flap for nasal reconstruction or skull base repairs, as the sphenopalatine artery represents the major blood supply to this versatile flap. Also, knowledge of the sphenopalatine foramen and its contents proves useful when performing endoscopic ligations for posterior epistaxis control where the sphenopalatine artery is targeted.
Reliable landmarks for identifying the sphenopalatine foramen have been delineated above (see Endoscopic landmarks for sphenopalatine foramen localization), though landmarks often used during surgery include the posterior portion of the middle turbinate and the ethmoid crest (i.e., crista ethmoidalis). During endoscopic sinus surgery, an incision can be made 1 cm anterior to the posterior aspect of the middle turbinate, and a mucoperiosteal flap can be raised posteriorly to identify the ethmoid crest. The sphenopalatine foramen and its contents should be located posterior to this landmark in over 95% of cases, allowing for the safe identification and/or preservation of the contents of the sphenopalatine foramen.[15][16][9]
Clinical Significance
The sphenopalatine foramen provides an essential anatomical landmark for multiple surgical procedures of the head and neck, including the creation of a nasoseptal flap for nasal reconstruction or skull base repairs, posterior epistaxis control, and functional endoscopic sinonasal surgery. Sound knowledge of the sphenopalatine foramen anatomy, including its structure, function, contents, and anatomical variations, is required to optimize success when performing such procedures.
Media
(Click Image to Enlarge)
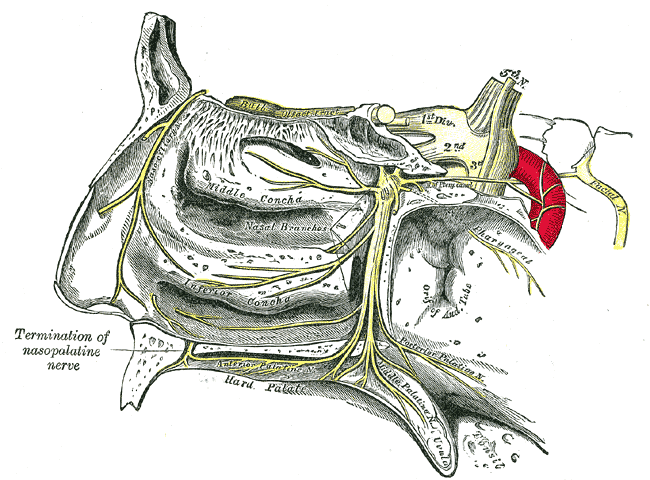
Trigeminal Nerve, Nasopalatine Distribution. This image illustrates the course of the trigeminal nerve in the nasopalatine region, highlighting the termination of the nasopalatine nerve, the sphenopalatine ganglion, and its branches.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
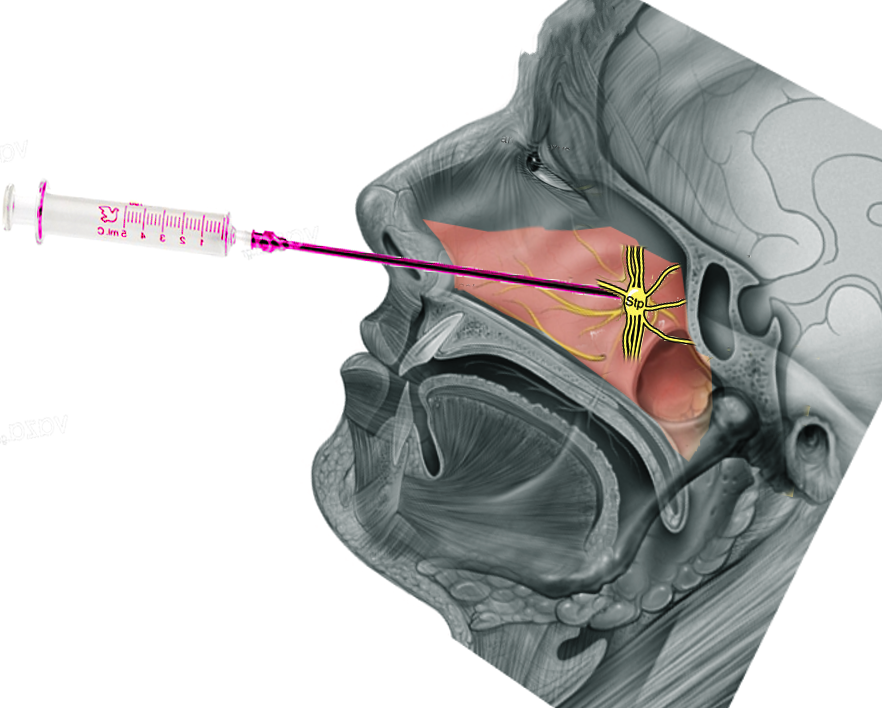
sphenopalatine ganglion Image courtesy S Bhimji MD
(Click Image to Enlarge)
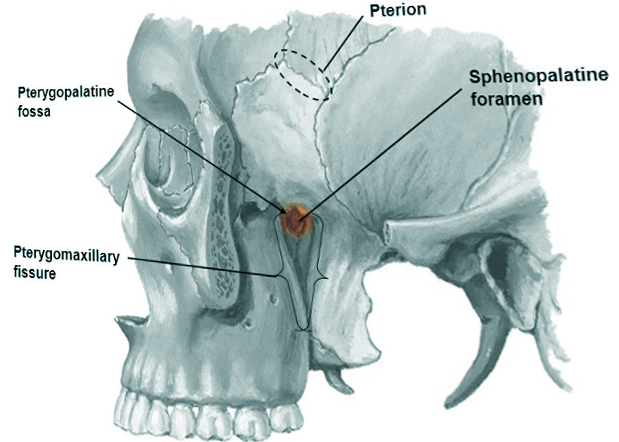
Sphenopalatine foramen Image courtesy S Bhimji MD
(Click Image to Enlarge)
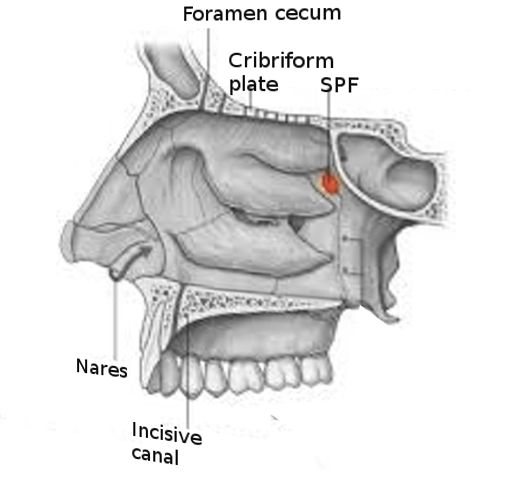
Sphenopalatine foramen Image courtesy S Bhimji MD
References
Kim JH, Oka K, Jin ZW, Murakami G, Rodríguez-Vázquez JF, Ahn SW, Hwang HP. Fetal Development of the Incisive Canal, Especially of the Delayed Closure Due to the Nasopalatine Duct: A Study Using Serial Sections of Human Fetuses. Anatomical record (Hoboken, N.J. : 2007). 2017 Jun:300(6):1093-1103. doi: 10.1002/ar.23521. Epub 2017 Jan 27 [PubMed PMID: 27860365]
Pothier DD, Mackeith S, Youngs R. Sphenopalatine artery ligation: technical note. The Journal of laryngology and otology. 2005 Oct:119(10):810-2 [PubMed PMID: 16259659]
Gao L, Zhou L, Dai Z, Huang X. The Endoscopic Prelacrimal Recess Approach to the Pterygopalatine Fossa and Infratemporal Fossa. The Journal of craniofacial surgery. 2017 Sep:28(6):1589-1593. doi: 10.1097/SCS.0000000000003419. Epub [PubMed PMID: 28863111]
Prades JM, Asanau A, Timoshenko AP, Faye MB, Martin Ch. Surgical anatomy of the sphenopalatine foramen and its arterial content. Surgical and radiologic anatomy : SRA. 2008 Oct:30(7):583-7. doi: 10.1007/s00276-008-0390-x. Epub 2008 Jul 23 [PubMed PMID: 18648719]
Wentges RT, Surgical anatomy of the pterygopalatine fossa. The Journal of laryngology and otology. 1975 Jan; [PubMed PMID: 1113030]
Wareing MJ, Padgham ND. Osteologic classification of the sphenopalatine foramen. The Laryngoscope. 1998 Jan:108(1 Pt 1):125-7 [PubMed PMID: 9432081]
Scanavine AB, Navarro JA, Megale SR, Anselmo-Lima WT. Anatomical study of the sphenopalatine foramen. Brazilian journal of otorhinolaryngology. 2009 Jan-Feb:75(1):37-41 [PubMed PMID: 19488558]
El-Shaarawy EAA, Hassan SS. The sphenopalatine foramen in man: anatomical, radiological and endoscopic study. Folia morphologica. 2018:77(2):345-355. doi: 10.5603/FM.a2017.0104. Epub 2017 Nov 13 [PubMed PMID: 29131280]
Saraceni Neto P, Nunes LM, Caparroz FA, Gregorio LL, de Souza RP, Simões JC, Kosugi EM. Resection of the ethmoidal crest in sphenopalatine artery surgery. International forum of allergy & rhinology. 2017 Jan:7(1):87-90. doi: 10.1002/alr.21832. Epub 2016 Aug 11 [PubMed PMID: 27513601]
Pádua FG, Voegels RL. Severe posterior epistaxis-endoscopic surgical anatomy. The Laryngoscope. 2008 Jan:118(1):156-61 [PubMed PMID: 18025950]
Demiralp KÖ, Kurşun-Çakmak EŞ, Bayrak S, Sahin O, Atakan C, Orhan K. Evaluation of Anatomical and Volumetric Characteristics of the Nasopalatine Canal in Anterior Dentate and Edentulous Individuals: A CBCT Study. Implant dentistry. 2018 Aug:27(4):474-479. doi: 10.1097/ID.0000000000000794. Epub [PubMed PMID: 30028392]
Catala M. [Embryology of the sphenoid bone]. Journal of neuroradiology = Journal de neuroradiologie. 2003 Sep:30(4):196-200 [PubMed PMID: 14566186]
BURDI AR. SAGITTAL GROWTH OF THE NASOMAXILLARY COMPLEX DURING THE SECOND TRIMESTER OF HUMAN PRENATAL DEVELOPMENT. Journal of dental research. 1965 Jan-Feb:44():112-25 [PubMed PMID: 14245486]
Konno A, Togawa K. Role of the vidian nerve in nasal allergy. The Annals of otology, rhinology, and laryngology. 1979 Mar-Apr:88(2 Pt 1):258-66 [PubMed PMID: 443720]
Honkura Y, Nomura K, Oshima H, Takata Y, Hidaka H, Katori Y. Bilateral endoscopic endonasal marsupialization of nasopalatine duct cyst. Clinics and practice. 2015 Jan 28:5(1):748. doi: 10.4081/cp.2015.748. Epub 2015 Feb 5 [PubMed PMID: 25918636]
Eordogh M, Grimm A, Gawish I, Patonay L, Reisch R, Briner HR, Baksa G. Anatomy of the sphenopalatine artery and its implications for transnasal neurosurgery. Rhinology. 2018 Mar 1:56(1):82-88. doi: 10.4193/Rhin17.181. Epub [PubMed PMID: 29166425]